1,2,4,5Sri Venkateswara University College of Pharmaceutical Sciences, Sri Venkateswara University, Tirupati, Andhra Pradesh, India-517502.
3Seven Hills College of Pharmacy, Tirupati
A Review on Lidocaine
Clinically, lidocaine, a local anaesthetic of the amide class, is used to block pain perception. [1,2]. Lidocaine possesses antinociceptive, antiarrhythmic, anti-inflammatory, and antithrombotic properties when administered systemically. Lidocaine uses mechanisms that are separate from its main mechanism of action, sodium channel inhibition, to produce these effects in both acute and chronic pain situations as well as acute respiratory distress syndrome.
Structure of lidocaine:
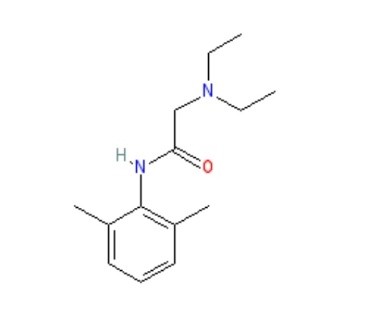
According to the Vaughan-Williams classification, lidocaine is a class Ib antiarrhythmic agent, and its use is indicated in the management of acute ventricular tachyarrhythmia. Lidocaine has long served as the foundation for local anaesthesia, providing efficient pain management for a variety of operations, from minor surgery to dental procedures. With a molecular weight of 234.3 g/mol and log p equal to 2.84, lidocaine is a low soluble and good penetrating medication (Biopharmaceutical Classification System class II), making it a good choice for cutaneous delivery. The most popular, dependable, and efficient amide derivative is this one. Because of its advantageous qualities, including its minimal systemic toxicity, intermediate duration of action, and low risk of allergic responses, lidocaine is prepared as a topical medication. Nils Lofgren initially synthesised lidocaine in 1935 in Professor Hans von Euler’s laboratory in Stockholm. Lofgren then started testing the compounds he and his colleagues had created [3]. When Lofgren tried the 57th compound in 1943, he discovered that it quickly numbed his tongue. According to Goldberg’s (toxicology) and Gordh’s (clinical data) publications, which suggested that lidocaine had a potent and surprising anaesthetic effect, the patent for Xylocaine® was granted in Sweden on May 11, 1948. In November 1948, the Food and Drug Administration authorised the use of Xylocaine® in the United States [4]. Clinical trials conducted by Torsten Gordh showed that lidocaine was a notable advancement above procaine, which at the time was the gold standard for treating surgical pain [5,6]. For the treatment of ventricular arrhythmias, neuropathic pain alleviation, and surgical discomfort, this amide-class anaesthetic is still often employed [7,8]. Along with its anti-arrhythmic and local anaesthetic uses, lidocaine also offers analgesic qualities for several pain problems. The ability of intravenous lidocaine (IVL) to alleviate complicated regional pain syndrome, hyperalgesia, and peripheral neuropathic pain was well acknowledged in the 1980s. Late-onset and insufficient local anaesthetic action are the main issues with using commercial lidocaine preparations. According to reports, commercial creams and gels cannot effectively transport lidocaine base (or its HCl salt) through undamaged skin. To overcome these issues, it is necessary to increase the skin’s permeability to lidocaine given topically. Topical anaesthetics such as lidocaine are frequently utilised for localised pain management during medical and cosmetic treatments. Conventional formulations often suffer from systemic absorption hazards, poor penetration, and short duration of action.
