Ashokrao Mane College of Pharmacy, Peth- Vadgaon/ Shivaji university 416112, Maharashtra, India
Materials in the nanoscale range are used as diagnostic instruments or to deliver therapeutic compounds to specific targeted regions in a controlled manner in the relatively new but quickly evolving fields of nanomedicine and nano delivery systems. Through the site-specific and target-oriented administration of precise medications, nanotechnology provides numerous advantages in the treatment of chronic human diseases. Chemotherapeutic drugs, biological agents, immunotherapeutic agents, and other nanomedicine applications have shown remarkable promise in the treatment of a variety of illnesses in recent years.
The study of materials' distinctive characteristics between 1 and 100 nm is known as nanoscience, and the use of this knowledge to produce or alter new products is known as nanotechnology. Nanomaterials are made possible by the ability to work with structures at the atomic level [1,2]. Nanomaterials can be applied in a variety of industries, including electronics and filmmaking, because of their special optical, electrical, and/or magnetic characteristics at the nanoscale. Because they have a high surface area to volume ratio, nanomaterials are special [3]. By using nanostructures and nanophases in a variety of scientific domains, nanotechnology has been demonstrated to overcome the divide between the biological and physical sciences [4,5]. particularly in nanomedicine and nano-based drug delivery systems, where these particles are of great importance [6]. Needless to add, the development and use of the tiniest particles, which are invisible to the naked sight, are not new developments. Examples of the earlier usage of nanomaterials comprise the well-known Damascene Swords, many late medieval church windows, and the Lycurgus Cup from the fourth century AD. on exhibit at the British Museum in London. When viewed from the outside, the antique Roman cup seems olive green, but when viewed from the interior, it becomes purple, showing a famous monarch [7]. Author K. Eric Drexler described how to construct intricate machines from individual atoms that can autonomously control molecules and atoms to manufacture things and replicate themselves in his first and most controversial book on nanotechnology, "The Coming Era of Nanotechnology"[8]. K. Eric Drexler, Chris Peterson, and Gayle Pergamit describe the possible applications of such "nanobots" or "assemblers" in the medical domain in their book Unbounding the Future. According to reports in the 1991 book "The Nanotechnology Revolution," the word "nanomedicine" was first introduced. "[9]. At the beginning of the 20th century, Paul Ehrlich tried to develop "magic bullets" that could be used to target illnesses and eliminate all germs with a single therapy. He developed Salvarsan, which is regarded as the first drug of this type with precise action and the forerunner of chemotherapy [10].
Table 1. Issues with conventional drug delivery and corresponding nanotechnology-based solutions
|
Issue with Traditional Delivery |
Nanotechnology-Based Solution |
|
Low bioavailability |
Improved absorption and extended circulation (polymeric nanoparticles, lipid-based carriers) |
|
Fast metabolism & clearance |
Sustained and controlled release systems |
|
Poor patient compliance |
Controlled release → decreased dosing frequency |
|
Non-specific toxicity |
Targeted delivery via ligands, antibodies, or EPR effect |
|
Poor aqueous solubility |
Nano-formulations (nanocrystals, liposomes, micelles) enhance solubility |
Need Of Nanotechnology in Medicine
Full-scale development of a possible medication candidate is frequently rejected due to safety or efficacy concerns involving inadequate solubility, poor permeability, poor bioavailability, and degradability by gastric acid. Hydrophobic medications are stabilized by nano-based drug delivery, which also enhances biodistribution and dissolution rate, leading to increased efficacy [11]. Lipid polymers are encapsulated and dispersed within a matrix to preserve medications from degradation in nano delivery systems. Furthermore, the medications can accumulate in the targeted location, such as tumors, inflammatory cells, or infectious cells, thanks to an improved permeability and retention effect [12]. Other potential advantages of nanotechnology include reduced toxicity to non-target cells due to the use of biocompatible nanoparticles, regulated drug release with less drug demand, and fewer side effects as a result of preferred accumulation at target areas [13].
Targeted medication delivery components
Nanoparticles Used in Drug Delivery
Treatments for cancer have made extensive use of nano-carriers, including liposomes, micelles, dendritic macromolecules, quantum dots, carbon nanotubes, and metal-based NPs.
