Gupta College of Technological Sciences, Asansol, West Bengal, India
Smiling depression, also known as high-function depression, represents a troubling dichotomy, where individuals outwardly project happiness while enduring profound inner anguish. Unlike conventional depression, which is typically marked by symptoms like visible sadness and withdrawal, those suffering from smiling depression meticulously craft a facade of well-being, making it exceedingly difficult to detect and diagnose. Unlike traditional depression, those suffering from smiling depression maintain a facade of normalcy, often excelling in work, social interactions, and daily responsibilities. This condition is particularly insidious, as it frequently goes unnoticed by those closest to the individual, including friends, family, and even healthcare professionals, resulting in delayed intervention and heightening the risk of severe outcomes, such as suicidal ideation. The societal stigma surrounding mental health compels individuals to maintain this deceptive disguise, further complicating the identification and treatment of smiling depression. This presentation delves into the complexities of this condition, exploring its symptoms, underlying causes, and the psychological mechanisms that enable sufferers to conceal their true emotions. By recognizing the signs and offering compassionate support, we can help those with smiling depression dismantle their pretense and seek the help they need. This work highlights the urgent need to destigmatize mental health and promote a more empathetic approach to psychological well-being.
Depression is one of the most common mental health concerns that impacts around three hundred million people in our society. One of the most dangerous forms of hidden depression is smiling depression, wherein the individual seems outwardly happy while hiding their suffering from the world. In many cases, the individuals may wear a mask of happiness or contentment, constructing a wall around their true feelings, making it hard to notice and diagnose them. It is an atypical type of depression with symptoms coinciding with depressive disorders, but it is not clinically recognized yet. Psychiatrists see that this new, yet unrecognized disorder is very much on the rise in the young generation or working individuals, and their symptoms are just quite the opposite of the symptoms of classic depression, like lethargy, sorrow, and hopelessness. These individuals appear perfect from the outside; they are active, high functioning with a good work-life balance, optimistic, and cheerful all day. As per the Diagnostic and Statistical Manual of Mental Disorders – V (DSM- V) criteria, the person must have five or more symptoms (major) during the same 2-week period for depressive disorders. [1] According to the DSM-5 criteria, a diagnosis of major depressive disorder requires the presence of at least five or more major symptoms during the same two-week period. These symptoms must include either a depressed mood or a loss of interest or pleasure, alongside other symptoms such as changes in appetite, sleep disturbances, fatigue, feelings of worthlessness, difficulty concentrating, or recurrent thoughts of death. The symptoms must significantly impair daily functioning and cannot be attributed to substance use or other medical conditions. But in these cases, the following symptoms may not match or maybe the opposite in the patients suffering from smiling depression.
Smiling depression has some characteristic features that are completely different from the classic one.
They are as follows:
Apart from the various factors associated with the delayed diagnosis, another factor mostly overlooked is the stigmas attached to the disease. Individuals with smiling depression conceal their emotional symptoms due to stigmas like fear of being labelled as attention-seeking, weak, or vulnerable, fear of being judged, fear of being discovered, fear of suicidal intentions, persistent stress, anxiety, difficulty in functioning, feeling guilty, worthless, and insomnia, etc. Several life events and personality features may predict susceptibility to smiling depression. People with high conscientiousness and perfectionism often put on a calm or "happy" front because they do not want to bother other people or have elevated expectations of themselves. These issues often challenge individuals to conceal their emotional symptoms and prevent them from seeking the help they need. No case study was found as such because this mental disorder is not yet officially recognized in the diagnostic manual for mental disorders. These characteristics often go unnoticed, leading to delayed diagnosis and a heightened risk of self-harm, including a potential for suicide.
2. Diagnosis and Help
Diagnosing Smiling Depression is a complex process because it lacks the overt sins associated with other depressive disorders. Those affected often mask their feelings and symptoms, keeping a socially fit or even cheerful appearance, which can lead friends, family, and clinicians to overlook their distress. Unlike more visible forms of depression, individuals with smiling depression are high functioning, excelling at work, keeping social connections, and meeting daily responsibilities, all while struggling with inner sadness or feelings of emptiness. Due to their functionality, those with this condition are likely to keep the energy and organizational skills that other people with more disabling depressive symptoms might lose, so their risk is more unpredictable and possibly more deadly if not diagnosed and treated early. Standard diagnostic tools, like the Beck Depression Inventory or the Patient Health Questionnaire-9 (PHQ-9), may help show symptoms, yet they sometimes miss nuanced signs in high-functioning individuals [3]. Healthcare providers must depend on prudent, inquiring conversations to figure out any latent depression, emptiness, or suppressed distress that may not be detected by regular questionnaires. A key diagnostic marker is a disconnection between their outwardly positive behaviour and inner emotional struggles, as they may still experience a lack of joy or enthusiasm in things that once interested them. Another notable concern is the elevated risk of suicide in smiling depression. The contribution of muscles toward making a smiling or joyful face can be used to diagnose the patient if the distinction between a forced and a natural smile is familiar to the masses with sensitization.
