Department of Pharmaceutics, Himalayan Pharmacy Institute, Mjhitar, Sikkim, India
The complicated and compromised physiological process of diabetic wound healing is brought on by inflammatory and metabolic problems linked to diabetes mellitus. Chronic hyperglycemia impairs angiogenesis, increases oxidative stress, prolongs inflammation, and causes endothelial and cellular dysfunction, all of which interfere with normal wound repair mechanisms. The typical stages of wound healing—haemostasis, inflammation, proliferation, and tissue remodelling—are disrupted by these changes, delaying wound closure and raising the risk of infection, persistent ulcers, and amputations. One of the most serious consequences of diabetes is diabetic foot ulcers, which place a heavy strain on people and healthcare systems across the globe. Innovative therapeutic approaches targeted at enhancing diabetic wound care have been developed as a result of recent developments in biomedical research. These include microneedle systems, photobiomodulation therapy, platelet-rich plasma therapy, hydrogel-based dressings, and drug delivery systems based on nanotechnology. These methods improve angiogenesis, manage inflammation, prevent infection, and encourage tissue regeneration. Furthermore, promising future paths for enhancing therapeutic results are provided by cutting-edge technologies such as stem cell therapy, exosome-based therapies, artificial intelligence-assisted wound monitoring, and nanomedicine-based targeted delivery systems. In addition to discussing existing therapeutic techniques and highlighting the molecular principles underpinning diabetic wound healing, this review also examines emerging technologies and research gaps that could direct future advancements in the treatment of diabetic wounds.
Wounds can be classified as either acute or chronic. After trauma or surgery, an acute wound develops and goes through the phases of haemostasis, inflammation, proliferation, and maturation(1). Diabetic wounds have become far more common in recent years, and because of their vulnerability to infection and delayed healing, they present a serious medical issue. In addition to raising death rates, these wounds cause amputations and serious mobility problems(2).
In diabetes mellitus, haemostasis is frequently brought on by several clinical diseases or alterations. Both enhanced prothrombotic (clotting) and haemorrhagic (bleeding) tendencies may result from these changes. Platelet dysfunction, which results in hyperactivity of platelets, altered platelet membrane function, and decreased nitric oxide availability, can cause haemostasis in diabetes mellitus(3).
Moreover, it can be brought on by anomalies in the coagulation cascade, such as elevated thrombin production, decreased fibrinolysis, and increased clotting factors. Other causes include vascular dysfunction, where endothelial damage impairs the release of anticoagulant molecules such as heparin sulphate and thrombomodulin(4).
Wound healing is a complex physiological phenomenon that occurs when the integrity of the skin is lost, impairing its ability to act as a barrier. A rapid defence system may frequently be triggered because of the skin's high level of exposure to external irritants and the need to prevent infections inside.(5).
The first step of wound healing, known as haemostasis, is when platelet aggregation and blood clot formation halt bleeding and supply an extracellular matrix (ECM) for cell migration. Immune cells such as neutrophils and macrophages migrate to the site of injury during the inflammatory phase. With the help of inflammatory cytokines, fibroblasts divide and move throughout the proliferative phase(6).
Angiogenesis and the creation of ECM proteins, especially collagen, which is essential for tissue regeneration, cause re-epithelialization to take place in a matter of hours. To sustain cell proliferation, fibroblasts are necessary for the creation of the extracellular matrix. Scar development and collagen remodelling occur at the last stage. Aesthetic scar development, pain alleviation, prompt closure, and skin integrity restoration—all of which lower the risk of infection and other complications—are the ultimate objectives of wound healing(7).
Platelets can be considered the “guardian of haemostasis,” where their main function is to maintain vascular integrity. The skin serves its primary function as a protective barrier against environmental, physical, or biochemical insults(8).