Table 2. Overview of different nanocarriers, their mechanisms, advantages, limitations, and applications.
|
Nanocarrier |
Description (Size & Mechanism) |
Key Advantages |
Major Limitations |
Representative Application |
|
Liposomes |
50–200 nm; spherical vesicles encapsulating both hydrophilic and lipophilic drugs |
Biocompatible; several FDA-approved formulations |
Prone to instability; high cost of production |
Doxil (liposomal doxorubicin for cancer therapy) |
|
Polymeric nanoparticles |
10–1000 nm; release drugs through a polymeric matrix |
Adjustable properties; enable sustained release |
Possible polymer-related toxicity |
Gene delivery systems |
|
Solid lipid nanoparticles (SLNs) |
50–500 nm; solid lipid core used for drug entrapment |
Provide stability; allow controlled drug release |
Limited drug loading capacity |
Anticancer formulations |
|
Nanostructured lipid carriers (NLCs) |
50–600 nm; blend of solid and liquid lipids for drug incorporation |
Enhanced drug loading and improved release profiles |
Challenges in large-scale production |
Topical and dermal drug delivery |
|
Dendrimers |
2–20 nm; branched, tree-like polymers with high surface functionality |
High drug loading potential; suitable for targeting |
Complex and costly synthesis |
Investigated in antiviral therapy |
|
Metallic nanoparticles |
10–100 nm; gold, silver, iron oxide nanoparticles modified for targeting |
Combine imaging and therapeutic functions |
Toxicity and biocompatibility concerns |
Gold nanoparticles in photothermal cancer therapy |
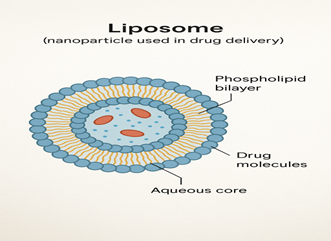
Liposomes
Phospholipid bilayers make up liposomes, which are spherical vesicles with a diameter of 30 nm to several microns. Because of their structure, Drugs that are hydrophilic can be added to the aqua core, whereas drugs that are hydrophobic can be added to the lipid bilayer. Drugs that are hydrophilic can be added to the aqua core, whereas drugs that are hydrophobic can be added to the lipid bilayer. Their ability to target is improved by surface modification using polymers, proteins, or antibodies. In cancer treatment, liposomes have proven especially effective, exhibiting enhanced drug distribution and less systemic toxicity [15].
Micelles
Amphiphilic molecules make up micelles, which self-assemble in aquatic settings to create structures with sizes between 10 and 100 nm. Drugs that are poorly soluble in water can be encapsulated thanks to their architecture, which has an inner core that is hydrophobic and an exterior shell that is hydrophilic. This unique structure enhances the medicines' solubility and bioavailability. Micelles exhibit adaptability in therapeutic settings, acting as delivery systems for a range of substances, such as medications, imaging agents, and diagnostic markers[16].

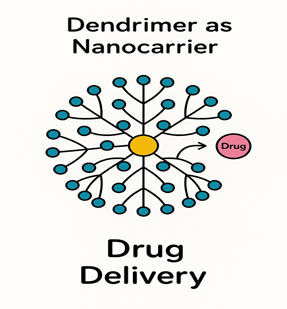
Dendrimers
Dndrimers are tree-like, extremely branched macromolecules that extend from a central core and have well regulated architectures. Several functional surface groups with their distinctive architecture can be altered for certain therapeutic uses. Drug encapsulation is made possible by the internal cavities, while conjugation with targeted ligands is made possible by the surface groups. Dendrimers have remarkable control over surface chemistry, size, and form[17].
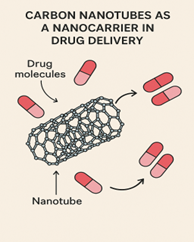
Carbon Nanotubes
Carbon nanotubes are made up of cylindrical graphene sheets that might have one or more walls. High drug loading capacity is made possible by their remarkable surface area-to-volume ratio, and a variety of medicinal compounds can be accommodated in their hollow interior. Their targeting and biocompatibility are improved by surface functionalization. These structures show great promise for tissue engineering and diagnostic applications. They are especially useful for intracellular drug delivery because of their capacity to pass through cell membranes [18].