Table 1:Physicochemical Properties:
|
IUPAC Name |
2-(Diethylamino)-N-(2,6Dimethylphenyl)Acetamide. |
|
Formula |
C14H22N2O |
|
Molecular Weight |
234.34 |
|
Melting Ranges |
68-69.0°C. |
|
Colour, Odour |
White Odourless Substances. |
|
Crystal Forms |
The Base Crystallizes From N-hexane as Fine Needles While the Hydrochloride Is Obtained as A Microcrystalline Powder from Aqueous Acetone |
|
Solubility |
Insoluble In Water. Soluble In Ethanol, Methanol, Acetic Acid, Diethyl ether, Dimethyl Sulfoxide. |
|
Rheological Behaviour |
Ensures Ease Of Application And Stability During Storage |
|
pH Compatibility |
Maintains Skin Compatibility And Prevents Irritation |
|
Drug Release Profiles |
Controlled-Release Systems Improve Therapeutic Outcomes and Reduce Dosing Frequency. |
Mechanism of action of lidocaine:
When used as a local anaesthetic, lidocaine works by blocking voltage-gated sodium channels (VGSCs), which reversibly stops action potentials from propagating. Lidocaine inhibits the priming of human peripheral PMNCs and neutrophils, for instance, which has an impact on inflammatory cells in vitro [9]. Additionally, lidocaine can decrease the release of pro-inflammatory mediators such as TNF-?, IL-4, and IL-6. Lidocaine reduces inflammation by preventing the release of histamine, leukocyte metabolism, and the expression of pro-inflammatory cytokines [10]. Lidocaine works by inhibiting NF-k? activation and the cytokine storm that follows [11]. Lidocaine dramatically lowers TNF-? levels in comparison to vehicle-treated controls. By controlling cellular metabolic activity, migration, exocytosis, and phagocytosis through reversible interactions with membrane proteins and lipids, it also has anti-inflammatory effects by reducing the accumulation of PMN (polymorphonuclear) granulocytes in the lung[12]. By preventing human peripheral polymorphonuclear cells or neutrophils from priming, lidocaine has an impact on inflammatory cells in vitro [13,14]. Lidocaine also could decrease mediator release. The antiarrhythmic effect's underlying mechanism seems to be like procaine's. As dosage increases, conduction time slows, refractory period lengthens, and ventricular excitability decreases. Therapeutic dosages do not reduce cardiac contractility[15]. Doses of lidocaine that result in similar increases in the diastolic stimulation threshold do not lower myocardial contractility or lower blood pressure, in contrast to procaine and procaine amide. Before the approval of amiodarone, the Advanced Cardiac Life Support (ACLS) algorithm included lidocaine as the main medication of choice for treating ventricular fibrillation (VF) or ventricular tachycardia (VT). Although lidocaine had been used for years to treat VF/VT, there was no proof that it was more effective than other medications. Lidocaine is still regarded as a good substitute for amiodarone in cases of cardiac arrest from VT/VF, even if it was later taken out of the ACLS Algorithm[16]. Other mechanisms allow lidocaine to produce extra analgesic effects. Numerous studies demonstrate that systemic lidocaine can be used as an analgesic during surgical procedures, particularly laparoscopic abdominal surgery. Lidocaine is often given at first dosages of 1.5–2 mg/kg BW and thereafter at 1.5–3 mg/BW/hr or 2-3 mg/min. As a result, serum lidocaine levels vary from 0.5 to 5?g/ml (~2–21 ?M), like what happens following epidural treatment. Lidocaine has several advantages, such as a speedy recovery, shorter hospital stays, unaffected bowel motions, and less pain following surgery.[17]. The effects of lidocaine on the central nervous system include blocking nicotinic and acetylcholine receptors, blocking opioid receptors, blocking presynaptic calcium channels in the dorsal root ganglion, blocking neurite growth, blocking muscarinic cholinergic receptors, and blocking substance P from attaching to receptors on natural killer (NK) cells[18,19]. Lidocaine is also effective in treating COVID-19. By lowering the cytokine storms linked to COVID-19, nebulised lidocaine seems to be a novel treatment for alleviating lung harm caused by the virus, potentially reversing ARDS. Therefore, additional pre-clinical studies and clinical trials are needed to better characterise the safety and effectiveness of lidocaine in treating individuals with severe acute respiratory distress syndrome (ARDS) brought on by COVID-19.
