Department of General Medicine, Government General Hospital, Kadapa, Andhra Pradesh, India. Department of Pharmacy Practice, P. Rami Reddy Memorial College of Pharmacy, Andhra Pradesh, India.
Sweet syndrome, also known as acute febrile neutrophilic dermatosis, is a rare inflammatory condition characterized by sudden tenderness, erythematous skin lesions, fever, and neutrophilia. It typically presents with raised, erythematous plaques, sometimes accompanied by pseudo-blistering or pustules, primarily on the face, neck, chest, and extremities. The condition can involve extracutaneous manifestations, including ocular, joint, and internal organs. While the absence of vasculitis was initially a diagnostic criterion, recent studies suggest that vasculitis changes occur in up to 74% of cases, challenging the distinction between sweet syndrome and leukocytoclastic vasculitis. Sweet syndrome is associated with infections, autoimmune disorders, malignancies (particularly myelodysplastic syndrome and acute myeloid leukaemia), and pregnancy. Its pathogenesis is thought to be a hypersensitivity reaction. Treatment with systemic corticosteroids often results in rapid improvement; however, recurrence is observed in approximately 25% of cases. Alternative therapies like colchicine, dapsone, and cyclosporine have also shown efficacy.
Sweet syndrome is often associated with underlying malignancies, infections, or drug reactions. Clinically, it presents with tender, erythematous plaques and nodules, usually on the upper extremities, neck, and face. Histopathology shows a substantial neutrophil infiltration of the dermis without any signs of vasculitis.
Case 1: A 35-year-old female presented with multiple, well-defined, erythematous plaques and nodules on the upper extremities and neck. She reported an associated fever and malaise for one week. There was no history of recent infections, malignancies, or drug exposure. In this report, we describe two clinical cases of sweet syndrome, highlighting their presentation, diagnostic evaluation, and clinical course.
Dermatological Examination:
Multiple bilaterally symmetrical erythematous plaques and nodules (3 18 cm × 2 18 cm) over the arms. Mild tenderness noted. Hyperpigmented atrophic scarring on the left leg. Two single plaques, each approximately 2 cm in diameter, with peripheral collarette scaling on the right leg.
Neurological Examination:
Radial and ulnar nerve thickening was observed, but no sensory or motor deficits were noted.
Investigations:
CBC: Leucocytosis with neutrophilia. ESR and CRP: markedly elevated.
Skin biopsy: negative dermal neutrophilic infiltrate with no evidence of vasculitis.
Autoimmune panel: Negative.
Treatment and Outcome: The patient was initiated on systemic corticosteroids (prednisolone (40mg/day) with gradual tapering over six weeks. Symptoms resolved within two weeks, with residual hyperpigmentation.
Case 2: A 65-year-old female presented with a single, well-demarcated erythematous plaque on the upper back, accompanied by mild pruritus but no systemic symptoms. There was no history of fever, infections, or malignancy.
Dermatological Examination:
Single erythematous plaque measuring approximately 4 cm × 3 cm over the scapular region.
Mild peripheral scaling.
No mucosal involvement or ulceration.
Investigations:
CBC: mild neutrophilia.
ESR and CRP: mildly elevated.
Skin biopsy: Neutrophilic dermal infiltrates without leukocytoclastic vasculitis.
Treatment and Outcome: The patient was prescribed topical corticosteroids (clobetasol propionate 0.05%), and colchicine 0.5 mg twice daily was administered. Regressed within three weeks without recurrence.
CASE PRESENTATION:
Case 1: A 35-year-old female presented to the Government General Hospital, Kadapa, with complaints of multiple, well-defined, erythematous plaques and nodules predominantly affecting the upper extremities and neck. The lesions were associated with mild tenderness, fever, and malaise persisting for the past week. The patient denied any history of recent infections, malignancies, or drug exposure. Upon dermatological examination, the patient exhibited multiple bilaterally symmetrical erythematous plaques and nodules, ranging in size from 3 cm to 18 cm, distributed over the arms and neck.

