Ideal Institute Of Pharmacy
Transdermal drug delivery has made an important contribution to medical practice. It is a medicated patch that delivers a specific amount of medication through the skin into the blood stream. An advantage of a transdermal drug delivery route over other types of medication delivery is that the patch provides a controlled release of the medication into the patient, usually through either a porous membrane covering a reservoir of medication or through body heat melting thin layers of medication embedded in the adhesive. The present investigation was aimed to formulate transdermal films of Spironolactone and Metformin HCL, which can be used for the treatment prevailing symptoms of PCOS using Solvent evaporation method and evaluated for physicochemical parameters like thickness, weight variation, moisture uptake, moisture content, folding endurance, and drug content values. Polycystic ovary syndrome (PCOS) is currently the leading cause of menstrual complications in women. It is characterized by clinical and/or biochemical hyperandrogenism, ovulation abnormalities and the presence of enlarged and/or polycystic ovaries in ultrasound images. It is often comorbid with hyperinsulinemia, dyslipidemia, overweight or obesity, and is a risk factor for the development of diabetes. Nine transdermal patches were prepared using different concentrations of Hydrooxypropyl methyl cellulose K4M (HPMC K4M) and Ethyl cellulose as polymers and Polyethylene glycol (PEG) as plasticizer. It was concluded that as the concentration of Plasticizer increases the folding endurance increases and as the concentration of Polymer increases thickness of patch and weight uniformity increases. Percentage moisture content and percentage moisture uptake decreases with increase in polymer concentration.
TRANSDERMAL DRUG DELIVERY SYSTEM (TDDM)
Transdermal drug delivery system has been in existence for a long time. In the past, the most commonly applied systems were topically applied creams and ointments for dermatological disorders. It is a widely accepted means of drug delivery system. The occurrence of systemic side-effects with some of these formulations is indicative of absorption through the skin. A number of drugs have been applied to the skin for systemic treatment. In a broad sense, the term transdermal delivery system includes all topically administered drug formulations intended to deliver the active ingredient into the general circulation. Transdermal therapeutic systems have been designed to provide controlled continuous delivery of drugs via the skin to the systemic circulation. [1] Most of the drug molecules penetrate through the skin through intercellular micro route. However, this route of delivery is challenged by the barrier nature of skin. The epidermis is the main barrier for penetration of the drug. [4] Therefore the role of permeation or penetration enhancers in TDDS is vital as they reversibly reduce the barrier resistance without damaging viable cells. [5] Several chemical enhancers such as sulphoxide, alcohols, fatty acids, polyols, urease and physical enhancers such as sonophorosis, electroporation, iontophorosis, and magnetophorosis have been used in TDDS. [4] Moreover, it overcomes various side effects like painful delivery of the drugs and the first pass metabolism of the drug occurred by other means of drug delivery systems. [1] They can even avoid gastrointestinal problems associated with drugs and low absorption. These therapeutic advantages reflect the higher marketing potential of TDDS. [5] So, this transdermal drug delivery system has been a great field of interest in the recent time. Many drugs which can be injected directly into the blood stream via skin have been formulated. [1] The appeal of using the skin as a portal of drug entry lies in case of access, its huge surface area, and systemic access through underlying circulatory and lymphatic networks and the noninvasive nature of drug delivery. Delivery of drugs through the skin for systemic effect, called transdermal delivery was first used in 1981. [9]The drug is mainly delivered to the skin with the help of a transdermal patch which adheres to the skin. [1] The advantages of delivering drugs through the skin include: [1] 1. Hepatic first pass metabolism, salivary metabolism and intestinal metabolism are avoided. 2. The ease of usage makes it possible for patients to self-administer. 3. Since the composition of skin structurally and biologically is the same in almost all the humans, there is minimal inter and intra patient variation. 4. Drugs showing gastrointestinal irritation and absorption can be suitably administered through the skin. 5. The risks, pain and inconvenience associated with parenteral therapy are evaded. 6. The release is more prolonged than oral sustained drug delivery systems. The following are some of the disadvantages of the transdermal delivery system: [1] 1. There is possibility of skin irritation due to the one or many of the formulation components. 2. Binding of drug to skin may result in dose dumping.
