Samarth College of Pharmacy Deulgaon Raja
Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), commonly termed Long COVID, denotes a constellation of symptoms persisting or emerging beyond the acute phase of COVID-19. PASC encompasses a heterogeneous clinical presentation affecting multiple organ systems and poses significant challenges to health care delivery and public health. Despite increasing recognition, precise pathophysiology, diagnostic criteria, and evidence-based therapeutic strategies remain incompletely defined. This review synthesizes current knowledge on PASC epidemiology, clinical manifestations, putative mechanisms, diagnostic considerations, management strategies, and future research directions. Recognizing PASC as a global health priority, we emphasize the need for standardized case definitions, multidisciplinary care models, longitudinal cohort studies, and mechanistic investigations to inform effective interventions
The Coronavirus Disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has resulted in profound morbidity and mortality worldwide. Although acute COVID-19 manifestations have been the primary focus of clinical and research efforts, there is increasing recognition of a subset of individuals who experience prolonged or new-onset symptoms after recovery from the acute phase (Nalbandian et al., 2021). These persistent symptoms are collectively referred to as Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) or Long COVID (World Health Organization [WHO], 2021). PASC represents a major post-pandemic challenge with substantial implications for patient quality of life, health care systems, and societal productivity.
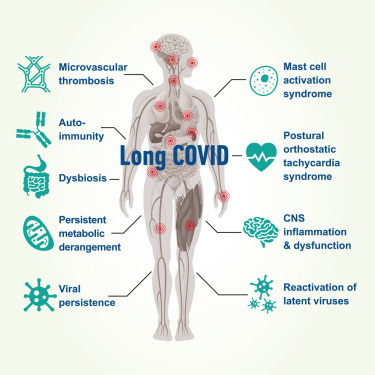
Figure 01 Biological mechanisms underpinning the development of long COVID
The purpose of this review is to provide a comprehensive synthesis of the current understanding of PASC, including epidemiological patterns, clinical characteristics, underlying mechanisms, diagnostic challenges, and contemporary approaches to management. The review highlights gaps in knowledge and outlines future research priorities necessary to improve patient outcomes.
2. Terminology and Case Definitions
A major impediment to PASC research and clinical care is the absence of a universally accepted definition. Several organizations have proposed working definitions based on symptom duration after acute infection:
The variability in definitions affects prevalence estimates and research comparability. Harmonization of case definitions is essential for consistent surveillance, clinical trials, and epidemiological research.
3. Epidemiology
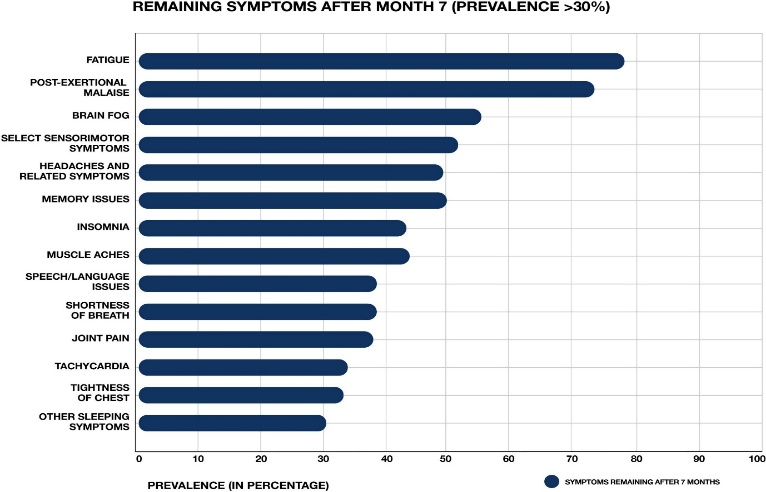
Figure 1 illustrates the prevalence of persistent symptoms reported in post-COVID-19 cohorts, highlighting fatigue, dyspnea, and cognitive dysfunction as the most common manifestations of PASC
Estimating the prevalence of PASC is challenging due to differing definitions, study methodologies, and populations. Nevertheless, multiple cohort studies suggest that a significant proportion of individuals recovering from SARS-CoV-2 infection experience persistent symptoms.
Population-based studies indicate that approximately 10% to 30% of people with confirmed SARS-CoV-2 infection report PASC symptoms lasting beyond four weeks (Sudre et al., 2021). Among hospitalized patients, symptom persistence appears even more common, with reports of up to 50% of individuals experiencing sequelae at six months (Huang et al., 2021). Common risk factors for PASC include older age, female sex, higher acute disease severity, and preexisting comorbidities such as diabetes, obesity, and cardiovascular disease (Al-Aly, Xie, & Bowe, 2022).
These findings underscore the broad impact of PASC across varied clinical settings and highlight the importance of continued surveillance.
4. Pathophysiological Mechanisms
The mechanisms underlying PASC are multifaceted and not yet fully elucidated. Proposed pathways include:
Table 1. Common Symptoms in PASC
|
System |
Symptom |
Reported Prevalence (%) |
|
General |
Fatigue |
30–60 |
|
Respiratory |
Dyspnea |
20–45 |
|
Neurological |
Cognitive impairment |
15–40 |
|
(Adapt with latest studies) |
4.1 Persistent Viral Antigen or RNA
Several studies have detected SARS-CoV-2 RNA or viral proteins in tissues weeks to months after acute infection, suggesting viral persistence could sustain inflammatory responses (Chertow et al., 2021).
4.2 Immune Dysregulation and Chronic Inflammation
Aberrant immune activation has been observed in PASC, characterized by elevated cytokines, altered T-cell profiles, and prolonged inflammatory signaling (Phetsouphanh et al., 2022). These immunological perturbations may contribute to ongoing symptomatology.