Any compromise in the structural integrity of the skin, either by acute or chronic injury, leads to multiple serious disorders or disarray that can result in serious morbidity and mortality. To overcome these secondary complications, the body tends to initiate a multidisciplinary and vibrant healing process at the site of injury, leading to partial restoration of the skin’s barrier function, re-establishment of tissue integrity, and maintenance of internal homeostasis(9).
Diabetes mellitus (DM) is a complex metabolic disease that impacts the body's glucose levels. Meta-inflammation is the result of a critical connection between inflammation and metabolic disorders. The natural process of wound healing comprises our well-defined phases: haemostasis, inflammation, proliferation, and remodelling. Metabolic inflammation in diabetes mellitus plays a critical role in the onset and progression of Type 1 and Type 2 Diabetes Mellitus, which is a systemic and chronic low-grade inflammation associated with excess nutrients and energy(10).
Diabetes, including types 1 (T1DM) and 2 (T2DM), has been shown in earlier research to be an inflammatory illness. Damage to pancreatic β-cells caused by cell-mediated autoimmunity is the cause of TIDM. T2DM has been regarded as a metabolic disease, so the metabolic determinant is the main pathogenetic factor. Diabetes, including types 1 (T1DM) and 2 (T2DM), has been shown in earlier research to be an inflammatory illness(10).
Damage to pancreatic β-cells caused by cell-mediated autoimmunity is the cause of TIDM. Since type 2 diabetes is considered a metabolic disease, the primary pathogenetic factor is the metabolic determinant. More recent studies, however, have started to concentrate on low-grade inflammation as a key element in the aetiology, progression, and complications of type 2 diabetes(11).
Reduced insulin production and elevated insulin resistance (IR), linked to chronic inflammation, are hallmarks of type 2 diabetes. There is evidence that the adipose tissue of diabetic individuals secretes several inflammatory cytokines, including interleukin (IL)-6 and tumour necrosis factor-α (TNF-α). Elevated levels of inflammatory cytokines may make the liver more likely to trigger the activity of IkB kinase (IKK). Insulin receptor 1 (IRS-1) substrate expression is inhibited by activated IKK, which raises IR(8).
Additionally, they raise the risk of consequences like cardiovascular disease, atherosclerosis, and lung impairment. T2DM has been reclassified as an immunological disorder because of findings that inflammation is a major factor in its development. In order to reduce cytokine inflammation and fight IR, pharmaceutical treatment has been directed at the inflammatory pathways implicated in type 2 diabetes.
Patients and healthcare systems are burdened by chronic wounds, particularly diabetic ulcers, which can result in consequences such as amputations and even death. Diabetes impairs tissue regeneration by interfering with the wound-healing process. Drug delivery systems that target poor healing stages have been developed as a result of advances in our understanding of diabetic wound pathophysiology. By addressing problems like high pH and degrading enzymes in the wound environment, these systems seek to enhance wound closure. Efficient treatment plans are necessary for a quicker recovery and lower medical expenses.
BIOLOGY OF WOUND HEALING:
Normal wound healing consists of four interconnected and overlapping phases:
Homeostasis, inflammation, proliferation, and tissue remodelling are the four interrelated and overlapping phases of normal wound healing. Each phase involves distinct cell populations that depend on the oxygen and nutrition that blood vessels provide to the healing cells (12). Therefore, it is essential to use biodegradable polymers to improve angiogenesis, revascularisation, and homeostasis in diabetic wounds in order to speed up the healing process of chronic wounds (12,13). Growth factors promote the production of new tissue, such as angiogenesis, granulation tissue, and a provisional extracellular matrix (ECM), which are produced by fibroblasts, MMPs, and angiogenesis, respectively(12,13). Myofibroblasts near the wound's edges contract during this phase, reducing the wound's open surface area. Tissue remodelling is the last stage of wound healing, during which the vascular density of the wound drops from high proliferation-phase levels as newly produced tissue matures. The two main causes of chronic wound development are infection and inadequate tissue oxygenation(13). Two important elements that lead to the development of chronic wounds are infection and inadequate tissue oxygenation. The inflammatory stage of healing is prolonged by incomplete bacteria clearance(13). Uncontrolled inflammation can lead to the formation of biofilms, which in turn cause the self-secretion of an exopolysaccharide matrix (EPS), which shields bacteria from antibiotic therapy and the human immune response. Because oxygen is necessary for several wound healing processes, such as epithelialization, angiogenesis, and collagen deposition, normoxic conditions are also essential. Notably, hypoxia is a trustworthy marker of long-term injury(13).

