Womens college of pharmacy peth-vadgoan 416 112.
Gillian–Barre syndrome (GBS) is a rare, but potentially fatal, immune-mediated disease of the peripheral nerves and nerve roots that is usually triggered by infections. Guillain-Barre syndrome (GBS) is now considered a heterogeneous group of related disorders, that includes Miller Fisher syndrome and various GBS subtypes [4]. Guillain-Barré Syndrome (GBS) is an umbrella term that describes several clinically and electro physiologically heterogeneous disorders that share the common feature of acute onset regional or generalized flaccid paralysis with or without sensory loss [1]. Immune-mediated immune responses may play a role in the development of GBS by interacting with brain tissue. Because the infected organism contains homologous epitopes, it initiates molecular and cell immune responses that interact with the ganglioside surface areas of the peripheral nerve (cell imitation) [5]. The severity of Guillain-Barré syndrome is exacerbated by these variables, especially in low-income and middle-income countries where healthcare systems are already constrained and struggle to meet the demands of other diseases [6].
Guillain-Barre syndrome was first discovered more than a century ago [2]. The clinical presentation of Guillain-Barre syndrome (GBS) was first described by Landry in 1859. He reported five patients with an ascending postinfectious polyneuropathy and all the features of GBS except for areflexia. The illness has been recognized as GBS since 1916, when Guillain Barre´, and Strohl described two French soldiers who contracted the illness during World War I [11]. Advances in the past century include investigating the immune-mediated pathophysiology of the disease, recognizing the spectrum of presentations, advancing diagnostic modalities, and prognostic models, and performing randomized trials of treatments to improve outcomes. Given the morbidity that can occur without treatment, all physicians should have knowledge of this rare disease [2]. Over 100 years after