TRANSDERMAL PATCH
Nicotine patches were the first transdermal patch success raising the market value of TDDS in medicine to newer heights. [5] A transdermal patch, which may also be considered a Transdermal Drug Delivery System (TDDS), is defined as a flexible, multi-layered, pharmaceutical single dose preparation of varying size containing one or more active substances to be applied to the intact skin for systemic absorption. [9] The first commercially available prescription patch was approved by the U.S. Food and Drug Administration in December 1979 containing scopolamine for motion sickness. The highest selling transdermal patch in the United States was the nicotine patch which releases nicotine to help with cessation of tobacco smoking. The first commercially available vapour patch to reduce smoking was approved in Europe in 2007. In addition, various other patches are available in market including fentanyl, an analgesic for severe pain, nitroglycerin patches for angina, lidocaine patches, marketed as Lidoderm, relieve the peripheral pain of shingles (herpes zoster), Buprenorphine, marketed as BuTrans, as analgesia for moderate to severe chronic pain. It is also now commonly used offlabel, for pain from acute injuries and chronic pain. Flector (Diclofenac Epolamine) patch is an NSAID topical patch for the treatment of acute pain due to minor strains, sprains, and contusions. It is also being used in the treatment of pain and inflammation for chronic conditions benefiting from NSAIDs including fibromyalgia and arthritis. Recent developments expanded their use to the delivery of hormonal contraceptives, antidepressants and even pain killers and stimulants for Attention Deficit Hyperactivity Disorder (ADHD). [1] A transdermal patch has several components including Baking layer, drug containing layer, rate controlling membrane, adhesive and release liner which play a vital role in the release of the drug via skin. Though all layers may not be available in all types of TDP as there are several types of transdermal patches. [4] Transdermal patches usually contain an excess of active substance than that delivered to the patient during use. This excess is necessary to maintain a clinically effective rate of delivery over time and allow the minimum patch surface area. [9] Various types of patches along with various methods of applications have been discovered to deliver the drug from the transdermal patch. Because of its great advantages, it has become one of the highly research field among the various drug delivery system. [1] The biological properties of drug for preparing transdermal patch should be of short half-life, should not produce allergic response and the drug should be potent with a daily dose of the order of a few mg/day. [4]
The advantages of delivering drugs through the Transdermal Patch: [9]
Delivery via the transdermal route is an interesting option because transdermal route is convenient and safe. The positive features of delivery drugs across the skin to achieve systemic effects are:
The disadvantages of delivering drugs through the Transdermal Patch: [9]
The various steps involved in transport of drug from patch to systemic circulation are as follows:
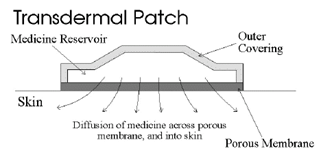
Figure 1: A typical transdermal patch showing diffusion of drug across porous membrane, and into skin.
COMPONENTS OF TRANSDERMAL PATCH: [1] [4] [5] [9]
The basic components of transdermal patch consists of polymer matrix / Drug reservoir, active ingredient (drug), permeation enhancers, pressure sensitive adhesive (PSA), backing laminates, release liner, and other excipients like plasticizers and solvents.
Polymer matrix:
Polymers are the backbone of a transdermal drug delivery system. Systems for transdermal delivery are fabricated as multilayered polymeric laminates in which a drug reservoir or a drug–polymer matrix is sandwiched between two polymeric layers: an outer impervious backing layer that prevents the loss of drug through the backing surface and an inner polymeric layer that functions as an adhesive and/or rate controlling membrane. Polymer selection and design must be considered when striving to meet the diverse criteria for the fabrication of effective transdermal delivery systems. The main challenge is in the design of a polymer matrix, followed by optimization of the drug loaded matrix not only in terms of release properties, but also with respect to its adhesion cohesion balance, physicochemical properties, compatibility and stability with other components of the system as well as with skin. [1]
The polymers utilized for TDDS can be classified as: [1]
The following criteria should be satisfied for a polymer to be used in a transdermal system: [9]
Drug:
The most important criteria for TDDS are that the drug should possess the right physicochemical and pharmacokinetic properties. Transdermal patches offer much to drugs which undergo extensive first pass metabolism, drugs with narrow therapeutic window, or drugs with short half-life which causes non-compliance due to frequent dosing. For example, drugs like rivastigmine for Alzheimer’s and Parkinson dementia, rotigotine for Parkinson, methylphenidate for attention deficit hyperactive disorder and selegiline for depression are recently approved as TDDS.
The selection of drug for transdermal drug delivery depends upon various factors: [9]
a. Physicochemical properties:
Permeation enhancers:
To increase permeability of stratum corneum so as to attain higher therapeutic levels of the drug permeation enhancers interact with structural components of stratum corneum i.e., proteins or lipids. The enhancement in absorption of oil soluble drugs is apparently due to the partial leaching of the epidermal lipids by the chemical enhancers, resulting in the improvement of the skin conditions for wetting and for trans-epidermal and trans-follicular permeation. The miscibility and solution properties of the enhancers used could be responsible for the enhanced transdermal permeation of water soluble drugs. [1] The penetration enhancer should be pharmacologically inert, non-toxic, non-allergenic, non-irritating and ability to act specifically, reversibly and for predictable duration. It should not cause loss of body fluids, electrolytes or other endogenous materials. [9] The permeation of drugs across the skin may also be enhanced by physical means including iontophorosis, electroporation, application of ultrasound (sonophoresis), and use of microscopic projection. Iontophorosis passes a few milliamperes of current to a few square centimeters of skin through the electrode placed in contact with the formulation, which facilitates drug delivery across the barrier. Electroporation is a method of application of short, high-voltage electrical pulses to the skin. After electroporation, the permeability of the skin for diffusion of drugs is increased by 4 orders of magnitude. The electrical pulses are believed to form transient aqueous pores in the stratum corneum, through which drug transport occurs. It is safe and the electrical pulses can be administered painlessly using closely spaced electrodes to constrain the electric field within the nerve-free stratum corneum. Application of ultrasound, particularly low frequency ultrasound, has been shown to enhance transdermal transport of various drugs including macromolecules. It is also known as sonophoresis. Transdermal patches with microscopic projections called microneedles were used to facilitate transdermal drug transport. Needles ranging from approximately 10-100 ?m in length are arranged in arrays. When pressed into the skin, the arrays make microscopic punctures that are large enough to deliver macromolecules, but small enough that the patient does not feel the permeation or pain. The drug is surface coated on the microneedles to aid in rapid absorption. They are used in development of cutaneous vaccines for tetanus and influenza. Various other methods are also used for the application of the transdermal patches like thermalporation, magnetophoresis, and photomechanical waves. However, these methods are in their early stage of development and require further detailed studies.