Figure 1. Time course of different cell populations in the wound during the healing process.
MECHANISMS IN WOUND HEALING
STAGES AND AGENTS USED IN THE HEALING OF WOUNDS IN DIABETES:
Blood glucose management, surgical debridement, graft transplantation, and wound dressing are all part of the conventional clinical therapy of diabetic wounds(12–14). The effectiveness of surgery and subsequent healing is largely dependent on the early revascularisation of grafts (13).
By stimulating vascular endothelial growth factors and angiogenesis, biodegradable hydrogels containing bioactive compounds such as stem cells and antioxidants have been produced to speed up the healing of diabetic wounds (13).
Biodegradable hydrogels do not have multifunctional properties, which allow them to be the ideal scaffolds to encapsulate drugs/cells in wound healing/skin reconstruction. Ideal scaffolding dressing (12) In wound healing, materials should possess multifunctional properties including appropriate mechanical properties and pore structure, antibacterial activity, antiultraviolet, haemostatic ability, tissue-adhesive, injectable and self-healing, controlled biodegradation, sustained bioactive molecule release, and excellent biocompatibility(12,14).
In both clinical and research settings, platelet-rich plasma hydrogel (PRP gel), which is made from fibrin glue with a combination of platelet-rich plasma (PRP), thrombin, and/or calcium,11 is used to treat diabetic wounds that do not heal(15).
The antibacterial activity of the dressing possesses anti-infection, wound fluid absorption, and gaseous exchange. The haemostatic ability of the dressing could rapidly control bleeding as a potential haemostatic agent after organ damage(14). External dressings, mechanical hemostats, synthetic/hemisynthetic sealants, and active or adhesive agents are several types of hemostats that are applied topically. Topical active agents, which include thrombin and fibrinogen, function by actively initiating the fibrin clot formation and coagulation cascade. Patients with coagulation problems benefit most from these drugs(16). Passive hemostats are the name given to these hemostatic agents. In order to accomplish hemostasis, these hemostats can improve the functioning coagulation system(16). Hemostatic agents come in the following varieties(16):
Hemostatic agent applications may considerably lower haemorrhage-related morbidity and mortality(14,16).
Hemostatic hydrogel is also utilised to treat heart and artery bleeding, but mostly the bleeding that is uncontrollable following trauma or occurring during surgery is a major cause of global mortality(17). The hydrogel's therapeutic value is significantly increased when a GelMA component is added, since it preserves its ability to seal moist wounds and speeds up polymerisation by an order of magnitude(17,18).
Additionally, hemostatic needles are also used to treat arterial and heart bleeding(18). It prevents blood loss with self-sealing haemostatic needles(18).
Restoring tissue integrity following injury requires the multi-phase, intricately coordinated process of wound healing. Hemostasis, inflammation, proliferation, and remodelling are its four overlapping phases, and each is controlled by distinct cells, signalling chemicals, and structural proteins. A careful balance between these phases is necessary for effective wound healing; any disturbances could result in excessive scarring or chronic wounds(15,17).
PHARMACOTHERAPY FOR WOUND HEALING
SUCROSE OCTASULFATE:
Its application in neuro-ischemic ulcers is supported by randomised controlled trials, which also provide better healing results in diabetic foot ulcers(19).
Agents, such as sucrose octasulfate (UrgoStart), that interfere with and reduce the effects of matrix metalloproteinases (and do so decrease the time to heal the wound) have been employed to overcome this problem in the treatment of chronic wounds(19).