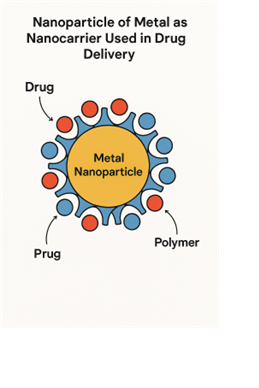
Nanoparticles of metal
Metallic nanoparticles, especially those made of iron oxide and gold, have special qualities for medication delivery. Hydrophilic polymers like dextran or polyethylene glycol envelop a magnetic core (4-5 nm) in iron oxide nanoparticles. These particles allow for magnetic targeting and have potential uses in imaging and medicinal administration. Excellent biocompatibility and ease of functionalization for targeted applications are two features of gold nanoparticles [19].
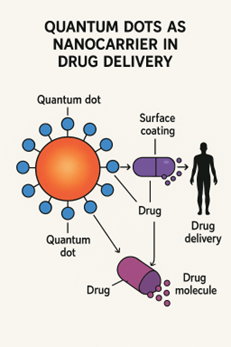
Quantum dots
Fluorescent semiconductor nanocrystals with a size range of 1–100 nm are known as quantum dots. They are useful for both imaging and drug delivery applications because of their remarkable optical qualities. Because of their fluorescent qualities, these nanostructures can be altered to deliver medicinal substances and offer real-time tracking capabilities [20].
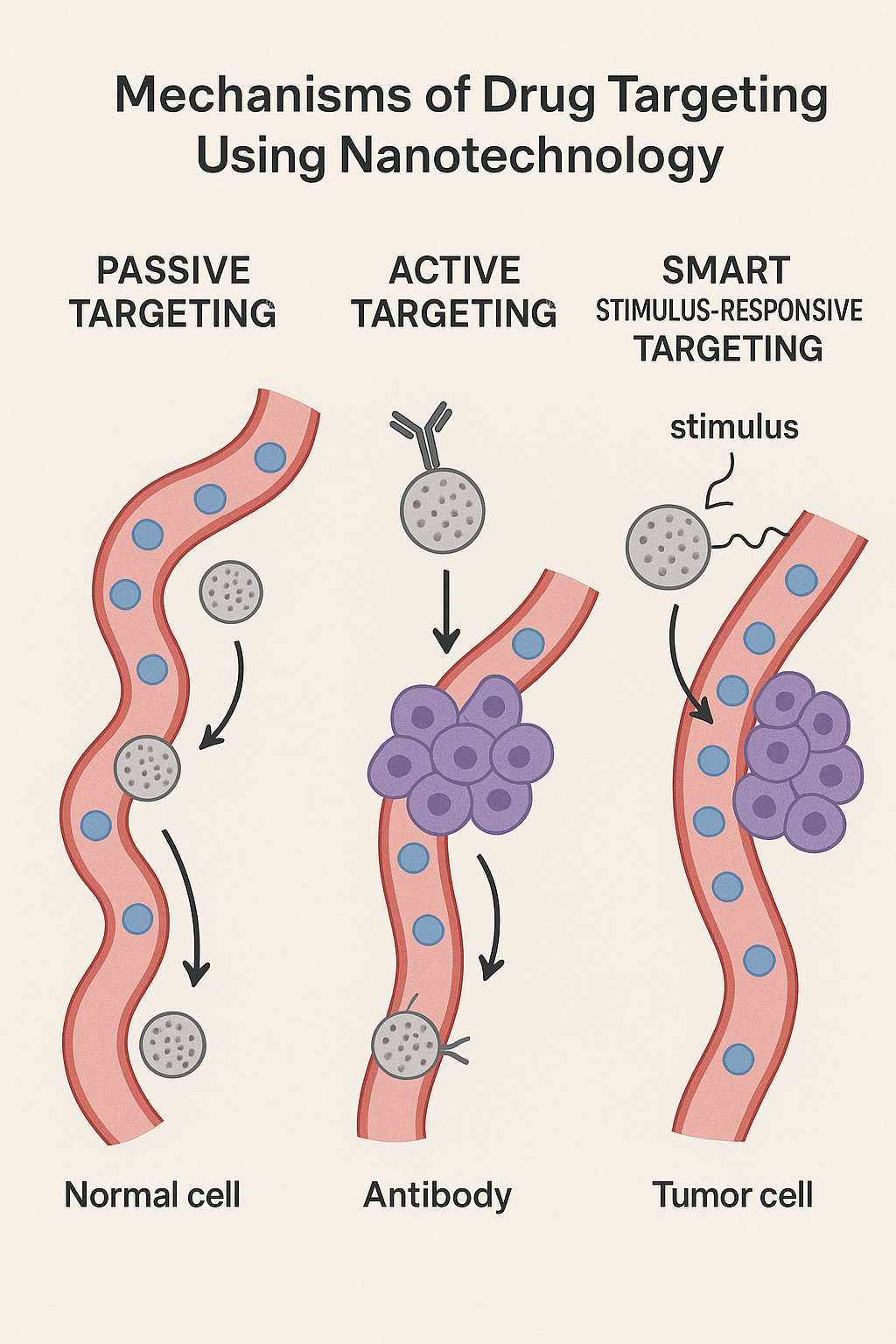
Mechanisms of Drug Targeting Using Nanotechnology
The distribution of therapeutic substances to the site of action has been completely transformed by nanotechnology in drug delivery systems. In order to improve therapeutic efficacy and lower systemic toxicity, medication targeting aims to deliver a treatment selectively to sick cells or tissues while limiting exposure to healthy areas. Three primary targeting strategies are identified in nanomedicine: stimuli-responsive (smart), active, and passive targeting [21].
Targeting Passively
The Enhanced Permeability and Retention (EPR) effect, a hallmark of solid tumors and inflammatory tissues, is the basis for passive targeting. Wide endothelial gaps in tumors make the aberrant vasculature extremely permeable, and lymphatic drainage is underdeveloped. This leads to the preferential accumulation and retention of nanoparticles between 10 and 200 nm in the interstitial spaces of tumors.
Doxil®, a pegylated liposomal formulation of doxorubicin, is a well-known example of passive targeting. It passively builds up in tumor tissues by the EPR effect. This method is also used in polymeric micelles made for hydrophobic anticancer medications. Although passive targeting has the benefit of being straightforward and requiring no surface alterations, it is constrained by the diversity of the EPR effect among people and tumors as well as the heterogeneity of tumor vasculature[22].