Pressure sensitive adhesive (PSA):
A PSA maintains an intimate contact between patch and the skin surface. It should adhere with not more than applied finger pressure, be aggressively and permanently techy, and exert a strong holding force. These include polyacrylate, polyisobutylene and silicon based adhesives. The selection of an adhesive is based on numerous factors, including the patch design and drug formulation. PSA should be physicochemical and biologically compatible and should not alter drug release. The PSA can be positioned on the face of the device (as in reservoir system) or in the back of the device and extending peripherally (as in case of matrix system).
Backing laminate:
The primary function of the backing laminate is to provide support. Backing layer should be chemical resistant and excipients compatible because the prolonged contact between the backing layer and the excipients may cause the additives to leach out or may lead to diffusion of excipients, drug or permeation enhancer through the layer. They should have a low moisture vapour transmission rate. They must have optimal elasticity, flexibility, and tensile strength. Examples of some backing materials are aluminium vapour coated layer, plastic film (polyethylene, polyvinyl chloride, polyester) and heat seal layer.
Release liner:
During storage release liner prevents the loss of the drug that has migrated into the adhesive layer and contamination. It is therefore regarded as a part of the primary packaging material rather than a part of dosage form for delivering the drug. The release liner is composed of a base layer which may be non-occlusive (paper fabric) or occlusive (polyethylene and polyvinylchloride) and a release coating layer made up of silicon or Teflon. Other materials used for TDDS release liner include polyester foil and metalized laminate.
Other excipients:
Various solvents such as chloroform, methanol, acetone, isopropanol and dichloromethane are used to prepare drug reservoir. In addition plasticizers such as dibutylpthalate, triethylcitrate, polyethylene glycol and propylene glycol are added to provide plasticity to the transdermal patch.
TYPES OF TRANSDERMAL PATCHES: [1]
Single layer drug in adhesive:
In this type the adhesive layer contains the drug. The adhesive layer not only serves to adhere the various layers together and also responsible for the releasing the drug to the skin. The adhesive layer is surrounded by a temporary liner and a backing.

Figure 2: Design of Single layer drug in adhesive transdermal patch.
Multi -layer drug in adhesive:
This type is also similar to the single layer but it contains an immediate drug-releaselayer and other layer will be a controlled release along with the adhesive layer. The adhesive layer is responsible for the releasing of the drug. This patch also has a temporary liner-layer and a permanent backing.

Figure 3: Design of Multi- layer drug in adhesive transdermal patch.
Vapour patch:
The patch containing the adhesive layer not only serves to adhere the various surfaces together but also serves as to release the vapour. The vapour patches are new to the market, commonly used for releasing the essential oils in decongestion. Various other types of vapour patches are also available in the market which are used to improve the quality of sleep and reduces the cigarette smoking conditions.
Reservoir system:
In this system the drug reservoir is embedded between an impervious backing layer and a rate controlling membrane. The drug releases only through the rate controlling membrane, which can be micro porous or non-porous. In the drug reservoir compartment, the drug can be in the form of a solution, suspension, gel or dispersed in a solid polymer matrix. Hypoallergenic adhesive polymer can be applied as outer surface polymeric membrane which is compatible with drug.

Figure 4: Design of Reservoir system transdermal patch.
Microreservoir system:
The system consists of microscopic spheres of drug reservoirs which releases drug at a zero order rate for maintaining constant drug levels. Microreservoir system is a combination of reservoir and matrixdispersion system. The aqueous solution of water soluble polymer is mixed with drug to form a reservoir. It is then followed by dispersing the solution homogeneously using high shear mechanical force in a lipophilic polymer to form thousands of microscopic drug reservoirs. Cross linking agents are added to stabilize the thermodynamically unstable dispersion by in-situ cross-linking the polymer.

Figure 5: Design of microreservoir transdermal patch.
VARIOUS METHODS FOR PREPARATION OF TDDS: [1] [9]
Circular Teflon mould method:
Solutions containing polymers in various ratios are used in an organic solvent. Calculated amount of drug is dissolved in half the quantity of same organic solvent. Enhancers in different concentrations are dissolved in the other half of the organic solvent and then added. Plasticizer (e.g., Di-N-butylphthalate) is added into the drug polymer solution. The total contents are to be stirred for 12 hrs and then poured into a circular Teflon mould. The moulds are to be placed on a levelled surface and covered with inverted funnel to control solvent vaporization in a laminar flow hood model with an air speed of 0.5 m/s. The solvent is allowed to evaporate for 24 h. The dried films are to be stored for another 24 h at 25±0.5°C in a desiccators containing silica gel before evaluation to eliminate aging effects. These types of films are to be evaluated within one week of their preparation.
Mercury substrate method:
The drug is dissolved in polymer solution along with plasticizer. It is followed by stirring for 10- 15 minutes to produce a homogenous dispersion and poured into a levelled mercury surface, covered with inverted funnel to control solvent evaporation.