Mode of action the mode of action of sucrose octasulfate potassium salt is by decreasing the level of the excess MMPs and stabilising growth factors, thereby preventing them from being degraded by MMPs(19).
AUTOLOGOUS LEUCOCYTE, PLATELET, AND FIBRIN PATCHES:
PLATELET?RICH PLASMA (PRP)(19):
They have been shown to promote tissue regeneration in ulcers with or without ischemia.
Mechanism of action: The purpose of this treatment is to deliver a cocktail of growth factors, including platelet-rich plasma (PRP), which are involved in wound healing, including, but not limited to, stem cells, growth factors, mitogens, and inflammatory cytokines Healing, and providing a scaffold allowing concentration of the wound; the action of growth factors in the wound(19)(20).
NANOTECHNOLOGY-BASED DELIVERY SYSTEMS(19):
The development of nanotechnology has created a means of manipulating several factors involved in the wound healing process in diabetes, by prolonging the bioavailability of topical agents at the wound site. The use of iron oxide nanoparticles, glass/hydrogel nanoparticles, polyethylene glycol, and hyaluronic acid, which prolong the bioavailability of target molecules at the wound site, is discussed.(19)(21).
Mechanism of action: Nanotechnology for antiarthritic therapy on nanomaterial-based drug delivery carriers. Wound-healing pathway in DFUs(22). Certain molecules have been engineered to enhance their bioavailability and thus promote wound healing. thus bioavailability enhancement of drugs using nanotechnology by binding to iron oxide nanoparticles to thrombin(21). Thrombin induces chemotaxis and activates fibroblasts, epithelial and endothelial cells, and is important for the healing process, thus playing an important role in the early stage of wound healing(20).
IMPACT OF DIABETES ON WOUND HEALING(9):
Diabetes-related chronic hyperglycemia interferes with several cellular and molecular functions necessary for healthy tissue repair. Key mechanisms include:
IMPAIRED ANGIOGENESIS:
Diabetes causes a lack of new blood vessel creation, which means the wound receives insufficient oxygen and nutrients, delaying closure and tissue regeneration.
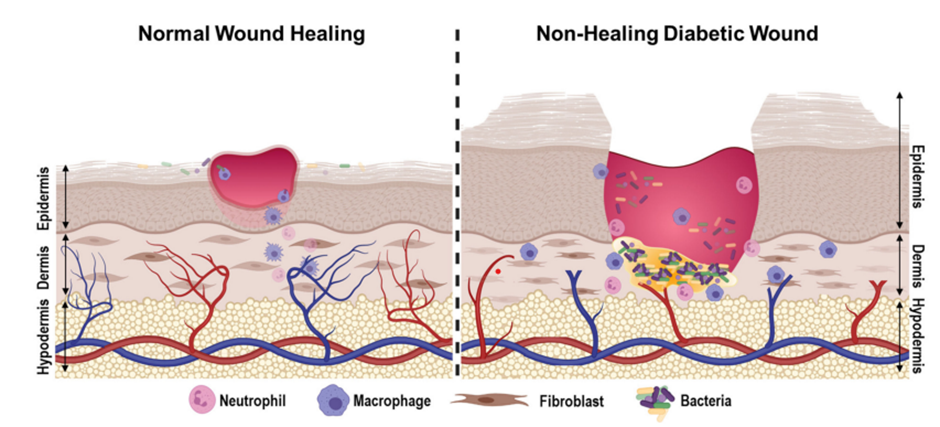
Figure: Pathophysiology of diabetic wounds. Diabetic wounds exhibit deregulated angiogenesis, chronically sustained sub-optimal inflammatory response, increased levels of reactive oxygen species, and persistent bacterial colonisation that often develops into a hard-to-treat(9).