2. Active Targeting:
Active targeting is the process of functionalizing nanocarriers with particular ligands that can identify and bind to receptors or antigens that are overexpressed on diseased cells; after binding, drug-loaded nanoparticles are internalized through receptor-mediated endocytosis, improving intracellular drug accumulation at the target site. For example, trastuzumab-conjugated nanoparticles are directed against HER2 receptors in breast cancer, while folate-conjugated nanoparticles preferentially target folate receptors overexpressed in ovarian and breast cancers. This approach greatly improves therapeutic specificity and lowers off-target toxicity, but it neces intricate formulation strategies and may be impacted by interpatient variability in receptor expression[23].
3. Smart Stimulus-Responsive Targeting
In order to provide precise spatiotemporal control over medication release, Sensitive nanocarriers, also known as smart delivery systems, are designed to release their payload in response to certain external or internal stimuli.[24].
- Among the internal stimuli are: o pH-sensitive systems, which take use of the endosomal/lysosomal compartments (pH ~5) or the acidic tumor microenvironment (pH ~6.5–6.8).
- Enzyme-sensitive systems, which react to overexpressed enzymes in tumors, such as matrix metalloproteinases.
- Redox-sensitive mechanisms, which release drugs in response to the elevated intracellular glutathione (GSH) levels in cancer cells.
- A few examples of external stimuli are: o Temperature-sensitive systems, which release medications at high temperatures. One example undergoing clinical research is ThermoDox®, a heat-sensitive liposomal version of doxorubicin.
- Usually made of superparamagnetic iron oxide, magnetic-responsive nanoparticles can be steered by external magnetic fields and activated to release medications when magnetic induction occurs.
- Systems that respond to light and ultrasound, in which sound waves or radiation trigger the release of a medication. The benefit of stimuli-responsive administration is site-specific, on-demand medication release, which reduces systemic exposure. Practical difficulties are presented by the need for exact nanocarrier design and, occasionally, specific tools for external triggers [25].