Pharmacokinetics of lidocaine:
The pharmacokinetics of lidocaine, which encompasses the processes of absorption, distribution, metabolism, and excretion of the drug, is crucial for ensuring its safe and effective application in clinical settings.
Absorption:
Distribution:
Lidocaine exhibits extensive distribution throughout the body, with significant concentrations observed in the heart, lungs, liver, and kidneys. It demonstrates a high degree of protein binding, predominantly to albumin. The volume of distribution for lidocaine is approximately 1-2 liters per kilogram of body weight.
Metabolism:
The metabolism of lidocaine primarily occurs in the liver, facilitated by the enzymes CYP3A4 and CYP1A2. This process results in the formation of two principal metabolites: monoethylglycinexylidide (MEGX) and glycinexylidide (GX). Notably, MEGX is an active metabolite that may enhance the anesthetic and antiarrhythmic properties of lidocaine.[20.21.22].
Excretion:
Lidocaine and its metabolites are predominantly eliminated through the kidneys via urine, with approximately 90% of the drug being cleared within a 24-hour period.[23]
Factors Influencing Pharmacokinetics:
Various factors can influence the pharmacokinetics of lidocaine, including:
Age: The pharmacokinetics of lidocaine may be modified in infants, children, and older adults.
Liver function: Impaired liver function due to disease can hinder the metabolism of lidocaine, resulting in elevated plasma levels and a risk of toxicity.
Kidney function: Renal impairment can affect the excretion of lidocaine and its metabolites, leading to increased plasma concentrations.
Drug interactions: Certain medications may interact with lidocaine, thereby impacting its pharmacokinetics. The pharmacokinetics of lidocaine are intricate and subject to influence from multiple factors. Recognizing these factors is crucial for the safe and effective administration of lidocaine.
Administration:
Adult Dosage:
Specific Patient Populations:
Hepatic impairment: The guidelines established by the American Association for the Study of Liver Diseases indicate that a lidocaine patch may be utilised for pain management in patients suffering from decompensated cirrhosis; however, it is advised to exercise caution in such cases[28,29,].
Renal impairment: Typically, dosage modifications are not required for individuals with renal impairment, as the absorption of topical lidocaine is minimal.
Pregnancy considerations: Lidocaine is believed to traverse the placenta through passive diffusion. The American College of Obstetricians and Gynecologists (ACOG) considers the use of local anaesthesia, including lidocaine with or without epinephrine, to be safe for treating oral conditions during pregnancy[30]. The maximum recommended dosage for lidocaine is 4.5 mg/kg (300 mg) for plain formulations and 7 mg/kg (500 mg) when combined with epinephrine[31]. It is important that a pregnant woman is not denied necessary surgical procedures or that such procedures are not postponed due to her pregnancy, as delays could adversely affect both her and the foetus. Current research suggests that exposure to anaesthetic or sedative agents in utero does not seem to impact foetal brain development. Furthermore, animal studies have not indicated any negative effects from limited exposures lasting less than three hours.
Breastfeeding considerations: Following continuous intravenous infusion, epidural administration, or high-dose local anaesthesia, the concentrations of lidocaine in breast milk remain low, thereby posing minimal risk to breastfeeding infants. Consequently, it is improbable that lidocaine will result in adverse effects for infants who are breastfed, and no specific precautions are warranted. The potential for lidocaine to interfere with breastfeeding, especially when used alongside other anaesthetics and analgesics, is a topic of discussion, influenced by the variability in research designs and methodologies. With appropriate support for breastfeeding, the use of epidural lidocaine in conjunction with opioids generally has a negligible effect on the success of breastfeeding, although the administration of labor pain medication may postpone the initiation of lactation[32].