Figure 01 Figure 02
Lesions before treatment on the neck Lesions after treatment on the Neck
The lesions were mildly tender on palpation. A hyperpigmented atrophic scar was observed on the left leg, and a solitary plaque with peripheral collarette scaling was noted on the right leg. Neurological evaluation revealed a thickening of the radial and ulnar nerves. No motor or sensory deficiencies were found, though. To establish a definitive diagnosis, several laboratory investigations were conducted. The complete blood count (CBC) showed marked leukocytosis with neutrophilia, suggesting an ongoing inflammatory response. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were significantly elevated, further indicating systemic inflammation. A skin biopsy confirmed the presence of a dense dermal neutrophilic infiltrate without vasculitis, consistent with Sweet Syndrome.
Figure 01 Figure 02
Before treatment After treatment
The autoimmune panel was negative, ruling out any associated autoimmune disorders. Based on the clinical presentation, laboratory findings, and histopathological features, a diagnosis of Sweet Syndrome (Acute Febrile Neutrophilic Dermatosis) was established. The patient was started on systemic corticosteroid therapy (prednisolone 40 mg/day), with a gradual tapering regimen over six weeks. Supportive measures, including analgesics, emollients, and topical corticosteroids, were provided for symptomatic relief. The patient showed significant improvement within two weeks, with a notable reduction in erythema and regression of skin lesions, leaving behind residual post-inflammatory hyperpigmentation. At the one-month follow-up, she exhibited complete recovery with no recurrence of symptoms.
Case 2: A 65-year-old female presented to Government General Hospital, Kadapa, with complaints of multiple erythematous plaques and rashes distributed over the abdomen, legs, and hands, accompanied by mild pruritus and mucosal ulcerations in the oral cavity. Before the appearance of skin lesions, she explained that she had a fever with chills and rigors and widespread arthralgia. The patient denied any history of preceding infections, malignancies, or recent drug exposure. On dermatological examination, multiple well-demarcated erythematous plaques with peripheral scaling were observed over the stomach, lower extremities, and upper limbs, with some lesions displaying central clearing and post-inflammatory hyperpigmentation. Examination of the oral mucosa revealed painful ulcers over the buccal mucosa, with no active bleeding or significant crusting. There was no involvement of the lips or tongue.
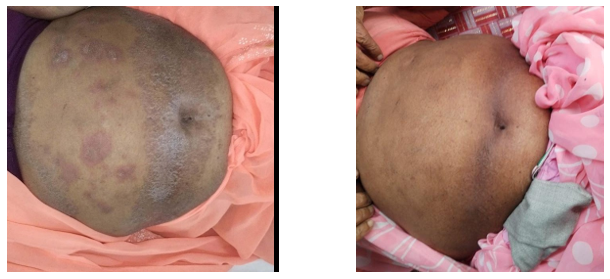
Figure 01 Figure 02
Before treatment over abdomen Lesions after treatment over Abdomen
The Laboratory investigations revealed mild neutrophilia on a complete blood count, along with elevated inflammatory markers, including erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). Histopathological analysis of a skin biopsy demonstrated dense neutrophilic dermal infiltrates without evidence of leukocytoclastic vasculitis, findings consistent with Sweet syndrome with mucosal involvement. The patient was initially treated with systemic corticosteroids (prednisolone 30 mg/day) with a gradual tapering regimen over six weeks. Additionally, topical corticosteroids (clobetasol propionate 0.05%) and colchicine (0.5 mg twice daily) were prescribed to manage inflammation and prevent recurrence.
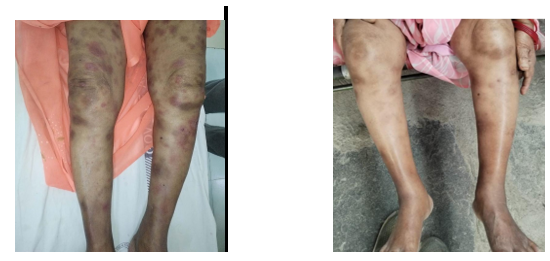
Figure 01 Figure 02
Before treatment over the legs, Lesions after treatment over the legs
Supportive care included emollients and antihistamines (cetirizine 10 mg daily) for symptomatic relief. Throughout treatment, the patient exhibited significant clinical improvement, with the resolution of fever and joint pains within the first week. Cutaneous lesions regressed progressively, and mucosal ulcers healed without residual scarring. By the third week, complete resolution of skin lesions was observed, with no evidence of recurrence on follow-up.