it was first described, GBS is now one of the best understood neuroinflammatory diseases, providing valuable insights into the mechanisms of peripheral nerve inflammation. However, many aspects of its nature continue to elude our comprehension [3]. Guillain-Barré syndrome (GBS) is a rare but serious post-infectious immune-mediated neuropathy. It results from the autoimmune destruction of nerves in the peripheral nervous system causing symptoms such as numbness, tingling, and weakness that can progress to paralysis [2]. We know that GBS is a postinfectious, monophasic, immune?mediated polyradiculoneuropathy, and its diagnosis is largely based on clinical patterns with or without the support of laboratory findings and electrophysiology [3].
Etiology:
The Guillain-Barre syndrome (GBS) and its variants are considered post-infectious, immune-mediated neuropathies [2]. The pathogen most frequently responsible for the initial infection that leads to GBS is Campylobacter jejuni (C. jejuni). C. jejuni is most commonly spread to people through their diet, specifically by the ingestion of raw or undercooked poultry meat and fish, unpasteurized milk, or water contaminated with the bacteria [6].
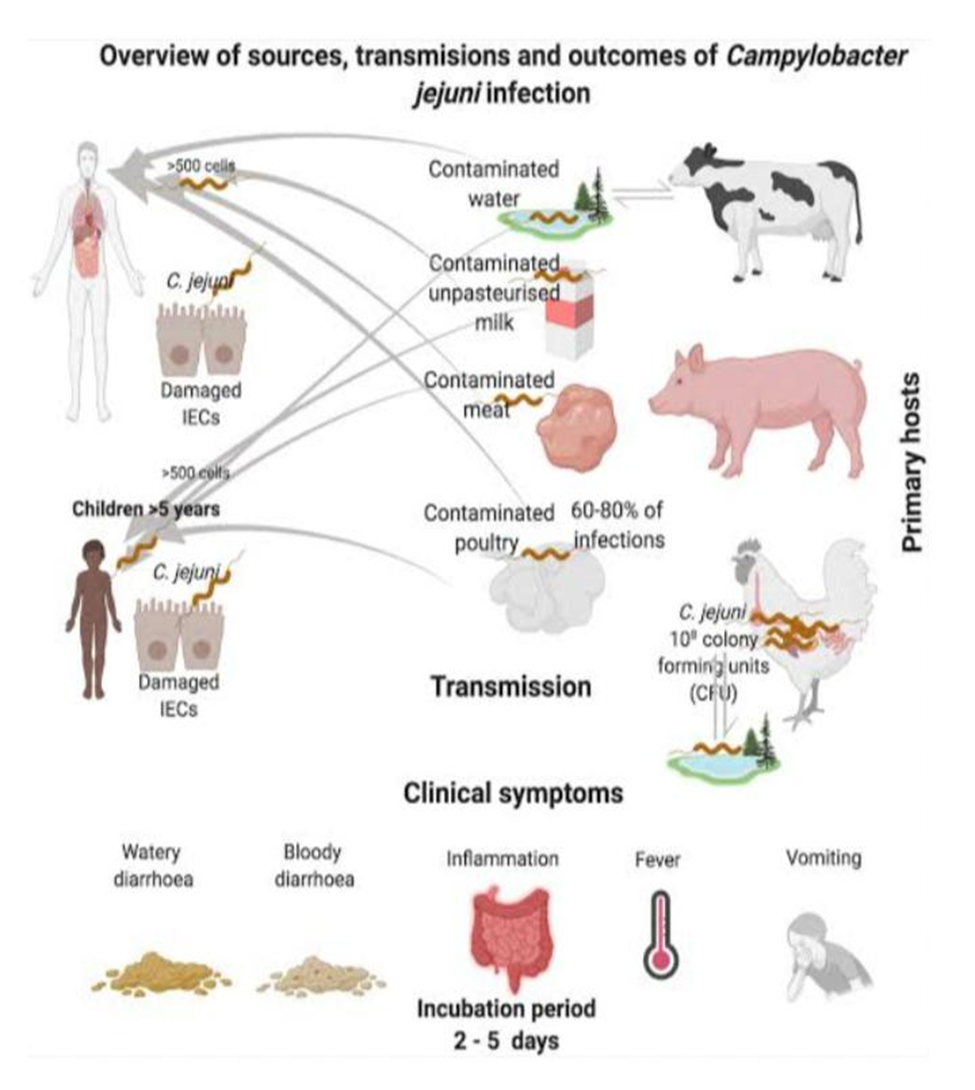
Fig1: Overview Of Sources, Transmissions and Outcomes of Campylobacter Jejuni Infection.
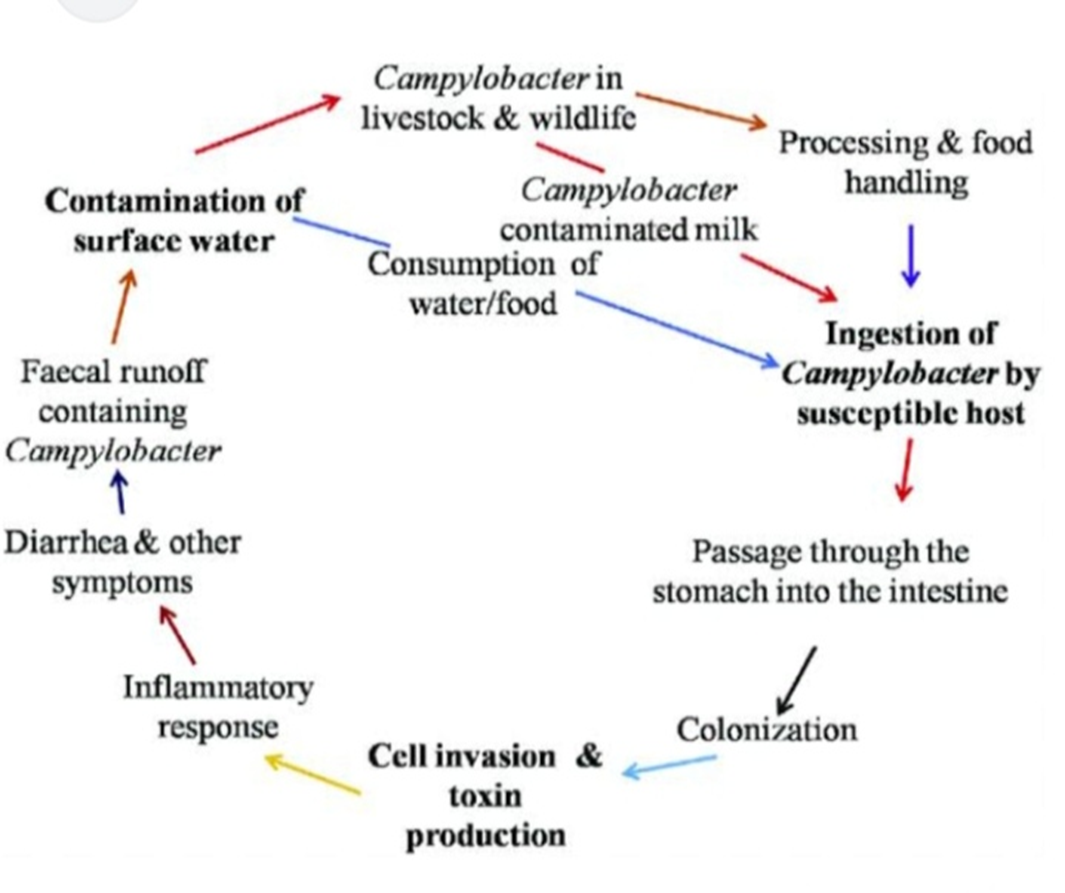
Fig2: Etiology of Campylobacter Jejuni
Pathophysiology:
The pathophysiology of GBS can be delineated into two pivotal stages: initiation by an immunological trigger and immune?mediated disruption of axons and or myelin. Based on electrophysiology, GBS has been traditionally divided into two forms: acute inflammatory demyelinating polyradiculoneuropathy (AIDP) and acute motor axonal neuropathy (AMAN). The notion that this neurophysiological dichotomy reflects a true underlying pathological difference between primarily demyelinating versus axonal GBS is currently being challenged, and the new EAN/PNS guidelines no longer support the distinction between AIDP and AMAN [3].