4.3 Endothelial Dysfunction and Coagulopathy
SARS-CoV-2 is associated with endothelial injury and a hypercoagulable state. Microvascular dysfunction could underpin multi-organ symptoms, including fatigue, dyspnea, and cognitive impairment (Fogarty et al., 2021).
4.4 Autonomic Nervous System Involvement
Autonomic dysregulation, including postural orthostatic tachycardia syndrome (POTS), has been reported in PASC cohorts and may explain symptoms such as palpitations and dizziness (Dani et al., 2021).
4.5 Organ-Specific Pathologies
Direct viral effects and secondary immune responses may lead to lasting damage in organs such as the lungs (pulmonary fibrosis), heart (myocarditis), kidneys (acute kidney injury sequelae), and brain (neurocognitive impairment) (Nalbandian et al., 2021).
The interplay between these pathways likely varies among individuals, contributing to the heterogeneous clinical manifestations of PASC.
5. Clinical Manifestations
PASC manifests with a wide array of symptoms that can persist or develop after initial recovery from acute COVID-19. Although the clinical presentation is variable, common symptoms include:
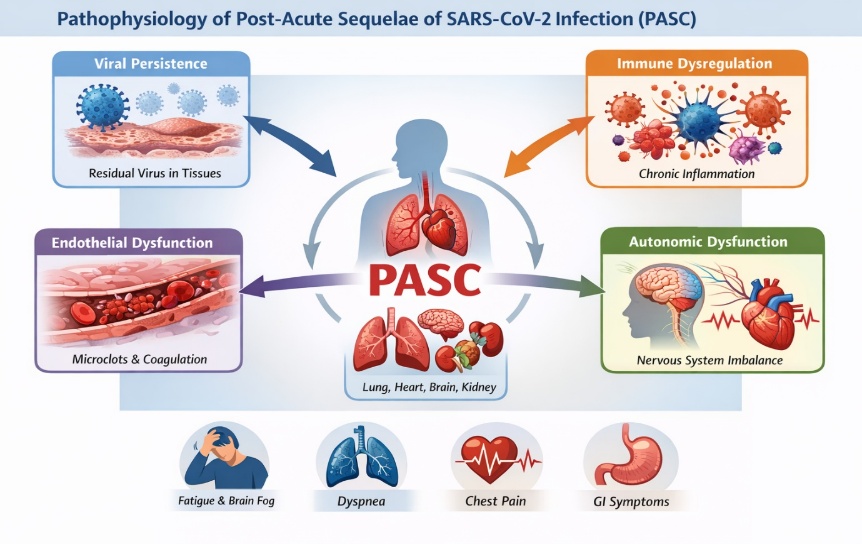
Figure 01 Schematic of proposed PASC pathophysiology (immune dysregulation, viral persistence, endothelial injury).
5.1 General and Systemic Symptoms
5.2 Respiratory Symptoms
5.3 Cardiovascular Symptoms
5.4 Neurological and Cognitive Complaints
5.5 Gastrointestinal Manifestations
5.6 Mental Health Sequelae
The multisystem nature of PASC emphasizes the need for comprehensive evaluation and multidisciplinary care.
6. Diagnosis and Assessment
There is no specific diagnostic test or biomarker for PASC. Diagnosis is primarily clinical and requires careful evaluation to exclude alternative explanations. A structured approach includes:
Validated symptom questionnaires and standardized outcome measures are increasingly used in research settings to quantify symptom burden and functional impairment.
7. Management Strategies
Management of PASC is primarily supportive and symptom-directed in the absence of disease-modifying therapies.
7.1 Rehabilitation and Physical Therapy
Individualized rehabilitation programs, including cardiopulmonary rehabilitation and graded physical activity, may improve functional capacity. However, care must be taken to avoid exacerbating symptoms in patients with post-exertional malaise.
7.2 Symptom-Based Management
7.3 Pharmacologic Interventions
No medications are currently approved specifically for PASC. Emerging clinical trials are evaluating:
7.4 Psychological Support
Psychological interventions, including cognitive behavioral therapy (CBT) and counseling, are recommended for patients with mood disorders, anxiety, or trauma-related symptoms.
8. Impact on Quality of Life and Society
PASC exerts a profound impact on patient quality of life, daily functioning, and socio-economic productivity. Persistent symptoms causing disability can lead to prolonged absence from work, increased health care utilization, and psychological distress (Al-Aly et al., 2022). Health systems must adapt to manage the growing burden of chronic sequelae post COVID-19.
9. Research Gaps and Future Directions
Despite significant advances, critical gaps remain:
Future research must integrate clinical investigation, basic science, and patient-centered outcomes to develop evidence-based interventions.
CONCLUSION
Post-Acute Sequelae of SARS-CoV-2 Infection (PASC) is a complex and heterogeneous condition with significant clinical and public health implications. Persistent symptoms affecting multiple organ systems may endure for months after the resolution of acute COVID-19, leading to substantial morbidity. A comprehensive understanding of PASC requires multidisciplinary research efforts, standardized diagnostic criteria, and tailored management strategies. Addressing this challenge will improve recovery trajectories and quality of life for individuals affected by Long COVID.
REFERENCES





Khushi Kayande, Anuradha Kendhale, Pratiksha Jaybhaye, Devanand Dongre, Dr. Prafulla Tathe, Post-Acute Sequelae of SARS-CoV-2 Infection (PASC): A Comprehensive Review, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3883-3889. https://doi.org/10.5281/zenodo.18754946
 10.5281/zenodo.18754946
10.5281/zenodo.18754946