“IPM membranes” method:
The drug is dispersed in a mixture of water and propylene glycol containing carbomer940 polymers and stirred for 12 h in magnetic stirrer. The dispersion is to be neutralized and made viscous by the addition of tri-ethanolamine. Buffer (pH 7.4) can be used in order to obtain solution gel, if the drug solubility in aqueous solution is very poor. The formed gel will be incorporated in the IPM (isopropyl myristate) membrane. 1.2.3.4. “EVAC membranes” method: In order to prepare the target transdermal therapeutic system, 1?rbopol reservoir gel, polyethelene (PE), ethylene vinyl acetate copolymer (EVAC) membranes can be used as rate control membranes. If the drug is not soluble in water, propylene glycol is used for the preparation of gel. Drug is dissolved in propylene glycol; carbopol resin will be added to the above solution and neutralized by using 5% w/w sodium hydroxide solution. The drug (in gel form) is placed on a sheet of backing layer covering the specified area. A rate controlling membrane will be placed over the gel and the edges will be sealed by heat to obtain a leak proof device.
Aluminium backed adhesive film method:
Transdermal drug delivery system may produce unstable matrices if the loading dose is greater than 10 mg. Aluminium backed adhesive film method is a suitable one. For preparation of same, chloroform is choice of solvent, because most of the drugs as well as adhesive are soluble in chloroform. The drug is dissolved in chloroform and adhesive material will be added to the drug solution and dissolved. A custom-made aluminium former is lined with aluminium foil and the ends blanked off with tightly fitting cork blocks.
Free film method:
Free film of cellulose acetate is prepared by casting on mercury surface. A polymer solution (e.g., 2% w/w) is prepared using organic solvent (e.g., chloroform). The optimized concentration of plasticizer is incorporated to the polymer solution (e.g., 40% w/w of polymer weight). Small volume (e.g., 5 ml) of polymer solution is poured in a glass ring which is placed over the mercury surface in a glass petri dish. The rate of evaporation of the solvent is controlled by placing an inverted funnel over the petri dish. The film formation is noted by observing the mercury surface after complete evaporation of the solvent. The dried film is separated out and stored between the sheets of wax paper in a desiccator until use. Free films of different thickness can be prepared by changing the volume of the polymer solution.
EVALUATION OF TRANSDERMAL PATCHES: [1] [4] [9]
Transdermal patches have been developed to improve clinical efficacy of the drug and to enhance patient compliance by delivering smaller amount of drug at a predetermined rate. This makes evaluation studies even more important in order to ensure their desired performance and reproducibility under the specified environmental conditions. These studies are predictive of transdermal dosage forms and can be classified into different types including physicochemical evaluation, in-vitro evaluation, and in-vivo evaluation. After the successful evaluation of physicochemical and in-vitro studies, in-vivo evaluations may be conducted.
Physicochemical Evaluation:
Thickness:
The thickness of transdermal film is determined by travelling microscope, dial gauge, screw gauge or micrometer at different points of the film.
Uniformity of weight:
Weight variation is studied by individually weighing 10 randomly selected patches and calculating the average weight. The individual weight should not deviate significantly from the average weight.
Drug content determination:
It can be determined by completely dissolving a small area (1 cm2 ) of polymeric film in suitable solvent of definite volume. The solvent is selected in which the drug is freely soluble. The selected area is weighed before dissolving in the solvent. The whole content is shaken continuously for 24 h in a shaker incubator followed by sonication and filtration. The drug in solution is assessed by appropriate analytical method.
Content uniformity test:
The test is applied as the gold standard to determine chemically the content of active constituent for each unit dose. The test is completed by performing assay to find out the content of drug material contained in polymeric film of the patch. According to USP the procedure consists of two stages. First stage consists of assaying the randomly selected ten units. It is followed by second stage to be performed on twenty more units when the first stage fails. Initially ten patches are selected and content is determined for individual patches. Test passes when all 10 unit doses have content ? 85 % and ? 115 % (RSD < 6>
Moisture content:
The prepared films are weighed individually and kept in a desiccators containing calcium chloride at room temperature for 24 h. The films are weighed again after a specified interval until they show a constant weight. The percent moisture content is calculated using following formula.
%Moisture Content = (???????????????????????????? ????????????????????? – ???????????????????? ?????????????????????) ???? 100 /???????????????????? ?????????????????????
Moisture Uptake:
Weighed films are kept in a desiccator at room temperature for 24 h. These are then taken out and exposed to 84% relative humidity using saturated solution of Potassium chloride in a desiccator until a constant weight is achieved. % moisture uptake is calculated as given below.
% Moisture Uptake = (???????????????????? ?????????????????????????????????????????????????? ?????????????????????)???? 100 /???????????????????????????? ?????????????????????
Folding Endurance:
Evaluation of folding endurance involves determining the folding capacity of the films subjected to frequent extreme conditions of folding. Folding endurance is determined by repeatedly folding the film at the same place until it break. The number of times the films could be folded at the same place without breaking gives the folding endurance value. [4]
Tensile Strength:
To determine tensile strength, polymeric films are sandwiched separately by corked linear iron plates. One end of the films is kept fixed with the help of an iron screen and other end is connected to a freely movable thread over a pulley. The weights are added gradually to the pan attached with the hanging end of the thread. A pointer on the thread is used to measure the elongation of the film. The weight just sufficient to break the film is noted. The tensile strength can be calculated using the following equation. [1]
Tensile Strength = ????/ ????.???? (1 + ???? /???? )
Where,
‘F’ is the force required to break.
