1,2,6 Rameshwaram Institute of Technology and Management, Lucknow Uttar Pradesh-227202, India
3,4,5 J. S. Singh Institute of Pharmacy. Sitapur Uttar Pradesh-261207, India
Since its introduction in 1999 Rabeprazole is widely used Proton pump inhibitor for the treatment of a number of disease and conditions that are related to the excessive secretion of the gastric acid but still there is a strong need of a dosage form of rabeprazole that meets requirement of all age group of patients. There is a requirement of a stable formulation whose dose can be easily adjusted according to patient. The aim of this review is to describe the discovery and development of Rabeprazole, discuss the issues that arise during formulation of dosage form with rabeprazole and their possible solution, present approaches and future prospectives to develop new dosage forms of rabeprazole. The review also outlines the physicochemical properties of Rabeprazole. The review is majorly focused on the presentation of the state of the art in the development of novel formulations with Rabeprazole, it covers different approaches involved employed in this like Nanoparticles, Nanosuspension, Microparticles, Suppositories etc. The review anticipates the future possibilities in the formulation of new dosage forms of rabeprazole.
Rabeprazole is a benzimidazole substitution proton pump inhibitor, it has several differences in comparison to other proton pump inhibitors. Rabeprazole was developed by Eisai Co., Ltd., a Japanese pharmaceutical company. The drug was discovered through efforts to improve upon existing PPI medications like omeprazole and lansoprazole. Rabeprazole received approval from the United States Food and Drug Administration (FDA) for medical use in February 1999. Rabeprazole covalently binds with and inactivates the gastric parietal cell proton pump (H+/K+-ATPase).[1] It works by inhibiting the proton pump in the stomach's cells responsible for producing acid. This in turn inhibits gastric acid secretion and raises gastric pH. Rabeprazole is indicated in treatment and management of several disorders related to gastric acid such as-
Gastroesophageal Reflux Disease (GERD):
Rabeprazole is commonly prescribed to relieve symptoms such as heartburn, regurgitation, and difficulty swallowing associated with GERD.
Erosive Esophagitis:
It is effective in healing erosions or ulcers in the lining of the oesophagus caused by excessive acid exposure.
Duodenal Ulcers:
Rabeprazole is used to treat and prevent duodenal ulcers (ulcers in the first part of the small intestine) caused by Helicobacter pylori infection or the use of nonsteroidal anti-inflammatory drugs (NSAIDs).
Gastric Ulcers:
It is also used to treat and prevent gastric ulcers (ulcers in the stomach), again often related to NSAID use or H. pylori infection.[2]
While generally considered safe and well-tolerated, rabeprazole may cause side effects in some individuals, including headache, diarrhoea, nausea, abdominal pain, and dizziness. Long-term use of PPIs like rabeprazole has been associated with potential risks such as an increased risk of bone fractures, vitamin B12 deficiency, and certain infections. The safety of rabeprazole during pregnancy and breastfeeding has not been fully established. Pregnant or breastfeeding individuals should consult their healthcare provider before using rabeprazole. Rabeprazole should not be used in individuals with a known hypersensitivity to PPIs or any of its components. It should also be used with caution in patients with severe liver impairment.[3]
FORMULA

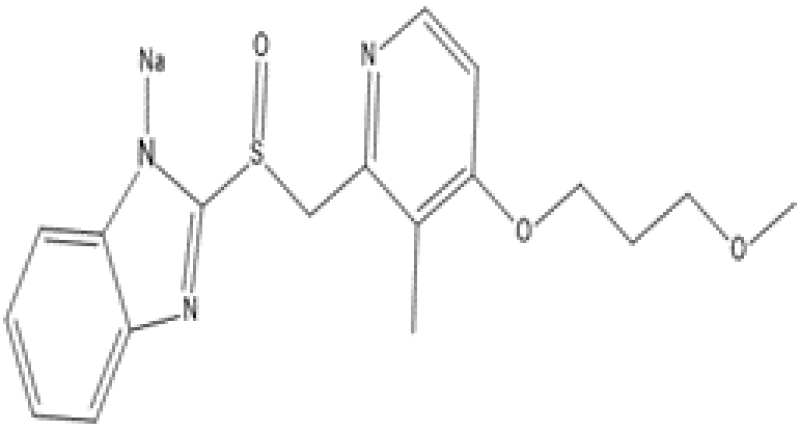
Figure 1: Rabeprazole Base Structure

Figure 2: Rabeprazole Salt Structure (Rabeprazole Sodium)
PHARMACOKINETICS AND PHARMACODYNAMICS
Mechanism of action of rabeprazole is same as other proton pump inhibitors. Proton pump inhibitors are benzimidazoles substitute, they have same basic structure. Being inactive compound Proton pump inhibitors require activation in the low pH of parietal cells to suppress the activity of the proton pump.[4,5,10] The formulation containing proton pump inhibitor are needed to be protected from gastric acid with enteric coating to avoid their premature activation in the stomach after oral administration. PPIs are absorbed from duodenum and transported to the canaliculi of parietal cells through blood stream. Once absorbed from the proximal small intestine these readily cross parietal cell membranes to enter the highly acidic (pH 1) parietal cell canaliculus. At low pH, proton pump inhibitors become protonated and converted to hydrophilic. This selectively hold them and leads to their activation to sulphenamide form within the canaliculus. The activated sulphenamide form binds covalently to the extra cytoplasmic cysteine residues of alpha subunit of H+, K+-ATPase leads to irreversibly inhibiting H+, K+-ATPase activity and gastric acid secretion.[6,7]