Pediatric patients: Neonates exhibit an underdeveloped metabolic clearance system, which heightens their susceptibility to the accumulation of drugs and their metabolites. Furthermore, the levels of ?1-acid glycoprotein in neonates and infants are significantly lower, with the concentration of AAG at birth being approximately 50% of that found in adults. This condition leads to a greater unbound fraction of lidocaine, a prolonged elimination half-life, and an elevated risk of accumulation, especially during continuous infusions.[33] In Pediatric patients, the administration of topical lidocaine must be approached with caution to avoid the risk of overdose. The maximum allowable dose is determined by the patient's weight or age for otherwise healthy children over the age of 3 years. For infants and children under 3 years, the application of no more than 1.2 mL of the 2% solution is recommended, ensuring a minimum interval of 3 hours between doses and a cap of 4 doses within a 12-hour period.
Systemic lidocaine infusions have been widely recognized for their efficacy in managing postoperative acute pain in pediatric patients; however, their validation for other forms of pediatric pain remains limited. The NMDA antagonist characteristics of lidocaine may offer advantages in addressing challenging pain conditions, including mixed nociceptive-neuropathic pain and central sensitization. The typical dosing regimen for these scenarios involves an initial bolus of 1.5 mg/kg, followed by a continuous infusion of 1 mg/kg/hr, with higher dosages often employed in pediatric oncology contexts. Further research is essential to evaluate the safety and efficacy of lidocaine infusions in children and to refine dosing guidelines for various pain types. Additionally, it is crucial to investigate the significance of monitoring plasma levels during continuous infusion[34].
Older Patients: In the case of older patients, local anaesthesia should be the primary choice for surgical interventions. It is advisable to use the minimum effective volume and concentration to mitigate the risk of systemic toxicity. For lidocaine, a concentration of 10 mg/mL is recommended, with a maximum dosage not exceeding 5 mg/kg. This strategy ensures effective local anaesthesia for numerous surgical procedures while minimizing the likelihood of postoperative complications[35].
Monitoring:
Adverse Effects:
Drug-Drug interactions:
Contraindications:
Warnings and Precautions:
Lidocaine viscous: Severe adverse events, including seizures, cardiopulmonary arrest, and fatalities, have been documented in children under the age of 3 due to the inappropriate use of lidocaine viscous 2%. This medication is contraindicated for treating teething pain and should only be utilized in this demographic when no safer alternatives are available[42]. It is imperative to strictly follow dosing guidelines and ensure secure storage to minimize associated risks. This boxed warning issued by the FDA specifically addresses these concerns and does not apply to all formulations, such as intravenous lidocaine. Previous research has indicated that lidocaine can suppress premature ventricular complexes (PVCs) and nonsustained ventricular tachycardia (NSVT), which were believed to be precursors to ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT). However, recent studies have associated the prophylactic use of lidocaine for PVC suppression with increased mortality rates following acute myocardial infarction, likely due to a rise in asystole and bradyarrhythmias, resulting in the discontinuation of routine prophylactic administration. Observational studies suggest that while lidocaine may reduce the recurrence of VF/pVT after the return of spontaneous circulation (ROSC), it does not enhance survival rates and offers no advantage for patients experiencing non-shockable rhythms[43].
Toxicity:
Signs and Symptoms of Overdose:
Management of Overdose :
CONCLUSION:
In conclusion, Lidocaine is an important choice for pain relief and antiarrhythmic effects with a favourable safety profile. This review examines its history, pharmacokinetics, mechanism of action, administration, drug interactions, contraindications, adverse effects, toxicity and clinical applications. It also assesses lidocaine use in pain relief, anaesthesia and cardiology. It also discusses different administration forms i.e., injectable, topical and oral with special benefits. This review provides a bit of knowledge regarding lidocaine’s characteristics for healthcare experts and analysts pointing to optimize its clinical applications.
REFERENCES

Swetha Meeniga, Nagaveni Pommala*, Saravanakumar Kasimedu, Mounika Gandham, Pranuth Atthoti, A Review on Lidocaine, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 1, 949-960. https://doi.org/10.5281/zenodo.14636911
 10.5281/zenodo.14636911
10.5281/zenodo.14636911