‘a’ is width of film
‘b’ is thickness of film
‘L’ is length of film
‘l’ is elongation of film at break point
Water vapour transmission studies (WVT):
WVT is determined by taking one gram of calcium chloride in previously dried empty vials having equal diameters. The polymer films are pasted over the brim with the help of adhesive like silicon adhesive grease and then allowed to set for 5 minutes. The vials are accurately weighed and placed in humidity chamber maintained at 68 % RH. The vials are then weighed repeatedly up to seven consecutive days and an increase in weight was considered as a quantitative measure of moisture transmitted through the patch. [1]
Adhesive studies:
The therapeutic performance of TDDS can be affected by the quality of contact between the patch and the skin. The adhesion of a TDDS to the skin is obtained by using PSAs, which are defined as adhesives capable of bonding to surfaces with the application of light pressure. The adhesive properties of a TDDS can be characterized by considering the following factors. [5]
Peel Adhesion properties:
It is the force required to remove adhesive coating from test substrate. It is tested by measuring the force required to pull a single coated tape, applied to substrate at 180° angle. The test is passed if there is no residue on the substrate. [1]
Shear strength properties or creep resistance:
Shear strength is the measurement of the cohesive strength of an adhesive polymer i.e., device should not slip on application determined by measuring the time it takes to pull an adhesive coated tape off a stainless plate. [1]
In-vitro studies
In-vitro release studies
The amount of drug available for absorption to the systemic pool is greatly dependent on drug released from the polymeric transdermal films. Diffusion cells include Franz-diffusion cell and its modification Keshary-Chien Cell. In this method transdermal system is placed in between receptor and donor compartment of the diffusion cell. The transdermal system faces the receptor compartment in which receptor fluid (e.g., drug solution) is placed. The agitation speed and temperature are kept constant. The whole assembly is kept on magnetic stirrer and solution in the receiver compartment is constantly and continuously stirred throughout the experiment using magnetic beads. At predetermined time intervals, the receptor fluid is removed for analysis and is replaced with an equal volume of fresh receptor fluid. The concentration of drug is determined by suitable analytical method. The pH of the dissolution medium ideally should be adjusted to pH 5 to 6, reflecting physiological skin conditions. For the same reason, the test temperature is typically set at 32°C (even though the temperature may be higher when skin is covered). [9]
In-vitro permeation studies
After release from the polymeric films, drug reaches at skin surface is then passed to the dermal microcirculation by permeation through cells of epidermis and/or between the cells of epidermis through skin appendages. Usually permeation studies are performed by placing the fabricated transdermal patch with rat skin or synthetic membrane in between receptor and donor compartment in a vertical diffusion cell such as Franz diffusion cell or Keshary-Chien diffusion cell. The transdermal system is applied to the hydrophilic side of the membrane and then mounted in the diffusion cell with lipophillic side in contact with receptor fluid. The receiver compartment is maintained at specific temperature (usually 32±5°C for skin) and is continuously stirred at a constant rate. The samples are withdrawn at different time intervals and equal amount of buffer is replaced each time. The samples are diluted appropriately and estimated by suitable analytical method. The amount of drug permeated per square centimeter at each time interval is calculated. Many variables including design of system, patch size, surface area of skin, thickness of skin and temperature may affect the in-vitro properties of drug. Thus, the permeation studies involves preparation of skin, mounting of skin on permeation cell, setting of experimental conditions like temperature, stirring, sink conditions, withdrawing samples at different time intervals, sample analysis and calculation of flux (i.e., drug permeated per unit area per unit time). [9]
In-vivo Studies
In-vivo evaluations are the true depiction of the drug performance. The variables which cannot be taken into account during in-vitro studies can be fully explored during in-vivo studies. In-vivo evaluation of TDDS may be carried out using either animal models or human volunteers or both. [1]
Animal models
Considerable time and resources are required to carry out human studies, so animal studies are preferred at small scale. The most common animal species used for evaluating transdermal drug delivery systems are mouse, hairless rat, hairless dog, hairless rhesus monkey, rabbit, guinea pig etc. Based on the experiments conducted so far it is concluded that hairless animals are preferred over hairy animals in both in-vitro and in-vivo experiments. Rhesus monkey is one of the most reliable models for in-vivo evaluation of transdermal drug delivery. [1]
Human models:
The final stage of the development of a transdermal device involves collection of pharmacokinetic and pharmacodynamics data following application of the patch to human volunteers. Clinical trials are conducted to assess the transdermal systems including the efficacy, risk involved, side effects, and patient compliance. Phase-I clinical trials are conducted to determine mainly safety in volunteers and phase-II clinical trials determine short term safety and mainly effectiveness in patients. Phase-III trials indicate the safety and effectiveness in large number of patient population and phase-IV trials at post marketing surveillance are done for marketed patches to detect adverse drug reactions. Though human studies require considerable resources but they are the best to assess the performance of the drug. [1]
IDEAL PRODUCT REQUIREMENTS: [9]
STRUCTURE OF SKIN
THE SKIN:
The skin of an average adult body covers a surface area of approximately 2 sq. m. and receives about one third of the blood circulating through the body and serves as a permeability barrier against the transdermal absorption of various chemical and biological agent. [9] The skin can be considered to have four distinct layers of tissues including non-viable epidermis (stratum corneum), viable epidermis, viable dermis and hypodermis (subcutaneous connective tissue). The epidermis is the relatively thin, tough, outer layer of the skin. The epidermis has keratinocytes. They originate from cells in the deepest layer of the epidermis called the basal layer. New keratinocytes slowly migrate up toward the surface of the epidermis. Stratum corneum (Non-viable epidermis) is the outermost portion of the epidermis, relatively waterproof and, when undamaged, prevents most bacteria, viruses, and other foreign substances from entering the body. The epidermis also protects the internal organs, muscles, nerves, and blood vessels against trauma. The outer keratin layer of the epidermis (stratum corneum) is much thicker. Viable Epidermis layer of the skin resides between the stratum corneum and the dermis and has a thickness ranging from 50-100 ?m. The structure of the cells in the viable epidermis is physiochemically similar to other living tissues. Cells are held together by tonofibrils. The water content is about 90%. The dermis, the skin's next layer, is a thick layer of fibrous and elastic tissue (made mostly of collagen, elastin and fibrillin) that gives the skin its flexibility and strength. The dermis contains nerve endings, sweat glands and oil glands, hair follicles, and blood vessels. The subcutaneous tissue also known as hypodermis is not actually accepted as a true part of the structured connective tissue. It is composed of loose textured, white, fibrous connective tissue containing blood and lymph vessels. Most investigators consider the drug permeating through the skin enter the circulatory system before reaching the hypodermis where the fatty tissue serve as a depot of the drug.