DISCUSSION:
Overview Of Sweet Syndrome:
Sweet syndrome, also known as acute febrile neutrophilic dermatosis, is a rare inflammatory condition characterized by sudden onset of tender, erythematous skin lesions, fever, and neutrophilia. It typically affects adults between 30 and 50 years of age and shows a female predominance. The illness is frequently linked to systemic symptoms like fever, malaise, and high neutrophil counts.[1] Juicy papules and plaques, usually on the face, are the clinical manifestation of Sweet syndrome. shoulders, and trunk, with prominent edema. These lesions may appear as raised, erythematous plaques, sometimes accompanied by pseudo-blistering or pustules, primarily on the face, neck, chest, and extremities.[2] Extracutaneous involvement may occur, affecting the eyes, joints, and internal organs. Histopathologically, it is characterized by a sterile neutrophilic infiltrate in the dermis.[3] Although vasculitis was traditionally considered absent in Sweet syndrome, recent studies suggest that vasculitic changes may be present in up to 74% of cases. This challenges the historical distinction between Sweet syndrome and leukocytoclastic vasculitis.[4] Interestingly, many cases show histologic evidence of vasculitis, leading to the proposal that Sweet syndrome may represent a variant of leukocytoclastic vasculitis rather than a distinct entity.[5] The pathogenesis of Sweet syndrome is not fully understood but is thought to involve a hypersensitivity reaction with aberrant activation, proliferation, and skin-homing of neutrophils.[6] Both innate and adaptive immune responses are believed to play roles in its development.[7] Various triggers have been identified, including infections, autoimmune disorders, malignancies (particularly myelodysplastic syndrome and acute myeloid leukemia), and pregnancy. Medications such as bortezomib, azacitidine, and colony-stimulating factors have also been implicated. In some cases, the syndrome has been associated with autoimmune conditions and, more rarely, rheumatoid arthritis. Sweet syndrome may act as a marker for underlying malignancy, particularly hematological malignancies, with up to 16% of patients developing associated cancers.[8] Patients with malignancy-associated Sweet syndrome are often older, anemic, and have lower platelet counts. Treatment typically involves systemic corticosteroids, which usually result in rapid clinical improvement.[9] However, recurrence occurs in approximately 25% of cases. Alternative treatments such as colchicine, dapsone, potassium iodide, and cyclosporine have shown efficacy. In refractory cases, immune suppressants, biologics, and small-molecule therapies may be considered. Despite available therapies, some cases remain resistant, highlighting the need for continued research and the identification of novel therapeutic targets.[10] Sweet syndrome remains a fascinating and complex dermatological condition with diverse clinical presentations, systemic associations, and evolving diagnostic and treatment approaches.
Comparison Of Case 1 And Case 2
|
Feature |
Case 1 |
Case 2 |
|
Age & Gender |
35-year-old female |
65-year-old female |
|
Clinical Presentation |
Single large erythematous plaque with collarette scaling over the shoulder |
Multiple erythematous plaques & nodules, tender lesions on extremities |
|
Systemic Symptoms |
Mild fever, fatigue |
Fever, malaise |
|
Histopathology |
Neutrophilic infiltration with edema |
Dense neutrophilic infiltrate without vasculitis |
|
Laboratory Findings |
Normal WBC count, mild elevation of inflammatory markers |
Leukocytosis, elevated ESR & CRP |
|
Triggering Factor |
Possible post-infectious immune response |
Idiopathic (no apparent underlying cause) |
|
Treatment |
Topical corticosteroids, systemic anti-inflammatory therapy |
Systemic corticosteroids, NSAIDs, supportive care |
|
Outcome |
Significant improvement with topical therapy |
Complete resolution with steroids |
Key Findings and Implications:
Clinical Variability:
Histopathological Confirmation:
Potential Triggers:
Management and Prognosis:
The prognosis is generally favorable, but the recurrence risk remains, especially in idiopathic cases.