Advantages and Disadvantages of Nanotechnology in Drug Delivery
Advantages of nanotechnology:
Disadvantages of nanotechnology:
Limitations & Challenges
Drug delivery could be revolutionized by nanotechnology, which makes focused, regulated, and effective therapeutic treatments possible. Nevertheless, a number of restrictions and difficulties remain limit its therapeutic use in spite of these benefits. These problems include large-scale manufacturing, physicochemical stability, economic viability, toxicological concerns, and ethical and legal obstacles. For nanomedicines to successfully transition from the bench to the bedside, these issues must be resolved[34].
Concerns about Toxicity
The possibility of toxicity from nanoparticles is one of the most important problems in nanomedicine. Because of their distinct physicochemical characteristics—such as their enormous surface area-to-volume ratio, changed surface reactivity, and nanoscale size—nanoparticles differ from traditional medications and may result in unanticipated biological interactions[35].
• Organ toxicity and bioaccumulation: Metallic nanoparticles (such as silver, gold, and iron oxide) have a low biodegradability and can accumulate in the liver, spleen, kidneys, and lungs, raising concerns about long-term toxicity and organ dysfunction[36].
• Immunotoxicity: When surface coatings (polymers, surfactants) interact with immune cells, some nanoparticles may cause immunological reactions or hypersensitivity reactions. For example, liposomal formulations have been observed to cause complement activation-related pseudoallergy (CARPA)[37].
• Genotoxicity and Cytotoxicity: Reactive oxygen species (ROS) can be produced by certain nanocarriers, particularly carbon-based ones (fullerenes, carbon nanotubes), which might result in oxidative stress, DNA damage, or apoptosis[38].
• Knowledge Gaps: Long-term toxicological studies are still lacking, and current preclinical models do not accurately mimic human physiology. Clinical acceptability and regulatory approval are delayed by this absence of thorough safety data[39].
2. Problems with Stability and Storage
Because of their intrinsic propensity for chemical and physical instability, nanoparticles may not be as safe or effective as they could be[40].
• Physical instability: During storage or transit, nanoparticles may aggregate, precipitate, or silt, changing their size and decreasing their ability to target[41].
• Chemical instability: Particularly in delicate formulations like liposomes or polymeric micelles, drug leakage, oxidation, or hydrolysis of encapsulated compounds may transpire[42].
• Shelf-Life Limitations: Distribution of many nanomedicines is difficult due to their strict storage requirements, which include low temperatures, light protection, or inert atmospheres[43].
• Sterility and Contamination: Because of their tiny size and surface activity, nanoparticles are susceptible to microbial contamination, and maintaining sterility without sacrificing formulation integrity can be challenging[44].
• Manufacturing Reproducibility: Batch-to-batch variability results from the technical demands of maintaining constant particle size distribution, surface charge, and morphology at an industrial scale[45].
3. Expensive production and scalability costs
The high production costs and difficulties in scaling up laboratory processes to industrial levels are the main obstacles to the commercialization of nanomedicines.
• Advanced Techniques: Techniques like microfluidics, supercritical fluid technology, and high-pressure homogenization call for specific tools and knowledgeable staff[46].
• Costs of Raw Materials: Lipids, ligands, surfactants, and high-purity polymers are frequently costly when employed to produce nanoparticles[47].
• Functionalization of the Surface: Production costs are further raised by including stimuli-responsive components or targeting ligands (antibodies, peptides, or aptamers)[48].
• Economic Barriers: Nanomedicines are far more costly than traditional oral or injectable formulations, which restricts their availability in low- and middle-income nations[49].
• Scale-Up Problems: Mass manufacturing and commercialization are hampered by the fact that many nanocarriers exhibit good performance at the laboratory scale but lack the same quality and reproducibility at the industrial scale[50].
4. Ethical and Regulatory Difficulties
Since nanoparticles frequently do not fit cleanly into the current frameworks for medication approval, regulation of nanomedicine is a significant bottleneck[51].
• Absence of standardized protocols:
Pharmacokinetics and biodistribution are influenced by the size, shape, surface chemistry, and charge of nanoparticles. It is not possible to capture these subtleties with standard pharmacological evaluation techniques[52].
• Quality Control: Nanocarrier characterisation may not be possible with traditional analytical methods. Development takes longer because regulatory bodies require exacting information on zeta potential, drug release kinetics, particle size distribution, and long-term safety[53].