PATHWAYS OF SKIN PERMEATION:
An important function of the skin is to protect the body from the external environment, and it is normally a very effective barrier to the permeation of active substances. However, for certain active substances, depending on their physicochemical properties, passive diffusion is possible to achieve a therapeutic effect. [6] Drug molecules permeate through skin surface by the different potential pathways including through the sweat ducts, through the hair follicles and sebaceous glands or directly across the stratum corneum. Since the last few years there is a point of debate among scientists for the relative importance of the shunt or appendageal route of transport across the stratum corneum and is further complicated by the lack of a suitable experimental model to permit separation of the these pathways. [1] Most of the drug molecules penetrate through the skin through intercellular micro route and therefore the role of permeation or penetration enhancers in TDDS is vital as they reversibly reduce the barrier resistance of the stratum corneum without damaging viable cells. [5]
BASIC PRINCIPLES OF TRANSDERMAL PERMEATION:
Earlier, skin was considered as an impermeable protective barrier, but later investigations were carried out which proved the utility of skin as a route for systemic administration. [1] Transdermal permeation is based on passive diffusion. Before a topically applied drug can act either locally or systemically, it must penetrate the stratum corneum – the skin permeation barrier. In the initial transient diffusion stage drug molecules may penetrate the skin along the hair follicles or sweat ducts and then absorbed through the follicular epithelium through the intact stratum corneum becomes the primary pathway for transdermal permeation. The release of a therapeutic agent from a formulation applied to the skin surface and its transport to the systemic circulation is a multistep process, which involves: [9]

POLYCYSTIC OVARY SYNDROME (PCOS)
WHAT IS POLYCYSTIC OVARY SYNDROME (PCOS)?
Polycystic ovary syndrome (PCOS), also known as the Stein-Leventhal syndrome, is one of the most common endocrinopathies among women of reproductive age. An abnormality in the ovaries is the primary cause of the disorder, but additional agents, such as obesity and environmental factors, affect the development of individual symptoms. [3] Women with polycystic ovarian syndrome (PCOS) have abnormalities in the metabolism of androgens and estrogen and in the control of androgen production. [11] In addition to hyperandrogenism and its related complications, the most common abnormalities associated with PCOS include menstrual disorders (amenorrhea or oligomenorrhea), often leading to infertility (in 73–74% of the cases), abdominal obesity (30–70%) and type 2 diabetes (approximately 10%). [3] Its prevalence among infertile women is 15%–20%. The etiology of PCOS remains unclear; however, several studies have suggested that PCOS is an X-linked dominant condition. Women with PCOS have abnormalities in the metabolism of androgens and estrogen and in the control of androgen production. High serum concentrations of androgenic hormones, such as testosterone, androstenedione, and dehydroepiandrosterone sulfate (DHEAS), may be encountered in these patients. However, individual variation is considerable, and a particular patient might have normal androgen levels. PCOS is also associated with peripheral insulin resistance and hyperinsulinemia, and obesity amplifies the degree of both abnormalities. Insulin resistance in PCOS can be secondary to a postbinding defect in insulin receptor signaling pathways, and elevated insulin levels may have gonadotropin-augmenting effects on ovarian function. In addition, insulin resistance in PCOS has been associated with adiponectin, a hormone secreted by adipocytes that regulates lipid metabolism and glucose levels. Both lean and obese women with PCOS have lower adiponectin levels than women without PCOS. A proposed mechanism for anovulation and elevated androgen levels suggests that under the increased stimulatory effect of luteinizing hormone (LH) secreted by the anterior pituitary, stimulation of the ovarian theca cells is increased. In turn, these cells increase the production of androgens (eg, testosterone, androstenedione). Because of a decreased level of follicle stimulating hormone (FSH) relative to LH, the ovarian granulosa cells cannot aromatize the androgens to estrogens, which leads to decreased estrogen levels and consequent anovulation. Growth hormone and insulin like growth factor 1 may also augment the effect on ovarian function. The ovaries may develop numerous small collections of fluid (follicles) and fail to regularly release eggs.