MEDICINAL USES
Rabeprazole can be used in the treatment and prevention of different gastrointestinal diseases, such as:
FACTORS TO BE CONSIDERED WHILE FORMULATING DOSAGE FORM WITH RABEPRAZOLE
The formulation of medicinal products that contain Rabeprazole, is a difficult process due to the low water solubility of Rabeprazole and stability problems. The main factors that effects the formulation of Rabeprazole are-
Physicochemical Properties:
The molecular structure of Rabeprazole is mainly based on the 2-pyridylmethylsulfinyl-benzimidazole moiety (Figure 2). Rabeprazole exists in several states of protonation which depends on the pH of the solution. Therefore, Rabeprazole exhibit two or three pKa values. The range of first value of pKa is 3.55 to 4.77 that is associated with the acceptance of protons in an acidic environment in the nitrogen atom of pyridine and second in presence of alkalis which is due to the dissociation of a proton from the benzimidazole ring. Chirality is another important aspect of the chemical structure in Rabeprazole. All PPIs contain an asymmetric sulfur molecule in the sulfinyl group, which helps in binding pyridine to the benzimidazole group. That’s why proton pump inhibitor can exists in both S- or R- enantiomers and also as racemates and so Rabeprazole. Both S- & R- enantiomeric forms of Rabeprazole are equally pharmacodynamically active.[9]
Stability:
Stability of Rabeprazole and other Proton pump inhibitors are affected by some physical and chemical factors such as-
Acidic Environment:
Rabeprazole is stable in basic environment (pH above 7.0) but highly unstable in acidic environment i.e. decompose very quickly. Rabeprazole and other PPI needed to be enteric coated for avoiding their pre-mature activation in gastric acid.[11]
Light:
Gracia et al observed that rabeprazole degrades and a new product formed when rabeprazole is exposed to UVC.[11] the experiment involves exposure of rabeprazole methanolic solution to UVC-254 nm for 1 hr.
Temperature:
Temperature had a direct effect on the stability of the Rabeprazole. Different research had shown that the PPI solution are stable on storage at low temperature but their stability decreases as the temperature increases.[12,13]
Presence of Salt:
Different studies had shown that the presence of other ion like phosphate, acetate etc has significant and different effect on different PPIs. The stability of Rabeprazole may increase or decrease depending upon the ion present.[14,15]
Interaction With Another Drugs:
Different studies were performed to understand the interaction of rabeprazole with other drug. The studies shows that rabeprazole interact significantly with several drugs like acetylsalicylic acid, clopidogrel, methotrexate etc.
DIFFERENT FORMULATION OF RABEPRAZOLE AVAILABLE ON MARKET
There are a number of formulations of rabeprazole that are available in market. The formulation presently available in market are mainly based on two basis and most important route of administration i.e. Oral and Parenteral.
The presently marketed products of rabeprazole are based on conventional dosage forms. The major part of rabeprazole market product includes-
PAST WORK ON FORMULATION OF RABEPRAZOLE
In recent past a large number of studies had been carried out to develop a new formulation with Rabeprazole. These researches were mainly focused on to develop a formulation with Rabeprazole that shows enhancement in efficacy, safety, stability, quality and acceptability. The stability of rabeprazole in acidic environment is a major area of concern as all PPIs get pre activated in acidic pH before their absorption and become ineffective, this is the most important point which should be kept in mind while formulating dosage form with rabeprazole and other PPIs.