ENDOTHELIAL AND CELLULAR DYSFUNCTION(9):
Hyperglycemia, which potentially leads to defects in wound healing and DFU is caused by atherosclerosis, the deficiency of the action of various skin cells, and peripheral neuropathy problems. In patient with DM(5)The hyperglycemia has been recognised as one of the factors that induce the abnormal function of EC, which plays an important role in the healing of DFU (23)through pressure-induced vasodilation, a response that is usually protective to the skin(9)(24).
OXIDATIVE STRESS(9):
In general, diabetes exerts a negative effect on wound healing, mostly by inducing severe oxidative stress. The high level of glucose present in diabetic patients causes an unbalance between the production of reactive oxygen species and the action of the body’s antioxidant systems, thus forming a highly oxidising environment at the wound site(9)(25). Although ROS(26)(27) also play an essential role in the wound healing process at the low level where it does not damage the cells, in high amounts, ROS have been shown to interfere with the cellular and molecular processes involved in the wound healing process, such as angiogenesis, the functioning of fibroblasts, and re-epithelialization(28)(25).
BARRIER DISRUPTION AND INFECTION(25):
Diabetes disrupts the skin barrier and increases susceptibility to infection, thereby severely impairing wound healing. Hyperglycemia disrupts the structure and function of keratinocytes and fibroblasts, thereby disrupting re-epithelialization and reducing the integrity of the barrier(29). In particular, diabetes reduces the expression of essential keratinocyte proteins and basement membrane components. This weakens the adhesion and survival of epithelial cells, which are vital for healing the skin barrier after injury(25)(29).
Such a compromised barrier only facilitates the penetration of bacteria. Diabetic wounds, including diabetic foot ulcers, are marked by uncontrolled inflammation, heightened neutrophil and macrophage mobility, and prolonged proinflammatory cytokine release. All these factors not only restrain healing but also facilitate bacterial attachment and biofilm formation, leading to infection(29)(9). The immune response in diabetes is further weakened by impaired macrophage function, reduced phagocytosis, and a failure to transition from a pro-inflammatory to a healing phenotype, all of which contribute to chronic wounds that are slow to resolve(30)(9).
MOLECULAR AND CELLULAR MECHANISMS:
IMPAIRED GROWTH FACTOR AND CELLULAR RESPONSES:
Raising the question of the vital functions of cells in diabetic conditions, one should consider the reduced or impaired production of growth factors for cell types, the weakened angiogenic response and, therefore, the synthesis of new spontaneous blood vessels, and the reduction of macrophages, keratinocytes, and fibroblasts functions(31). The lack of normal reaction by the cells and the deterioration of the synthesis of pro-cellular proteins and ECM remodelling(26) leads to the impairment of the ability of the cells to migrate, proliferate, and remodel the extracellular matrix, the three basic steps for which they are responsible and which, being impaired, lead to abnormal wound repair in diabetes(31).
OXIDATIVE STRESS AND IMPAIRED ANGIOGENESIS:
Hence, in diabetic wounds, a pro-oxidant microenvironment is formed with the increased level of reactive oxygen and nitrogen species that lead to oxidative cytocidal and cytostatic effects(32). Besides, decreased nitric oxide impairs angiogenesis and fibroblast function, and extracellular matrix failure, while hyperglycemia leads to deep leukocyte chemotaxis and increased elastase activity(31)(32).
CELLULAR DYSFUNCTION AND APOPTOSIS:
In diabetic ulcers, increased apoptosis of fibroblasts and impaired migration and differentiation by keratinocytes at the wound edge are seen(31). Molecular analysis had identified that the defective keratinocyte function was related to over-expression of c-myc, as well as β-catenin misplacement and lower EGFR signalling (31)(33).
KEY SIGNALLING PATHWAYS
Tissue regeneration, migration, and cell proliferation all depend on insulin signalling. ECM deposition(26)Wound contraction and maturation are all hampered in diabetes by insulin resistance and abnormal signalling pathways (including JNK and Smad)(33)(34).