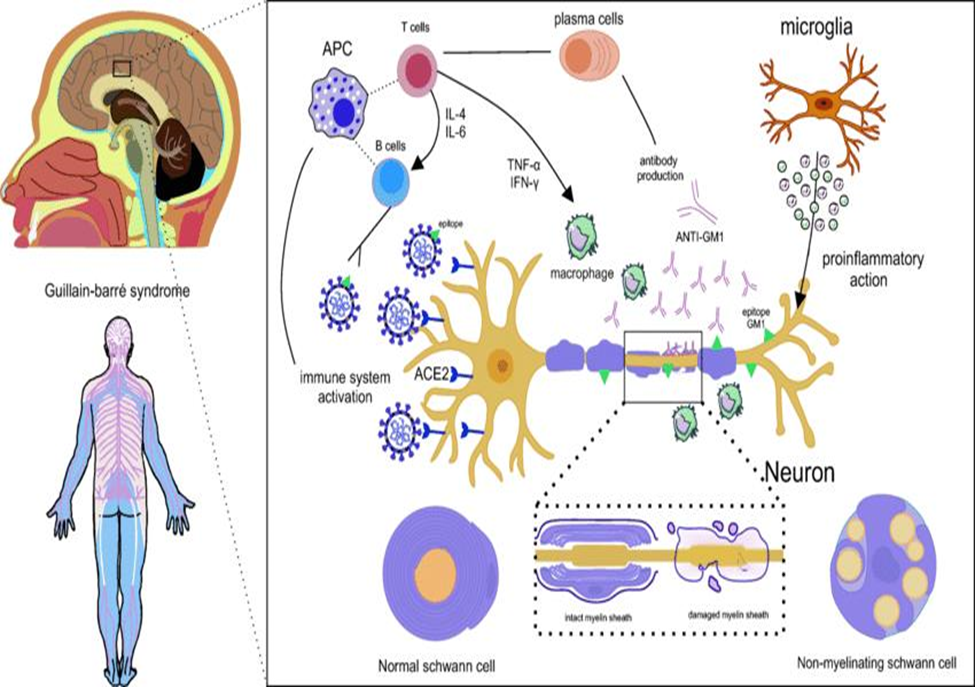
Fig3:: Representation of molecular mimicry, pathophysiological mechanism of GBS.
The pathophysiology of GBS is evidenced by the mechanism of molecular mimicry, in which the virus shares epitopes common to neuron components, such as the myelin sheath and axonal lining. Thus, direct virus infection triggers the activation of the immune system and APC precursor cells, which differentiate into T and B lymphocytes. Also, the viral epitope is recognized by the B lymphocyte and the T lymphocyte releases isoleucine such as IL-6 and interleukin 4 (IL-4), in addition to cytokines such as TNF-α and interferon-gamma (IFN-γ) for macrophage activation, triggering local inflammation that can be exacerbated. Thus, there is the production of antibodies (ANTI-GM1) to attack the virus, however, by sharing epitopes, these antibodies also attack components of the neuron. The recruitment of more macrophages increases inflammation, as well as the performance of the microglia that release cytokines such as IFN-γ and interleukin 1 beta (IL-1β). Finally, the neuron is in hyperinflammation and operates with its reduced functionality or loses it definitively, being able to suffer cell death and causing irreversible damage to the patient with this syndrome [10].
