Department of M.Pharm (Pharmacology), ITM Gida, Gorakhpur 273209
The treatment of peptic ulcer disease has changed dramatically since Helicobacter pylori-induced gastritis was identified as a significant contributing factor. One course of antimicrobial therapy that eradicates the H. pylori infection is more effective than ongoing suppression of acid secretion in preventing ulcer recurrence. It is widely recognized that Helicobacter pylori is the cause of chronic active type B gastritis and is likely the most prevalent bacterial infection in the world. While some people develop either a duodenal or gastric ulcer, many patients live with persistent superficial gastritis. A relatively little percentage of the lymphoid. In certain cases, the data indicates that chronic superficial gastritis advances to atrophy, the loss of gastric acid secretory capacity, and the formation of gastric cancer. In other cases, the reaction to H. pylori infection seems to progress to become a mucosal associated lymphoid tissue (MALT) lymphoma. Peptic ulcer disease (PUD) is most caused by Helicobacter pylori infection and nonsteroidal anti-inflammatory drug (NSAID) use. When there is a low risk of stomach cancer due to age under 55 and the lack of alarm symptoms, the test-and-treat approach for H. pylori detection is recommended.
The term "peptic ulcer" describes a condition in which there is a discontinuity in the entire thickness of the gastric or duodenal mucosa that persists because of acid and pepsin in the gastric juice.
Peptic ulcer disease differs from gastritis and erosions in that ulcers typically extend through the muscularis mucosa into the deeper layers of the submucosa. It is one of the common gastrointestinal disorders in clinical practice.
Gastric acid is a critical component of upper gastrointestinal tract complications including gastritis, erosions, and peptic ulcers.
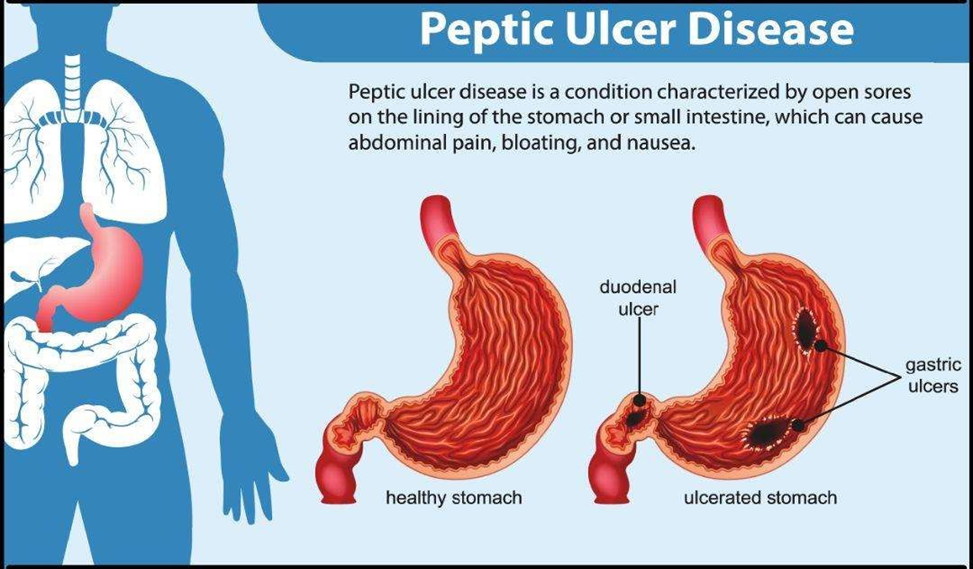
TYPES OF PEPTIC ULCER
1. Acute peptic ulcer
2. Chronic peptic ulcer
The Role of H. pylori in Peptic Ulcer Disease
The idea that H. pylori-induced gastritis plays a significant role in the development of peptic ulcer disease, particularly duodenal ulcers, is supported by three lines of evidence. More than 95 percent of patients with duodenal ulcers and more than 80 percent of patients with gastric ulcers are infected with H. pylori, except for those who have gastrointestinal conditions or are taking non-steroidal anti-inflammatory medications [3,4,5]. Patch closure or definitive surgery are the two main treatments for perforated ulcers. As stated earlier, simple closure is linked to an intolerably elevated ulcer recurrence rate [35]. Either patch closure or definitive surgery are the two main treatments for perforated ulcers. As was already established, simple closure is linked to an unacceptable rate of ulcer recurrence [6].
Hypotheses to Explain H. pylori-Negative Peptic Ulcer Perforations
Even when case-control studies are considered, the frequency of H. pylori infection in perforated peptic ulcers varies significantly among studies, as was previously demonstrated. These contentious findings could be caused by several factors, including variations in the frequency of NSAID use, the type of perforated ulcer under consideration (gastric or duodenal), the sensitivity and specificity of H. pylori diagnostic techniques, or the potential that the infection would have been eliminated by ulcer perforation management procedures.