Table 1
|
Mechanism |
Diabetic Alteration |
|
Growth factor production |
Decreased |
|
NO production |
Decreased |
|
Keratinocyte/ fibroblast fxn |
Impaired, migration |
|
Oxidative stress |
Increased ROS/RNS |
|
matrix metalloproteinases |
increased |
CURRENT THERAPEUTIC APPROACHES:
HYDROGEL-BASED DRESSINGS:
Hydrogel-based dressings are advanced wound care materials that have demonstrated significant benefits in the management of diabetic wounds, especially diabetic foot ulcers(35).
Hydrogel dressings are more successful than traditional dressings at promoting the healing of diabetic foot ulcers(36), with notably shorter healing durations and better rates of full wound closure, according to many meta-analyses and clinical studies(36)(37).
Modern wound care relies heavily on intelligent hydrogels, such as those that contain bioactive chemicals and nanoparticles. These dressings greatly aid in tissue regeneration and wound healing in diabetic patients by delivering medications, keeping the area wet, and having antibacterial, anti-inflammatory, and angiogenic qualities. The drug delivery can be done depending on the stage of wound healing; these dressings can be loaded with pro-angiogenic(8), antimicrobial, or anti-inflammatory substances for a regulated and prolonged release(8)(38).
MICRONEEDLE:
Microneedles enable precise, minimally invasive delivery of drugs, genes(39) and cells directly to the wound site to replace material, taking antibiotics, and anti-oxidative materials(40) immune modulators, and proinflammatory angiogenic effect substances(40). A single application in the wound microenvironment can have all these effects simultaneously; it is not necessary to repeatedly change materials. This technology offers advantages over traditional methods by improving local drug concentrations, reducing systemic side effects and enhancing patient comfort and compliance(40)(37).
PHOTOBIOMODULATION THERAPY:
Photo-biomodulation uses the specific wavelengths of light which is mostly (LEDs or lasers), which reduces inflammation and oxidative stress and promotes angiogenesis, as well as improve overall wound healing(41). This non-invasive method is becoming more popular as an adjunctive treatment for diabetic wounds(41). PBM is capable of promoting EC migration, proliferation and organisation for angiogenesis, infiltration of inflammatory cells to speed up healing and immune surveillance, as well as increase fibroblast matrix synthesis and wound contraction(42)(43)(41).
ADVANCED WOUND DRESSINGS:
Compared to regular dressings, specialised dressings, such as those containing sucrose octasulfate, have shown efficacy in randomised controlled studies, resulting in higher rates of complete wound closure and faster healing(44). The potassium salt of sucrose octasulfate functions at the tissue level and inhibits excess matrix metalloproteinases (MMP) production. Additionally, the distinctive structure of the potassium salt of sucrose octasulfate enables interactions with growth factors, restoring their biological functions and facilitating tissue formation(45)(46). These dressings maintain moisture, protect against infection, and can incorporate therapeutic agents for enhanced healing(44).
FUTURE DIRECTIONS AND RESEARCH GAPS:
FUTURE DIRECTION:
STEM CELL AND EXOSOME THERAPY:
Exosome-based treatments and mesenchymal stem cells (MSCs) are demonstrating great potential for diabetic wound repair. Compared to conventional stem cell therapy, exosome therapy is especially effective and safe since it lowers the chance of cancer progression and encourages healing by regulating immune responses and promoting tissue regeneration. To ascertain the best sources of stem cells, dosage, safety, and clinical procedures for these treatments, more investigation is necessary(47).
NANOMEDICINE AND TARGETED DELIVERY:
The stability, targeting, and continuous release of therapeutic agents like peptides and ncRNAs are improved by developments in nanotechnology, including delivery systems based on nanoparticles. These developments increase the effectiveness of treatments and lessen side effects, but further work is required to maximise biocompatibility and create condition-responsive delivery methods for practical application(48).