In smiling depression, the tendency to put a happy face always forces people to put a fake smile on their faces. The Duchenne smile, renowned as a genuine or emotional smile, engages the zygomatic major and the orbicularis oculi muscles, creating a more natural, friendly, and happy appearance [4]. The forced or fake smile involves:

A Diagram of The Facial Muscles
Diagnosing Smiling Depression Through Facial Muscle Activity [5]
Facial expressions serve as powerful indicators of emotional states, and their analysis can unveil concealed psychological conditions, such as smiling depression. In this paradoxical state, individuals mask profound sadness behind a facade of cheerful expressions. The Facial Action Coding System (FACS), developed by Paul Ekman, is still the gold standard for systematically decoding facial movements by mapping them to specific muscle activities known as Action Units (AUs). For example, a genuine Duchenne smile—characteristic of authentic joy—engages the zygomaticus major (AU12), which elevates the corners of the mouth, and the orbicularis oculi (AU6), responsible for crinkling around the eyes. However, individuals experiencing smiling depression often show controlled or non-Duchenne smiles, where the eyes stay disengaged, betraying their underlying emotional distress despite an outwardly positive demeanor. To streamline the analysis, researchers have introduced Region Units (RUs), which consolidate facial areas, such as the brows, eyes, and mouth, for localized examination. Modern techniques like Active Appearance Models (AAM) employ statistical algorithms to precisely track and analyze these regions in video recordings, measuring subtle shape and texture changes in real-time. These measurements are classified by sophisticated classifiers like MultiBoost, which classifies facial expressions into broad categories (e.g., happiness, sadness, anger) and subtle expressions (e.g., controlled smiles, concerned looks). Automation renders the process objective, eliminating human error and subjective bias.
Several key metrics are used in this method:
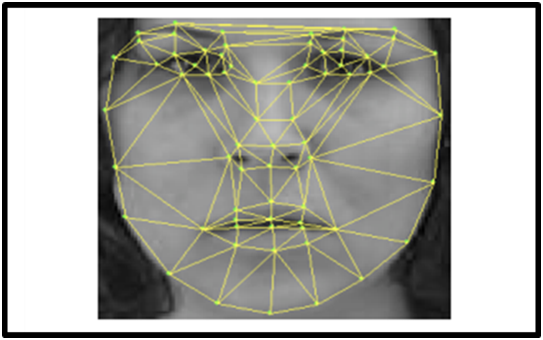
Face mesh is used to group AUs
3. Treatment and Support
The treatment of smiling depression requires approaches that address both the concealed emotional pain and the outwardly well-functional lifestyle of the individual. Increasing awareness is the first and foremost step to destigmatize the issue with enforcement of the need to recognize and support those struggling with smiling depression.
3.1 Role of Family: Family encouragement is critical in helping those with smiling depression by offering an empathetic and understanding space where they feel free to express themselves. Families can be a strong, positive force in their recovery journey by providing consistent emotional support, validating their feelings, and offering gentle guidance toward professional help. Family members can provide unique forms of support and a strong foundation that complements formal therapeutic approaches, making a significant difference in the healing journey.
It can be understood by the following points below:
Establishing a culture that values and promotes candid and open communication is the first step in family encouragement. Many people who suffer from smiling depression have a great need to keep appearances, often repressing their actual feelings to spare their loved ones from anxiety or hardship. Family members lessen the need to hide symptoms when they express that all emotions are normal and acceptable. It might make the person feel comfortable enough to show vulnerability if told that melancholy, tension, or other challenging feelings are normal. Families may promote trust and empower individuals to express their genuine emotions without worrying about negative consequences by making eye contact, paying close attention, reacting with empathy, and using open-ended communication rather than condemnation.
The inhibitions developed because of stigmas attached to the issue that make people reluctant to get professional help should be addressed first to encourage them to consider getting help and remind them that therapy is a positive step toward self-care and well-being. It can be done by taking mini steps like volunteering to find an appointment with the therapist, going with them for their sessions, developing coping mechanisms to minimize the stressors, etc.