• Ethical Concerns: There are ethical questions because of the possibility of unanticipated toxicity, long-term bioaccumulation, and unclear impacts on future generations. Furthermore, because of the dangers to human safety, conducting clinical trials for nanomedicines necessitates stringent ethical oversight[54].
• Accessibility and Intellectual Property: Big pharmaceutical companies' patenting of nanotechnologies may impede innovation and worldwide accessibility, posing socio-ethical concerns[55].
5. Bench and Bedside Translational Gap
Only a small number of nanomedicine formulations—such as Doxil®, Abraxane®, and Onivyde®—have received FDA approval, despite the fact that thousands of them have been documented in studies. The cause of this "translational gap" is:
• Predicting clinical performance from preclinical models is challenging.
• Variability in patient response brought on by variations in receptor expression or tumor physiology.
• Clinical studies have lengthy schedules and substantial expenses[56].
Recent Advances & Future Perspectives
Over the past few decades, research on nanotechnology has increased dramatically, and the healthcare sector has also attracted more attention. Advances in technology have improved our understanding of some of the intricate etiologists at play, raised the possibility of early detection, and expanded the potential therapeutic applications of nanomedicine. Although they have only been partially implemented and integrated, many nano systems have demonstrated success in lowering obstacles in various healthcare domains. While research on nanomedicines and nanodevices is still in its early stages, one strategy to speed up this process is to focus on creating novel ways to address the associated difficulties[57]. The ongoing advancement of techniques based on nanotechnology has raised hopes that debilitating and possibly lethal illnesses may soon be successfully treated. If we are to swiftly and fully exploit the enormous potential of nanotechnology, which is currently untapped, we must prioritize filling the gaps brought about by insufficient efficacy and preclinical safety studies. Although nanotechnology can address a lot of issues, this does not mean that there aren't any difficulties or restrictions. Recent advances in nanotechnology-based drug delivery have fundamentally altered the way that many illnesses are treated, particularly those associated with cancer, neurological disorders, and infectious infections[58]. Nanotechnology decreases adverse effects and increases therapeutic efficacy by facilitating controlled release profiles, enhanced bioavailability, and targeted drug delivery. Drug Delivery Systems Based on Nanoparticles: Because of their unique physicochemical properties, such as a high surface area-to-volume ratio92, nanoparticles can efficiently deliver drugs to specific body areas. One of the main advantages of nanotechnology is its ability to direct drugs to specific cells or tissues. Targeting ligands, such as peptides, antibodies, or small molecules, are commonly added to the surface of nanoparticles to do this. These ligands selectively attach to disease cell-overexpressed receptors [59].
CONCLUSION:
Nanotechnology has become a revolutionary approach to drug delivery because of its ability to overcome the shortcomings of conventional treatment systems, such as poor solubility, low bioavailability, rapid metabolism, and systemic toxicity. Using a range of nanocarriers, including liposomes, polymeric nanoparticles, dendrimers, and solid lipid nanoparticles, researchers have developed techniques for the targeted, controlled, and extended administration of pharmaceuticals. Mechanisms such as stimuli-responsive release systems, active targeting via ligand-receptor interactions, and passive targeting via the EPR effect can significantly improve therapeutic benefits. From the creation of vaccines and antimicrobial treatments to cancer treatment and medication delivery to the central nervous system, nanotechnology has many applications. However, despite these advancements, problems with toxicity, stability, large-scale manufacturing, regulatory approval, and ethical considerations remain. These barriers need to be eliminated in order to translate laboratory advancements into clinical solutions that are safe, effective, and affordable. The combination of personalized nanomedicine, multifunctional systems, and smart nanocarriers may have a significant impact on future advancements in drug delivery. With further research, technological developments, and established regulatory frameworks, nanotechnology is expected to play a significant role in the advancement of precision medicine and the improvement of healthcare outcomes worldwide.
REFERENCES


Vanshika Giri*, Pranita Ghadage, Dhairyashil Deshmukh, Pratik Dhalgade, Omkar Khavare, Abhijit Jadhav, Tejashree Khamkar, Nanotechnology in Drug Delivery, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 1579-1592 https://doi.org/10.5281/zenodo.17365497
 10.5281/zenodo.17365497
10.5281/zenodo.17365497