Figure 5. Polycystic ovary
DIAGNOSIS OF PCOS
Women with PCOS are predisposed to type 2 diabetes or develop cardiovascular disease. Factors implicated in the low fertility in these patients include anovulation, increased risk of early miscarriage, and late obstetric complications. [2] The disorder is diagnosed if 2 of the 3 specified conditions are met: [3]
According to the criteria proposed by the National Institutes of Health (NIH, 2009), a diagnosis of PCOS involves detection of clinical or biochemical hyperandrogenism and chronic ovulation disorders. 4 phenotypes of PCOS can be distinguished: [3]
A pelvic exam. The doctor visually and manually inspects your reproductive organs for masses, growths or other abnormalities. During a pelvic exam, your doctor inserts two gloved fingers inside your vagina. While simultaneously pressing down on your abdomen, he or she can evaluate your uterus, ovaries and other pelvic organs. [7]

Figure 6: Pelvic Diagnosis
Blood tests.
Your blood may be analyzed to measure hormone levels. This testing can exclude possible causes of menstrual abnormalities or androgen excess that mimics PCOS. You might have additional blood testing to measure glucose tolerance and fasting cholesterol and triglyceride levels. [7]
An ultrasound.
Your doctor checks the appearance of your ovaries and the thickness of the lining of your uterus. A wandlike device (transducer) is placed in your vagina (transvaginal ultrasound). The transducer emits sound waves that are translated into images on a computer screen. During a transvaginal ultrasound, your doctor or a medical technician inserts a wandlike device (transducer) into your vagina while you lie on your back on an exam table. The transducer emits sound waves that generate images of your pelvic organs, including your ovaries. On an ultrasound image (inset), a polycystic ovary shows many follicles. Each dark circle on the ultrasound image represents a fluid-filled follicle in the ovary. Your doctor may suspect PCOS if you have 20 or more follicles in each ovary. [7]

Figure 7: An Ultrasound Diagnosis
MANAGEMENT OF PCOS: [2] [3] [7] [11]
PCOS treatment focuses on managing your individual concerns, such as infertility, hirsutism, acne or obesity. Specific treatment might involve lifestyle changes or medication.
Lifestyle changes:
Your doctor may recommend weight loss through a low-calorie diet combined with moderate exercise activities. Even a modest reduction in your weight- for example, losing 5 percent of your body weight- might improve your condition. Losing weight may also increase the effectiveness of medications your doctor recommends for PCOS, and can help with infertility.
Medications:
To regulate your menstrual cycle, your doctor might recommend:
1. Combination birth control pills.
Pills that contain estrogen and progestin decrease androgen production and regulate estrogen. Regulating your hormones can lower your risk of endometrial cancer and correct abnormal bleeding, excess hair growth and acne. Instead of pills, you might use a skin patch or vaginal ring that contains a combination of estrogen and progestin.
2. Progestin therapy.
Taking progestin for 10 to 14 days every one to two months can regulate your periods and protect against endometrial cancer. Progestin therapy doesn't improve androgen levels and won't prevent pregnancy. The progestin-only minipill or progestin-containing intrauterine device is a better choice if you also wish to avoid pregnancy.
To help you your doctor might recommend:
1. Clomiphene (Clomid). This oral anti-estrogen medication is taken during the first part of your menstrual cycle.
2. Letrozole (Femara). This breast cancer treatment can work to stimulate the ovaries.
3. Metformin (Glucophage, Fortamet, others). This oral medication for type 2 diabetes improves insulin resistance and lowers insulin levels. If you don't become pregnant using clomiphene, your doctor might recommend adding metformin. If you have prediabetes, metformin can also slow the progression to type 2 diabetes and help with weight loss.
4. Gonadotropins. These hormone medications are given by injection.
5. Birth control pills. These pills decrease androgen production that can cause excessive hair growth.
6. Spironolactone (Aldactone). This medication blocks the effects of androgen on the skin. Spironolactone can cause birth defect, so effective contraception is required while taking this medication. It isn't recommended if you're pregnant or planning to become pregnant.
7. Eflornithine (Vaniqa). This cream can slow facial hair growth in women.
8. Electrolysis. A tiny needle is inserted into each hair follicle. The needle emits a pulse of electric current to damage and eventually destroy the follicle. You might need multiple treatments.
Lifestyle and home remedies:
To help decrease the effects of PCOS, try to:
1. Maintain a healthy weight. Weight loss can reduce insulin and androgen levels and may restore ovulation. Ask your doctor about a weight-control program, and meet regularly with a dietitian for help in reaching weight-loss goals.
2. Limit carbohydrates. Low-fat, high-carbohydrate diets might increase insulin levels. Ask your doctor about a low-carbohydrate diet if you have PCOS. Choose complex carbohydrates, which raise your blood sugar levels more slowly.
3. Be active. Exercise helps lower blood sugar levels. If you have PCOS, increasing your daily activity and participating in a regular exercise program may treat or even prevent insulin resistance and help you keep your weight under control and avoid developing diabetes.
DRUG PROFILE:
Metformin:


Spironolactone:


REVIEW OF LITERATURE
MATERIALS AND METHODS:
Materials:
All the chemicals used in this research were of standard pharmaceutical grade. Spironolactone and Metformin HCL was procured as a gift sample from Cipla Pharmaceuticals. Ethyl Cellulose, Polyethylene glycol 400(PEG 400), Methanol, Hydrooxypropyl methyl cellulose K4M (HPMC K4M), and Mercury were bought from Powder Pack PVT. LTD. Borivali, Mumbai. Square shape Bandage was bought from local market. Other materials used in the study such as chloroform, di-n-butyl-phthalate (DBP), etc.) Were of analytical grade.