For individuals with smiling depression, the stability and unconditional support of family are deeply reassuring. These charted individuals are often plagued with feelings of self-doubt or worthlessness, and encouragement from family serves as an integral counterbalance when family serves as a counterbalance, helping reinforce thoughts of belonging and worth. Family members can play a crucial role by helping to counteract the negative self-perception many people suffering from smiling depression experience actively reminding them of their strengths, accomplishments, and positive attributes. They need to feel secure, and constant statements of love, gratitude, and reassurance help them ground themselves.
4. Cultural and Societal Influence
The cultural and societal norms surrounding smiling and emotional expression play a significant role in the diagnosis of smiling depression. Across cultures, smiling is not only an expression of inner contentment but a social process shaped by deeply rooted norms and values as well. Smiling in America, for instance, is closely associated with cheerfulness and good vibes, such that social norms expect individuals to adopt a friendly and open demeanor. This "ethic of cheerfulness" promotes smiling even when facing difficulties, generally masking inner turmoil?. [9] Such cultural norms can make it challenging to identify smiling depression, as individuals may appear outwardly content while concealing profound emotional pain. In contrast, collectivist cultures like Japan prioritize keeping social harmony. Here, smiles often serve as a mask for negative emotions to avoid disrupting group cohesion. The concept of wa, or social harmony, drives individuals to display controlled emotions, including polite or masking smiles in situations where they may be experiencing sadness or distress?. [9] While this cultural norm fosters societal stability, it complicates the recognition of smiling depression, as outward emotional restraint is culturally prescribed rather than indicative of emotional well-being. Similarly, in Polish culture, the smile is deeply tied to sincerity, and smiling in social contexts is often reserved for moments of genuine happiness. This cultural emphasis on emotional authenticity may create fewer barriers to diagnosing smiling depression, as deviations from expected emotional transparency can be more easily noticed?. [9] Social "display rules," i.e., cultural norms regarding the expression of feelings in a specific social situation, also regulate the visibility of smiling depression. In individualistic cultures like the United States, where the presentation of the self in the best light is very much emphasized, smiles can convey social competence as well as confidence. Social pressures of this sort lead people to conceal their actual feelings, and hence diagnosis becomes more challenging? [10] Collectivist societies, on the other hand, encourage emotional restraint to maintain group cohesion, which can suppress outward displays of distress and delay help-seeking behaviour. Gender roles also intersect with cultural roles, which add another layer of complexity. Women are socialized to smile more, in line with societal expectations of submissiveness and politeness. This added pressure on women to smile can hide smiling depression symptoms, as women's smiles will hide societal expectations rather than their true emotional state. Men, who are not necessarily socialized to be vulnerable, will smile less, and thus there can be other problems with the identification of depressive symptoms?. [10]
5. Cost of Treatment
The study on the "Cost Burden of Treatment Resistance in Patients with Depression" offers a stunning look at the financial and clinical toll of treatment-resistant depression (TRD). It’s quite striking to see just how much more expensive and complex it becomes to treat depression when patients don’t respond to standard therapies. The fact that TRD patients face around 40% higher medical costs underscores the need for early identification and alternative approaches for those at risk. Overall, research highlights a broader issue in healthcare: the considerable hidden costs associated with inadequate first responses to treatment. For mental health conditions, especially, this study suggests that investing in targeted treatment adjustments and patient monitoring could pay off significantly, both in cost savings and, more importantly, in patient quality of life. It’s an important reminder that health outcomes and economic impact often go hand in hand, and studies like this could pave the way for smarter, more compassionate care strategies. [17] The study on the Cost of Depression sheds light on the significant financial and personal impacts of managing major depression, particularly the role that treatment adherence and patient response play in healthcare costs and quality of life. It’s eye-opening to see those indirect costs, primarily from lost productivity, make up the vast majority (87%) of total costs, far outweighing drug costs. One of the most striking findings is the difference in costs between patients who respond to treatment and those who don’t. Responders experience not only a better quality of life but also significantly lower costs, largely due to reduced sick leave. This highlights the importance of effective treatment approaches that prioritize response rates. [18] This document is both insightful and practical: while depression treatment has an upfront cost, its economic and societal benefits make it a worthwhile investment. Employers have a real incentive to support better mental health care, as the improvements in productivity and well-being could offset much of the expense. If more effort were made to integrate effective treatment into standard primary care and to create incentives for high-quality depression management, we’d likely see both economic benefits and improved lives. [19] One of the key insights from this study is that patients who respond well to treatment incur much lower costs, around 39% less, than those who don’t. This isn’t just a matter of financial savings—it means that patients who respond to treatment are likely feeling better and can participate more fully in their daily lives. Although adherence alone didn’t seem to lower costs, the boost in quality of life among those who stuck to their medication is encouraging and points to the broader benefits of effective treatment and patient commitment. [18]
6. Intersectional Perspectives
6.1 Hormonal and Biological Factors That Lead to Depression
This topic highlights the role of biological factors like hormones and their role in diagnosing depression. The three key diagnostic tests are the dexamethasone suppression test (DST), the response of the thyroid stimulating hormone (TSH) to thyrotropin-releasing hormone (TRH), and responses of growth hormone (GH).