In the researches performed in past the routes of administration that are most used are oral and parenteral although some research also involves alternative route of administration like rectal, topical etc. These formulations include –
Sublingual Tablet:
Abraham Sindhu et al 2010 had developed sublingual tablets of Rabeprazole by wet granulation method. For quantitative evaluation of interaction and main effect quadratic model was used. Crospovidone and Croscarmellose Sodium were used as super disintegrants and mannitol was used as diluent, for purpose of sweetening agent Sodium Saccharin was employed and for enhancing the flow property talc was used.[16]
Solanki Kinjal P. et al 2020 had developed Sublingual tablets for oromucosal delivery as oromucosal drug delivery shows faster pharmacological action by rapid absorption and high bioavailability. The Sublingual tablet was prepared with carrier particle covered with fine dry particle of rabeprazole sodium by direct compression method. Mucoadhesive polymer used was HPMC K4M.[17]
Floating Microspheres:
Delayed Release Multiparticulates:
Buccal Tablet:
Mucoadhesive Enteric Coated Tablet:
Mucoadhesive Microcapsules:
Sustained Release matrix tablets:
Pulsatile Drug Delivery System:
Buffered Tablets :
Enteric Coated Tablet:
The enteric coating is done to prevent the disintegration of tablet in stomach this is done to avoid pre-activation of rabeprazole in acidic environment of stomach. If PPIs get released in stomach after pre-activation the become inactive so enteric coting prevents their release in stomach leads to drug release in intestine at basic pH where drug gets absorbed.
Delayed Release Tablet:
Mouth Dissolving Tablet:
Raft Forming System:
Transdermal Patches:
Immediate Release Tablet:
Buccal Film:
Different route of administration and polymer used in different formulations of rabeprazole are given in the table below

Table 2: Route of administration and Polymer used in different formulation
DEVELOPMENT OF NEW FORMULATION WITH RABEPRAZOLE
Rabeprazole was discovered in 1986 and was approved for medical use in 1997. Sence then many research were performed on rabeprazole and many formulations are proposed to enhance its stability, safety and efficacy. There is a lack of dosage form of the rabeprazole that may be suitable for all paediatric groups. There are many conventional dosage forms of rabeprazole but in recent years newer dosage forms like nanoparticles, microparticles etc have gained the interest of researchers. Some Formulation which gains interest in recent years and could be a great area of interest as rabeprazole formulation in future are-
Nanoparticles:
Nanoparticles had gained the attention of researchers a lot in field of pharmacy due to their unique properties that can be tailored for various applications. Nanoparticles are biodegradable and bio compatible. One of the most prominent applications of nanoparticles in pharmacy is drug delivery. Nanoparticles can encapsulate drugs, protecting them from degradation and improving their solubility and bioavailability. Additionally, nanoparticles can be engineered to target specific cells or tissues, allowing for targeted drug delivery and reducing systemic side effects. Nanoparticles can be designed to release drugs in a controlled manner over an extended period. This controlled release can improve the efficacy and safety of drugs by maintaining therapeutic levels in the body and reducing the frequency of dosing. Theragnostic nanoparticles combine diagnostic and therapeutic functions in a single platform. They enable simultaneous imaging and drug delivery, allowing for personalized medicine approaches and real-time monitoring of treatment response. Nanoparticles can serve as carriers for vaccines, enhancing their stability, immunogenicity, and targeted delivery to immune cells. This can lead to improved vaccine efficacy and the development of novel vaccination strategies. Overall, nanoparticles offer versatile and promising solutions for various challenges in pharmacy, ranging from improving drug delivery and efficacy to advancing diagnostic and therapeutic approaches. Ongoing research in nanoparticle-based drug delivery systems continues to expand the possibilities for innovative pharmaceutical interventions.[37]
Nano Suspension:
Nanosuspensions are a type of colloidal dispersion consisting of submicron-sized drug particles suspended in an aqueous or non-aqueous liquid medium, typically stabilized by surfactants or polymers. These nanoparticles are typically in the size range of 10 to 1000 nanometres. Nanosuspensions have gained significant attention in the field of pharmacy due to their potential to overcome challenges associated with poorly water-soluble drugs, such as low bioavailability and variable therapeutic efficacy. Nanosuspensions increase the surface area of drug particles, leading to improved dissolution rates and enhanced solubility of poorly water-soluble drugs. This can result in better bioavailability and therapeutic outcomes. By reducing particle size, nanosuspensions can enhance the physical and chemical stability of drugs that are prone to degradation, aggregation, or crystallization.[41]