Clinical and Research Implications
CONCLUSION
Sweet Syndrome, though rare, presents with a broad clinical spectrum ranging from localized cutaneous lesions to systemic inflammatory involvement. The comparative analysis of the two cases illustrates this variability, with Case 1 demonstrating classic febrile neutrophilic dermatosis and systemic features, while Case 2 exhibited a milder, localized variant with mucosal involvement. Despite differences in presentation and severity, both cases underscore the critical role of histopathological confirmation in establishing a definitive diagnosis. Prompt initiation of corticosteroid therapy resulted in favorable outcomes in both patients, reaffirming its role as the mainstay of treatment. This study emphasizes the need for clinicians to maintain a high index of suspicion for Sweet Syndrome in patients presenting with sudden-onset erythematous plaques and systemic symptoms, even in the absence of known triggers. Early recognition and individualized treatment not only facilitate rapid recovery but also help prevent unnecessary investigations and misdiagnosis. Ongoing research into the pathogenesis and alternative therapies may further enhance management strategies, particularly for recurrent or steroid-refractory cases.
ACKNOWLEDGEMENT: We would like to thank the Superintendent, Head Department of General Medicine, Government General Hospital, Kadapa, for their support in writing this case study. Sincere thanks to the patient and their family for granting consent to utilize the patient's valuable medical records for the case study.
Conflict Of Interest: The authors declare that there is no conflict of interest.
Abbreviations: CBC: complete blood count, ESR: erythrocyte sedimentation rate, CRP: C-reactive protein, NSAIDs: non-steroidal anti-inflammatory drugs, WBC: white blood cells
Patient Consent: The patients referenced in this case study have provided consent for publication, acknowledging the study's nature and understanding that their identity will be kept confidential. The patient is satisfied with the medication they received.
Summary:
Sweet Syndrome, or acute febrile neutrophilic dermatosis, is a rare inflammatory skin disorder characterized by the abrupt onset of painful erythematous plaques, systemic symptoms such as fever and malaise, and neutrophilia. This study presents a comparative analysis of two female patients diagnosed with Sweet Syndrome, illustrating the clinical variability and highlighting diagnostic and therapeutic approaches.
Case 1 involved a 35-year-old female with multiple erythematous nodules and plaques over the upper extremities and neck, associated with fever and systemic inflammation. Laboratory findings revealed leukocytosis, elevated ESR and CRP, and histopathology confirmed dense dermal neutrophilic infiltrates without vasculitis. The patient responded well to systemic corticosteroids (prednisolone 40 mg/day), with complete resolution within four weeks.
Case 2 featured a 65-year-old female with a localized erythematous plaque on the back and mild pruritus, but no significant systemic symptoms. Laboratory investigations showed mild neutrophilia and mildly elevated inflammatory markers. Skin biopsy confirmed the diagnosis. The patient was managed successfully with topical corticosteroids (clobetasol) and oral colchicine (0.5 mg twice daily), achieving remission within three weeks.
The discussion emphasizes Sweet Syndrome’s association with infections, autoimmune diseases, malignancies, and drug exposures, and outlines its pathogenesis as a hypersensitivity reaction involving neutrophil dysregulation. Histopathology remains the diagnostic cornerstone, particularly in distinguishing it from vasculitic dermatoses. Although traditionally considered non-vasculitic, newer evidence suggests vasculitic changes may occur in a subset of cases. Both cases demonstrated favorable outcomes, reinforcing the efficacy of corticosteroid therapy as the mainstay of treatment. The study highlights the importance of early recognition, histological confirmation, and individualized management. It also suggests a need for further research into steroid-sparing agents for recurrent or refractory disease.
REFERENCES


S. Iqra*, S. Farida, S. Ayesha Ahamed, Dr. S. Prabhu Kiran Reddy, Dr. C. Rajaram, Sweet Syndrome in Contrast: A Two-Case Comparative Study of Localized and Systemic Manifestations, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 3870-3878. https://doi.org/10.5281/zenodo.15728501
 10.5281/zenodo.15728501
10.5281/zenodo.15728501