DST and Depression:
In nearly 50% of the patients suffering from endogenous depression, hypersecretion of cortisol has been found, especially during nighttime and the following morning. [15] The DST evaluates how efficiently the suppression of cortisol in the body occurs following the administration of a synthetic steroid known as dexamethasone. Depressed patients are liable to show rapid normalization of cortisol levels, which suggests abnormal regulation in cortisol.
TSH responses to TRH:
Patients with depression may show a subnormal TSH response to TRH injection, but this phenomenon is seen only in some subsets, whose definition is still less clear than desired. In clinical studies, it has been seen that patients with depression may show a subnormal thyroid-stimulating hormone (TSH) response to thyrotropin-releasing hormone (TRH) injection. This phenomenon is of particular interest because it suggests a potential link between the hypothalamic-pituitary-thyroid (HPT) axis and mood disorders. However, this response is not uniformly observed in all individuals with depression, indicating variability among patient subsets.
GH Responses:
Depressed patients have a deviating GH response to some stimuli, such as insulin and amphetamines, which may be indicative of dysfunction in the non-adrenergic system. However, the results are inconclusive at this point and need more research to prove the possible therapeutic and prognostic importance. [15]
6.2 Gender, Race, Lgbtq+ Perspectives
Women: Major Depressive Disorder (MDD) is almost twice as common in women as in men, especially during their childbearing years. About 17% of people will develop MDD in their lifetime, and women are more likely to do so at 21%. Social stress is more likely to place women at risk for depression. [1] There is a moderate genetic component to MDD, particularly in females, which suggests a heightened sensitivity to stress.[2] Fluctuations in estrogen and progesterone throughout the reproductive cycle—such as during menstruation, pregnancy, postpartum, and menopause—significantly affect mood and can drive MDD (Major Depressive Disorder).[2] These hormonal changes can activate neurobiological processes, particularly influencing neurotransmitters like serotonin, which play a crucial role in mood regulation. Marital status and employment: Single, divorced mothers and working mothers who are the subjects of salient marital conflict or role overload are more likely to have increased depressive symptoms. Sociocultural role expectations can also cause such events. Low social support, especially during stress-laden periods like pregnancy, postpartum, or when ill, can cause precipitating episodes of depression. Women are more vulnerable to depression because they are more exposed to stress, trauma, and sexual assault. Such events can precipitate maladaptive coping, which most commonly presents as rumination. Such a condition occurs in approximately 13% of women after childbearing and can persist for many months if left untreated. Risk factors include lower socioeconomic status, physical illness, and relationship tension. [3] Race and Depressive Symptoms: In India, the concept of race can be somewhat nuanced, often overlapping with caste and regional identities. Like findings in U.S. studies, there may be variations in how depressive symptoms manifest and are addressed across distinct groups. For instance, marginalized communities may face higher levels of stigma and fewer resources for mental health support, which can exacerbate depressive symptoms and impact mortality risk. Understanding these dynamics is crucial for addressing mental health disparities. [9]
LGBTQ+ Perspectives: Minority stress is often cited as a cause of mental health disparities (higher levels of depression along with high suicidal thoughts) among lesbian, gay, and bisexual (LGB) youth. [4,5] It was observed in an interpersonal-psychological study conducted among a group of gender and sexual-oriented (cisgender/transgender and LGBTQ+ students). Feeling burdensome, pride issues, lack of belongingness, and victimization, along with the pressure to stand as labeled “normal” among the population, are the common factors pushing them towards mental problems. However, the specific processes or mechanisms behind these disparities are not well-studied. These findings have implications for understanding and addressing mental health disparities in this population. [4,5]
6.3 Age-Related Perspectives:
Depression in Adults: Accurate diagnosis and treatment of depression rely on evidence-based approaches. Depression is a complex condition characterized by diverse symptoms, including sadness, loss of interest or pleasure (anhedonia), and suicidal tendencies. Comprehensive assessment methods are essential to ensure correct understanding and management of the disorder. In contrast, SCID (Structured Clinical Interview for DSM Disorders, offers a more detailed and standardized evaluation. Although highly reliable for diagnosing mental disorders, including depression, SCID interviews are time intensive. A shorter alternative is the MINI (Mini International Neuropsychiatric Interview), which balances thoroughness and efficiency. Evidence-based assessments should address key depressive symptoms like low mood and suicidality. They should also evaluate specific subtypes (e.g., melancholic, atypical, and seasonal depression), track the progression and chronicity of symptoms, and find any comorbid conditions. Tools like the LIFE (Longitudinal Interval Follow-Up Evaluation) are particularly useful for monitoring symptom patterns over time. It is crucial to differentiate between suicidal thoughts and actual plans or preparations for suicide, as the latter is a stronger predictor of immediate risk. By integrating tools like the SCID and MINI with longitudinal tracking methods, clinicians can achieve a holistic understanding of a patient’s condition and provide targeted treatment tailored to their specific needs. [14]