Methods:
Ethyl Cellulose (EC) and Hydrooxypropyl methyl cellulose K4M (HPMC K4M) was used as polymer for the formulation of Transdermal Patch. Polyethylene glycol 400 (PEG 400) was used as a plasticizer, di-n-butyl-phthalate (DBP) is used as penetration enhancer. The polymer was dissolved in chloroform: methanol (1:1) solvent. The drug was dispersed uniformly in the viscous solution with continuous stirring. The DBP was also added on the same time. The resulting mass was poured into leveled mercury surface in a Petri dish covered with inverted funnel. The Petri dish was left undisturbed at room temperature for one day. The patch was obtained intact by slowly lifting from the Petri dish. Then the prepared patch was attached in the bandage to get the final product. The final patch was stored in the polyethelene bag for further evaluation.room temperature for one day. The patch was obtained intact by slowly lifting from the Petri dish. Then the prepared patch was attached in the bandage to get the final product. The final patch was stored in the polyethelene bag for further evaluation.
Table 1. Formulation design.
General procedure for the synthesis of chalcones by Claisen-Schmidt condensation
Equimolar quantities (0.001mol) of 2-acetylthiophene and respective aldehydes (0.001mol), were mixed and dissolved in minimum amount (3ml) of alcohol, to this aqueous potassium hydroxide solution (30%) was added slowly and mixed occasionally for 24 hrs, at room temperature. Completion of the reaction was identified by observing on precoated TLC plates of Merck. After completion of the reaction, the reaction mixture was poured into crushed ice, if necessary acidified with dil HCl. The solid separated was filtered and dried. It was purified by recrystallization or by column chromatography performed on silica gel (100-200 Mesh, Merck), using ethyl acetate and hexane mixture as mobile phase.5
Equimolar quantities (0.001mol) of 2-acetylthiophene and respective aldehydes (0.001mol) were mixed and dissolved in minimum amount (3ml) of alcohol; to this aqueous potassium hydroxide solution (30%) was added slowly and mixed. The entire reaction mixture was microwave irradiated for about 2-6 minutes at 180 watts, then kept aside for 1-3 hrs. Completion of the reaction was identified by observing on precoated TLC plates of Merck. After completion of the reaction, the reaction mixture was poured into crushed ice, if necessary acidified with dil HCl. The solid separated was filtered and dried. It was purified by recrystallization or by column chromatography performed on silica gel (100-200 mesh, Merck), using ethylacetate and hexane mixture as mobile phase. 6

Table 1. Formulation design.
Evaluations:
The thickness of each patch was measured by using digital vernier caliper at five different positions of the patch and the average was calculated.
Patches sizes of 2cm radius (4cm diameter) was cut. The weights of five patches were taken and the weight variation was calculated.
A patch of 2cm radius (4cm diameter) was cut evenly and repeatedly folded at the same place till it brakes. The numbers of times the film was folded at the same place without breaking give the value of the folding endurance.
Percentage moisture content, Percentage moisture uptake, Drug content determination, Tensile Strength, In-vitro release studies, In-vitro permeation studies etc. was unable to carry out due to lockdown because of COVID-19. So all this evaluation will be carried out in future.
RESULT AND CONCLUSIONS:
Transdermal films of Spironolactone and Metformin HCL have been successfully formulated as once daily formulation by Mercury Substrate Method. Nine different patch were prepared. The Patch was then evaluated on various parameter such as Thickness, Folding Endurance and weight uniformity as shown in Table 2. And on those parameter included in Table 2 it can be concluded that formulation (F9 and F10) was best prepared. The prepared patch can be best used for curing the symptoms related to PCOS. Evaluation of the prepared films in terms of physical appearance, weight uniformity, thickness uniformity, and Folding Endurance suggest that the method employed for formulation of the transdermal patches was reproducible and ensured excellent quality and uniformity in patch characteristics with minimum variability. It can also be concluded that as the concentration of polymer increases the thickness of patch, weight uniformity, folding endurance increases. Further, in vitro and ex vivo drug release studies for all the formulations will be carried out which will show the drug release. These results show that transdermal delivery of Spironolactone and Metformin HCL can have good potential applications in therapeutic arena offering advantages in terms of reduced dosing frequency, improved patient compliance, non-invasive characteristics, improved bioavailability, and easy termination of therapy. The administration of Spironolactone and Metformin HCL for the treatment of the symptoms of PCOS should further accentuate the aforesaid advantages.

Table 2. Evaluation of the patch.
PICTURES OF THE PREPARED TRANSDERMAL PATCH


REFERENCES:
Setji.T, Brown.A. “Polycystic ovary syndrome update on diagnosis and Treatment” The American Journal of medicine. 2014:127; 912-919 23. Williams.T, Mortad.R, Porter.S. “Diagnosis & Treatment of Polycystic Ovary Syndrome” American family physician. 2016:94(2); 106-113

Nitesh Choudhary, Preeti Gupta, Kajal Bokade, Aishwarya Sable, Ankita Suryavanshi, Shweta Patil, Formulation And Evaluation Of Transdermal Patch For Polycystic Ovary Syndrome (PCOS), Int. J. of Pharm. Sci., 2024, Vol 2, Issue 4, 875-902. https://doi.org/10.5281/zenodo.11045487
 10.5281/zenodo.11045487
10.5281/zenodo.11045487