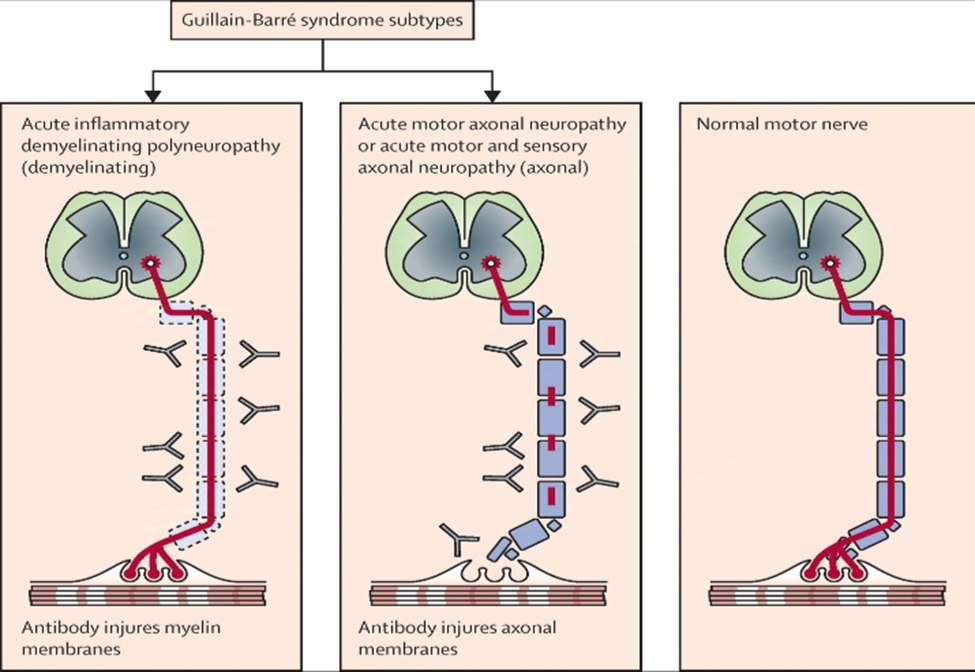
Fig.4: Major Guillain-Barré syndrome subtypes in which antibody-mediated effector pathways, including complement activation, cause glial or axonal membrane injury with consequent conduction failure [20].
Symptoms of Guillain-Barre syndrome may include:
1.A pins and needles feeling in the fingers, toes, ankles or wrists.
2.Weakness in the legs that spreads to the upper body.
3.Unsteady walk or not being able to walk or climb stairs.
4.Trouble with facial movements, including speaking, chewing or swallowing.
5.Double vision or inability to move the eyes.
6.Severe pain that may feel achy, shooting or camplike and may be worse at night.
7.Trouble with bladder control or bowel function.
8.Rapid heart rate.
9.Low or high blood pressure.
10.Trouble breathing [7].
Relapse rare but not ruled out: Most individuals recover from GBS without recurrence, though a much smaller group of patients may experience return of symptoms months or even years later. Continuous medical follow-up is necessary for long-term management [18].
|
Complications |
When to be alert |
|
Choking |
Bulbar palsy |
|
Cardiac arrhythmias |
All patients |
|
Delirium |
Limited communication |
|
Depression |
Limited communication |
|
Urinary retention |
All patients |
|
Constipation |
Immobility |
|
Corneal ulceration |
Facial palsy |
|
Dietary deficiency |
Bulbar and facial palsy |
Fig: Important complications of GBS [12].
WHO response:
WHO is supporting countries to manage GBS by enhancing surveillance of causative agents such as campylobacter jejuni or Zika virus; providing guidelines for the assessment and management of GBS; supporting countries to implement guidelines and strengthen health systems to improve the management of GBS cases; and defining the research agenda for GBS. WHO’s Intersectoral global action plan on epilepsy and other neurological disorders aims to address the challenges and gaps in providing care and services for people with neurological conditions such as GBS and ensure a comprehensive, coordinated response across sectors [8].
Diagnosis:
To diagnose Guillain-Barre Syndrome, healthcare providers use various tests to confirm the condition and rule out other potential causes of the symptoms. Early and accurate diagnosis is crucial for starting treatment promptly. Here are the common diagnostic methods:
Electromyography (EMG) and Nerve Conduction Tests:
These tests measure the health and function of skeletal muscles and the nerves controlling them:
1) Electromyography (EMG): This involves inserting tiny electrodes into muscles to assess their electrical activity and detect nerve damage.
2) Nerve Conduction Tests: These check how quickly and efficiently electrical signals travel through your nerves. Abnormal results can indicate nerve damage typical of GBS.
3) Spinal Tap (Lumbar Puncture)-
In this procedure, a healthcare provider inserts a needle into the lower back to collect cerebrospinal fluid (CSF) from around the spinal cord.
Key Findings in GBS:
A normal white blood cell count and an elevated protein level in the CSF are characteristic of GBS and observed in about 80% of cases. If other abnormalities are present, they may point to a different condition.