Depression in kids:
It encompasses three studies aimed toward the assessment of the internal structure of the CDI (Children’s Depression Inventory) and its link to demographic variables as well as the social behavior of children. The Children’s Depression Inventory (CDI) has gained significant importance in recent years due to the alarming rise in mental health problems among children and adolescents, even those with seemingly sound lifestyles. Despite advancements in healthcare, education, and access to resources, young individuals are increasingly vulnerable to depression and related disorders, influenced by various societal and technological changes.
Work, study, and peer pressure: Modern life demands peak performance from children and adults alike. Academic expectations have skyrocketed, with students facing immense pressure to excel in studies, take part in extracurricular activities, and secure a competitive edge for future careers. Simultaneously, social pressures from peers often exacerbate feelings of inadequacy, isolation, or low self-worth.
Increased Screen Time: The shift toward technology-based education, particularly post-pandemic, has drastically increased screen exposure. Digital platforms, though effective for learning, often lead to prolonged hours of screen time. While gaining knowledge from various online sources, students can experience mental fatigue, eye strain, and reduced social interactions. Additionally, the rise of gaming systems, many of which are designed with addiction-prone mechanics, further consumes children's time and fosters unhealthy habits, affecting sleep cycles, physical activity, and emotional well-being.
Changing Social Dynamics: The prevalence of social media platforms amplifies peer pressure. Constant exposure to curated, idealized versions of others' lives can lead to comparison, feelings of inadequacy, and a decline in self-esteem. Moreover, cyberbullying and online harassment are emerging as significant stressors for young individuals. The outcome of this study provides a strong indicator of the association between social skills deficits and depressive symptoms in that it would guide treatment interventions. [16]
7. Future Areas to Be Explored
Overall, the cultural scripts surrounding smiling influence the presentation and perception of smiling depression. In cultures where smiling is strongly associated with happiness or politeness, the condition becomes harder to diagnose, as the outward appearance of positivity can easily mask internal struggles. To address these challenges, culturally sensitive diagnostic tools and mental health frameworks are essential. These tools must account for the diverse ways in which emotional expressions are shaped by societal norms, ensuring that smiling depression does not go unnoticed in those who silently endure its effects. It is a silent struggle, so anyone who is suffering from it should be supplied with professional help. Hence awareness programs on a massive scale are the utmost necessary step along with the elimination of the risk factors mentioned in the article. Alternative holistic treatment systems, like nature-based, hobby-based systems, and dietary management complementary to professional help, are the potential areas that can be explored.
CONCLUSION:
Ultimately, this article dispels the misconception that depression and smiling depression are synonymous, highlighting their distinct differences. It underscores the critical need for awareness, as misdiagnosis of this condition poses a serious risk to the patient’s well-being. Open discussions about smiling depression are essential to fostering a supportive environment for those struggling with it. The article advocates for a more compassionate and informed approach to mental health, urging the eradication of societal stigmas to facilitate timely intervention and comprehensive support for affected individuals.
ACKNOWLEDGEMENT:
The authors express their sincere appreciation to the other authors who have contributed to the research on this condition. We are particularly grateful to the medical practitioners who have done the correct documentation and diagnosis for their patients and raised awareness of this rising condition of smiling depression.
CONFLICT OF INTEREST:
The authors declare no conflicts of interest related to this article.
REFERENCES



Anubhava Kumar Burnwall*, Krishnendu Ghosh, Anshu Jha, Smiling Depression: When A Smile Hides the Pain, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 569-580. https://doi.org/10.5281/zenodo.15150111
 10.5281/zenodo.15150111
10.5281/zenodo.15150111