Nanosuspensions can be engineered to target specific sites within the body, such as tumours or inflamed tissues, by modifying their surface properties or incorporating targeting ligands. This enables localized drug delivery and minimizes systemic side effects. Nanosuspensions can be formulated using various manufacturing techniques, including high-pressure homogenization, media milling, and precipitation methods. This flexibility allows for the development of nanosuspensions for a wide range of drugs and therapeutic applications. Nanosuspensions can be administered via different routes, including oral, intravenous, intramuscular, and subcutaneous routes, depending on the specific drug and therapeutic indication. Despite their potential benefits, scaling up the production of nanosuspensions for commercialization can pose challenges related to reproducibility, stability, and manufacturing costs. Addressing these challenges requires careful optimization of formulation and processing parameters. Nanosuspensions represent a promising approach for improving the delivery of poorly water-soluble drugs in pharmacy, offering opportunities for enhanced therapeutic outcomes and patient care. Ongoing research and development efforts continue to explore new applications and address the challenges associated with the formulation and commercialization of nanosuspensions.[42]
Microparticles:
Microparticles play a significant role in drug delivery systems. These are small particles with diameters typically ranging from 1 to 1000 micrometres. They can be made from various materials such as polymers, lipids, proteins, or inorganic materials like metals or ceramics. Microparticles offer several advantages in pharmaceutical applications Microparticles can be designed to release drugs in a controlled manner, either through diffusion, degradation, or a combination of both. This allows for sustained release formulations, minimizing dosing frequency and reducing side effects. Encapsulation of drugs within microparticles can protect them from degradation in the body, ensuring stability and maintaining their therapeutic efficacy. Functionalization of microparticles with ligands or antibodies allows for targeted delivery to specific tissues or cells, increasing drug concentration at the site of action while minimizing systemic exposure.[45] Microparticles can enhance the bioavailability of poorly soluble drugs by increasing their solubility and dissolution rate, thereby improving absorption and therapeutic outcomes. Microparticles serve as scaffolds for tissue regeneration and engineering by providing a substrate for cell attachment, proliferation, and differentiation. They can be loaded with growth factors or other bioactive molecules to enhance tissue regeneration. Microparticles can be functionalized with probes or markers for diagnostic purposes, such as imaging or detection of biomarkers, pathogens, or specific cell types. Microparticles are used as carriers for vaccine antigens, providing protection and controlled release to enhance immune response and efficacy.
Microparticles offer versatile platforms for drug delivery and various other pharmaceutical applications, contributing to advancements in therapy, diagnostics, and tissue engineering.[46]
Renata Platcheck Raffin et al 2007 had developed microparticle of pantoprazole with aim to develop a formulation that provide controlled release to the drug. He technique used to prepare microparticle of pantoprazole was Emulsion/solvent evaporation method. Polymer used for the preparation of microparticle was Eudragit S 100.[47]
Transdermal Drug Delivery:
Transdermal drug delivery involves the administration of drugs through the skin for systemic distribution. This method offers several advantages over traditional oral or injectable routes. Transdermal delivery avoids the pain and discomfort associated with injections and the inconvenience of swallowing pills, making it more patient-friendly. Transdermal patches can provide controlled and sustained release of drugs over an extended period, maintaining constant plasma drug levels and reducing the need for frequent dosing. By bypassing the gastrointestinal tract and liver, transdermal delivery can avoid first-pass metabolism, leading to improved bioavailability of certain drugs. Transdermal delivery can minimize gastrointestinal side effects and fluctuations in drug levels compared to oral administration, leading to better tolerability and compliance. Transdermal patches are easy to apply and remove, requiring minimal effort on the part of the patient. This convenience can improve adherence to treatment regimens. Transdermal patches can be designed to deliver drugs locally to specific sites, such as for pain relief or skin conditions, while minimizing systemic exposure and side effects. Transdermal patches can incorporate multiple drugs, allowing for combination therapy and improved treatment outcomes for conditions requiring complex medication regimens. Despite these advantages, transdermal drug delivery also has limitations, including limited drug permeability through the skin, the need for drugs with suitable physicochemical properties, and potential skin irritation or sensitization. However, ongoing research and development efforts aim to overcome these challenges and expand the utility of transdermal delivery systems in clinical practice.[49] Soral Manisha et al 2021 had formulated transdermal patches containing Rabeprazole sodium. The polymer employed for the development of transdermal patches were Hydroxy Propyl cellulose, PVP K-30, PVP K-90 (for formation of film) and PEG 400 (plasticizer). Tween 80 was used as permeation enhancer.[36]