4) Imaging Tests-
An MRI (magnetic resonance imaging) of the spine may be recommended to rule out alternative diagnoses and look for other possible causes of symptoms, such as inflammation or nerve compression [9].
Recovery:
Treatment and care:
The following are recommendations for treatment and care of people with Guillain-Barré syndrome:
1) Guillain-Barré syndrome is potentially life-threatening. GBS patients should be hospitalized so that they can be monitored closely.
2) Supportive care includes monitoring of breathing, heartbeat and blood pressure. In cases where a person’s ability to breathe is impaired, he or she is usually put on a ventilator. All GBS patients should be monitored for complications, which can include abnormal heart beat, infections, blood clots, and high or low blood pressure.
3) There is no known cure for GBS, but treatments can help improve symptoms of GBS and shorten its duration.
4) Given the autoimmune nature of the disease, its acute phase is typically treated with immunotherapy, such as plasma exchange to remove antibodies from the blood or intravenous immunoglobulin. It is most often beneficial when initiated 7 to 14 days after symptoms appear.
5) In cases where muscle weakness persists after the acute phase of the illness, patients may require rehabilitation services to strengthen their muscles and restore movement (8).
Recently two types of treatments can speed recovery and reduce symptoms:
1) Plasma exchange- also known as plasmapheresis. Plasma is the liquid portion of part of your blood. In a plasma exchange, plasma is removed and separated from your blood cells. The blood cells are then put back into your body, which makes more plasma to replace what was removed. Plasmapheresis may work by ridding plasma of certain antibodies that contribute to the immune system’s attack on the peripheral nerves.
2) Immunoglobulin therapy- Immunoglobulin containing healthy antibodies from blood donors is given through a vein. High doses of immunoglobulin can block the damaging antibodies that may contribute to Guillain-Barre syndrome.
People with Guillain-Barre syndrome need physical help and therapy before and during recovery. Your care may include:
1) Movement of your arms and legs by caregivers before recovery, to help keep your muscles flexible and strong.
2) Physical therapy during recovery to help you cope with fatigue and regain strength and proper movement.
3) Training with adaptive devices, such as a wheelchair or braces, to give you mobility and self-care skills [17].
Foods to Include in the Diet for Guillain-Barré Syndrome:
1.High-protein foods: Include sources like chicken, fish, eggs, and legumes to support muscle recovery and immune function.
2.Fruits and vegetables: Rich in vitamins and antioxidants, citrus fruits, berries, spinach, and broccoli can help reduce inflammation.
3.Healthy fats: Avocados, nuts, and olive oil are sources of essential fatty acids, which protect nerve cells.
4.Whole grains: Oats, brown rice, and whole wheat are full of energy and fiber that initiate good digestion and health
5.Probiotics: Dahi (curd) and buttermilk improve the health of the gut, which is an important development for a healthy response.
Foods to Avoid with Diet in Guillain-Barré Syndrome:
Some of the foods that need to be avoided because they trigger inflammation:
1.Processed foods: In these food products, unhealthy fats and chemical preservatives are in a big number that would spike up inflammation and damage the recovery process.
2.Sugar-rich foods: that contain high amounts of sweets, soft drinks, and excessive sugar can weaken the immune system and inflammation.
3.Fatty foods: oily food that is heavy and greasy can provoke inflammation and digestive disturbance
4.Too much milk: High-fat dairy products can also cause inflammation in some patients.
5.High-sodium food: Processed snacks and canned food may provoke water retention and other health problems [19].
CONCLUSION:
Guillain-Barre Syndrome (GBS) is a rare but serious autoimmune disorder that requires prompt medical attention. While most people recover, some may experience long-term effects. Early diagnosis and treatment can significantly improve outcomes. As per all study on Guillain-Barre syndrome there is no specific treatment to this disease but our life style management and regular check up with help providers we can fight with this disease. Ongoing studies focus on understanding GBS triggers, improving treatments and enhancing recovery. Guillain-Barré Syndrome (GBS) is a complex condition, and while there is no specific cure, a combination of:
1. Supportive care
2. Lifestyle management
3. Regular check-ups
4. Rehabilitation therapy
Can significantly improve outcomes and quality of life.
Ongoing research aims to:
1. Identify triggers
2. Develop more effective treatments
3. Enhance recovery
REFERENCES

Sanika Patil*, Sayali Patil, Gillian Barre Syndrome: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 1521-1529. https://doi.org/10.5281/zenodo.15860547
 10.5281/zenodo.15860547
10.5281/zenodo.15860547