INTEGRATION OF AI AND DIGITAL WOUND MONITORING:
Diabetes wound care is being rapidly transformed by the combination of artificial intelligence (AI) with digital wound monitoring, which offers significant advancements in diagnosis, monitoring, and individualized treatment.
ENHANCED DIAGNOSTIC ACCURACY AND EARLY DETECTION:
Diabetic foot ulcer (DFU) classification, segmentation, and early detection are being greatly enhanced by AI-powered models, such as deep learning and generative AI. Compared to manual approaches, these technologies allow for more accurate and objective wound assessments (49)(50).
REMOTE AND REAL-TIME MONITORING:
Continuous, remote monitoring of wound healing is now possible due to the development of AI-driven smartphone applications and sensor-embedded "smart" dressings. Patients with mobility impairments or those living in distant areas may particularly benefit from these technologies' ability to automatically gather and evaluate data on wound size, temperature, pH, and exudate. This will enable prompt interventions and lessen the need for frequent clinic visits(51)(52).
PERSONALIZED MEDICINE AND PRECISION WOUND CARE:
Developments in stem cell manipulation highlight the most effective therapeutic tools available to improve wound healing processes like angiogenesis, cell proliferation, and collagen synthesis; possible techniques include gene modification, nanotechnology, and altering the scaffold microenvironment, including relative oxygen tension. Another possible cell-derived treatment that might make cell-free translational therapy possible is secretome engineering, namely, the use of extracellular vesicles(53).
RESEARCH GAPS:
DIVERSE DATASETS:
Future studies must place a high priority on gathering and utilising a variety of clinical datasets in order to improve the generalizability and resilience of AI models(54).
CLINICAL VALIDATION AND INTEGRATION:
To validate AI technologies and ensure their seamless integration into current healthcare operations, more real-world research and clinical trials are required(50)(51).
POOR REPRODUCIBILITY AND QUANTIFICATION:
Standardised, quantitative outcome metrics and reproducibility are lacking in many models. This variation makes comparing research more difficult and calls into question the validity of preclinical results(55).
TRANSLATIONAL FAILURE:
Many treatments that demonstrate effectiveness in animal models do not succeed in clinical trials, frequently as a result of poor preclinical model selection or restrictions. This emphasises how urgently models that more accurately replicate the wound settings of people with diabetes and forecast clinical outcomes are needed(55)(56).
INADEQUATE LONG-TERM CLINICAL TRIALS:
The absence of strong, long-term clinical studies assessing novel treatments and technology is a significant research gap that persists despite advancements in diabetic wound care. Small sample numbers, brief follow-up times, single-centre designs, and retrospective approaches constrain the generalizability and depth of findings in the majority of current studies(57)(58).
CONCLUSION
Diabetic wound healing is a multifaceted process that is significantly impaired by the metabolic and inflammatory disturbances characteristic of diabetes mellitus. Chronic hyperglycemia leads to impaired angiogenesis, endothelial dysfunction, oxidative stress, and a prolonged inflammatory response, all of which contribute to delayed wound closure, increased risk of infection, and higher rates of complications such as amputations and mortality.
Recent advancements in understanding how diabetic wounds develop have opened the door to more targeted and effective treatments. Innovative approaches like smart drug delivery systems, biodegradable polymers, hydrogels, platelet-rich plasma, and nanotechnology are helping improve blood flow, fight infection, and support tissue repair.
In the end, addressing the unique challenges of wound healing in diabetes is essential for improving patient outcomes, reducing healthcare burdens, and preventing serious complications associated with chronic wounds.
REFERENCES





Asher Gurung, Simran Gurung, Ankita Adhikari, John Saikia, Ashsis Sapkota, Wound Healing Mechanism in Diabetes, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 2343-2356. https://doi.org/10.5281/zenodo.19142546
 10.5281/zenodo.19142546
10.5281/zenodo.19142546