Suppositories:
Suppositories are solid dosage forms intended for insertion into body orifices, usually the rectum, vagina, or urethra. They are designed to deliver medications locally or systemically, depending on the drug and its intended therapeutic effect. Suppositories can be composed of various bases, including cocoa butter, glycerinated gelatine, polyethylene glycol, or a combination of these. The choice of base depends on factors such as drug compatibility, melting point, stability, and patient preferences. The drug release from suppositories depends on factors such as the physicochemical properties of the drug, the composition of the suppository base, and the physiological conditions at the site of insertion. Suppositories can release drugs through dissolution, diffusion, or a combination of both. Suppositories offer several advantages, including avoidance of first-pass metabolism, rapid onset of action, and improved patient compliance, especially in cases where oral administration is not feasible or practical. Despite their advantages, suppositories may cause local irritation or discomfort upon insertion, and they may require specialized training for proper administration. Additionally, some patients may find them socially or culturally unacceptable.
Petra Bestebreurtje et al 2020 had developed Suppositories of omeprazole with the aim of to provide a treatment for hyperacidity in infants. The base used for formulation of suppository were witepsol H15 and arginine.[50]
Hydrogel:
Hydrogels are three-dimensional network structures composed of hydrophilic polymers that can absorb and retain large amounts of water or biological fluids. Hydrogels are widely employed as drug delivery systems due to their ability to encapsulate and release drugs in a controlled manner. Drugs can be incorporated into the hydrogel matrix either through physical entrapment or chemical conjugation. The swelling and dissolution properties of hydrogels can be tailored to control the release rate of drugs, offering sustained or targeted delivery to specific tissues or organs. Hydrogels can also prolong the residence time of drugs in the eye, enhancing their therapeutic efficacy. Hydrogels are explored for oral drug delivery to improve the bioavailability and controlled release of drugs. They can protect drugs from degradation in the gastrointestinal tract, enhance their solubility and absorption, and provide targeted delivery to specific regions of the gastrointestinal tract. Hydrogels are used in topical formulations such as creams, gels, or patches for the delivery of drugs to the skin. They provide hydration and occlusion, enhancing drug penetration into the skin and improving the therapeutic outcomes of dermatological treatments. Hydrogels offer versatile platforms for drug delivery, wound healing, tissue engineering, and diagnostic applications in pharmacy and biomedicine. Their tunable properties make them attractive candidates for a wide range of pharmaceutical and biomedical applications.
CONCLUSION
Despite being discovered more than 20 years ago and its efficacy in treatment and prevention of several gastrointestinal disorder like Peptic ulcer, Crohn’s Disease, Acid reflux disease etc there are certain issues that are not solved yet. As mentioned, in the review there are several approaches that can be useful in eliminating problems like stability, etc associated with the rabeprazole but there still remains room for improvement. Availability of a formulation of rabeprazole for children and all medical conditions is the most important issue that needed to be resolved. There is a lack of dosage form of the rabeprazole that may be suitable for all paediatric groups due to this, practices like opening capsules to withdraw their content, preparing dispersion of capsule content in some random media etc leads to the degradation of the drug or optimum quantity of drug did not reach the systemic circulation. Hence there is a strong need to develop a formulation that is suitable for paediatric administration. The route of administration on which most researches were performed is oral route of administration but in recent year other novel routes of administration like Transdermal drug delivery, Buccal Drug delivery, etc had gained interest of researchers. The polymer which are most used in the formulation of rabeprazole sodium dosage form are HPMC and Eudragit based polymers.
REFERENCES





Aman Kumar Singh, Alka Verma, Ram Sevak Verma, Ramnivas, Suraj Mishra, Pranjul Verma, Formulation of Dosage Forms with Rabeprazole: Challenges and Future Perspectives, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 3, 932-946. https://doi.org/10.5281/zenodo.10868683
 10.5281/zenodo.10868683
10.5281/zenodo.10868683