NSAID USE
The concurrent use of NSAIDs, a known independent cause of ulcer complications, may be one reason why the prevalence of H. pylori in some ulcer perforation studies is lower than anticipated. Many studies, however, have not used a systematic questionnaire to prospectively measure NSAID use or to report the prevalence of H. pylori differently for patients who take NSAIDs and those who do not.
As an exception, Ng et al.’s study [7] showed intraoperative and antral biopsies revealed a 70% H. pylori infection rate in patients with perforated peptic ulcers; however, if NSAID users were taken out of the equation, this number increased to 80% (although the infection was found in only 23% of cases in patients using these medications). According to other research, NSAID use is common among individuals with perforated peptic ulcers, particularly those who are not infected [8].
Ulcer Site (Duodenal or Gastric Ulcer)
The most significant etiologic factor for non-complicated duodenal ulcers is H. pylori infection, although NSAIDs appear to have a less significant effect [9,10,11]. However, H. pylori infection is far less common in stomach ulcer disease, indicating that factors from the body—primarily NSAIDs—are to blame for a comparatively high percentage of stomach ulcers [12].
DIAGNOSIS OF INFECTION
Endoscopic biopsies of gastric mucosa or non-invasive techniques can be used to diagnose H. pylori infection of the stomach [13]. The clinical scenario determines which test is best for a particular patient. There are non-invasive techniques for diagnosing: serologic testing and urea breath tests are used to detect H. pylori infection. Enzyme-linked immunosorbent assays and other quick serologic tests can identify the circulating antibody response caused by a chronic infection [14–20]. These tests are almost as sensitive and specific as methods involving biopsy and have been adapted for use in the physician’s office [21].
TREATMENT OF INFECTION
It is challenging to completely remove H. pylori, and effective treatment necessitates the simultaneous use of two or more antimicrobial medications [22–25]. Eradication has typically been defined in therapeutic studies as the absence of organisms that can be detected by breath testing or tissue samples at least one month after treatment is finished [26,27]. The absence of infectious organisms during or just after therapy may simply indicate that the infection has been suppressed and may not indicate a long-term recovery [26,28].
Currently available treatment regimens for H. pylori do not completely eliminate the infection in all patients, and many of them have a comparatively high frequency of adverse effects. Novel therapies that use either brand-new medications or novel combinations of already-approved medications will undoubtedly be developed in the future. Numerous medication combinations are presently undergoing extensive testing. The necessity to evaluate novel agent combinations in infected humans complicates the research process because sensitivity in vitro does not accurately predict antimicrobial effectiveness in vivo [29–31].
Amoxicillin
Both in vitro and in vivo, H. pylori is extremely sensitive to amoxicillin. It has topical or intraluminal activity, inhibits the formation of bacterial cell walls, and is most effective when used in an acidic environment, though active when the pH is neutral [32].
Tetracycline
Tetracycline, which inhibits bacterial protein synthesis and, like amoxicillin, seems to act luminally or topically, is likewise highly effective against H. pylori. At low pH, it is active [33].
Clarithromycin
A macrolide antibiotic called clarithromycin prevents bacteria from synthesizing proteins. Although it has a comparable antibacterial range as erythromycin, it is more efficient against H. pylori, more acid-soluble, and better absorbed. Resistance may arise, just like with metronidazole, when only clarithromycin is administered [34].
CONCLUSION
All patients with confirmed peptic ulcer disease who exhibit signs of H. pylori infection should receive antimicrobial therapy against the bacteria. The first regimen—triple therapy using bismuth, metronidazole, and tetracycline—is the option chosen based on research that is currently available. Clarithromycin may be used in place of metronidazole for people who have a history of taking it.
Antisecretory medication is also advised for patients with active, symptomatic peptic ulcers to aid in healing and alleviate symptoms. Second-choice regimens combine an antisecretory agent with two antibacterial medications, such as metronidazole, amoxicillin, or clarithromycin. An H/K-ATPase antagonist, like omeprazole, is preferred.
It is not advised to use omeprazole in conjunction with a single antimicrobial medication, particularly amoxicillin, as this combination is less effective.
REFERENCES


Paro Kasaudhan, Dr. Suprabha Devi, The Role of the Helicobacter Pylori Infection in Ulcer Development and Treatment, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4010-4015. https://doi.org/10.5281/zenodo.18763060
 10.5281/zenodo.18763060
10.5281/zenodo.18763060
