1Department of Pharmaceutics, R. G. Sapkal College of Pharmacy, Anjaneri, Nashik, Maharashtra 422301.
2Department of Pharmaceutics, Brahma valley college of pharmacy Nashik, Maharashtra 422301
Recently, nanobiomedicine a fascinating topic with enormous potential to transform cancer detection and treatment methods has emerged from the nexus of nanotechnology and biomedical research. The goal of this novel combination of biology, medicine, and nanotechnology is to develop therapeutic and diagnostic agents that are safer and more effective, especially in the field of theranostics for different types of cancer. The most prevalent malignant primary brain tumor is glioblastoma multiforme (GBM), which occurs in 3.19 cases per 100,000 person years. With a 5-year survival rate of 7.2%, glioblastoma multiforme (GBM), a WHO grade IV glioma, is the most prevalent malignant primary brain tumor. Treatment has been extremely difficult because of its highly infiltrative nature, genetic variability, and blood brain barrier (BBB) protection. Chemoradiotherapy and surgical excision are the usual treatments for GBMs. Resistance to all available treatment approaches is enhanced by the strong DNA repair and self-renewing properties of glioblastoma cells and glioma initiating cells (GICs), respectively.
1.1 Glioblastoma multiforme
Glioblastoma (GBM), is a grade IV astrocytoma that spreads quickly and violently (1). There are four classes of gliomas according to the World Health Organization (WHO): Low-grade gliomas, such as oligodendrogliomas, gangliogliomas, dysembryoplastic neuroepithelial gliomas, and mixed gliomas, are classified as grade one and two tumors. High-grade gliomas are categorized as malignant gliomas (WHO three and four), which include anaplastic astrocytoma, oligodendrogliomas, ependymomas, glioblastomas, and gliosarcomas. The prognosis is worse and malignant gliomas have become more aggressive. Less than 5% of grade IV patients lived after five years (2,3). they make up only 2% of all cancers, primary malignant central nervous system (CNS) tumors are frequently linked to high rates of morbidity and death. Gliomas and nongliomas are two categories of CNS malignancies. Nongliomas include the infrequently occurring CNS germ cell tumors, as well as a number of malignant and usually non-cancerous tumors. Astrocytomas, oligodendrogliomas, ependymomas, and glioblastomas are the most prevalent types of gliomas (4). Astrocytoma with a WHO grade 4, or GBM, is the most prevalent histologic subtype of diffuse gliomas and makes up around half of all primary malignant brain tumors.
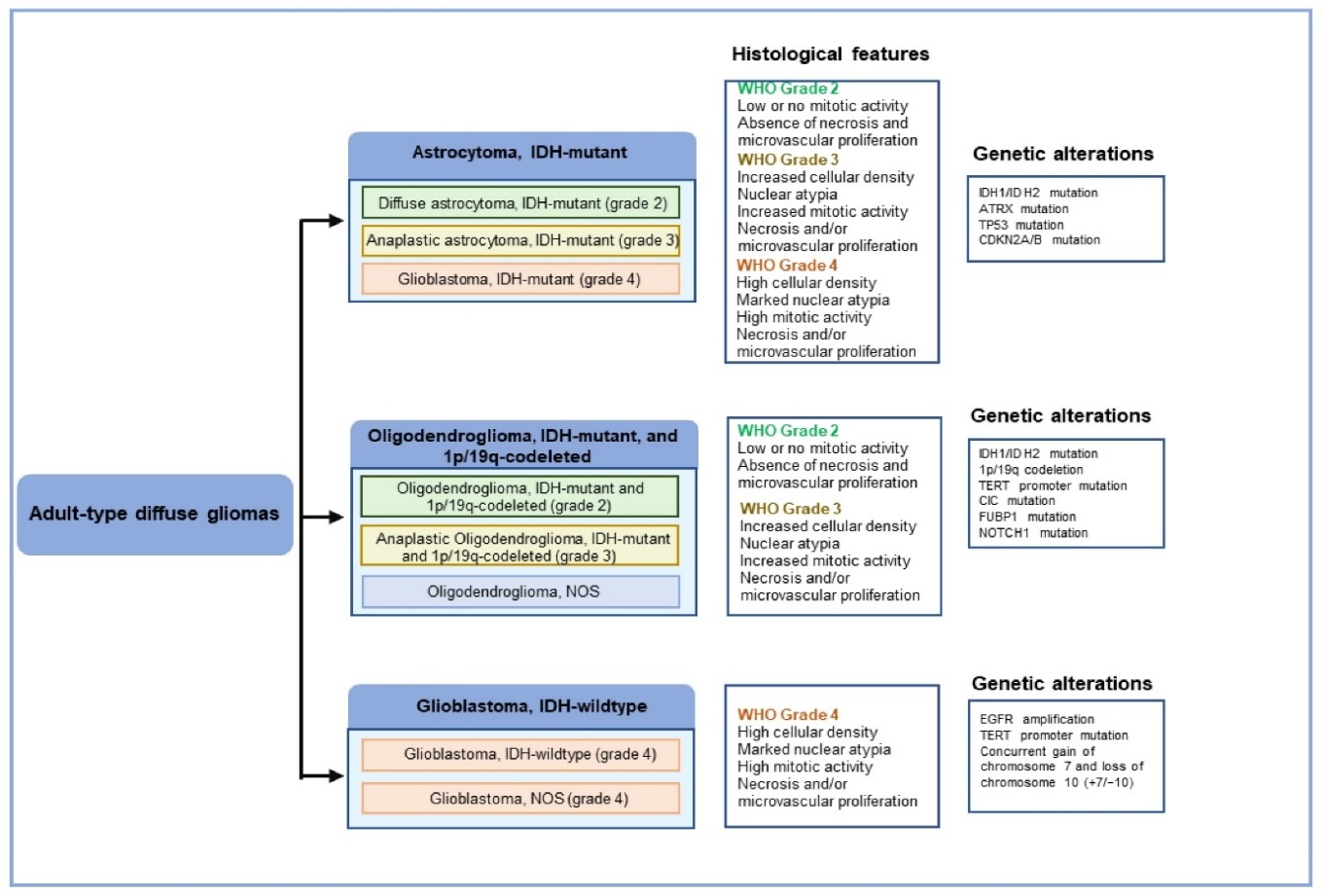
Fig 1: - WHO grade 4, or GBM, is the most prevalent histologic subtype of diffuse gliomas
The purpose of this study is to investigate population-based survival rates for LGG patients in the United States by beginning treatment and usual patient demographics. The latest data on tumor and patient genotype and its impact on survival after an LGG diagnosis is next examined (5). Depending on where they originate, brain tumors can be classified as primary or metastatic. Primary brain tumors are those that start inside the skull, whereas the latter is self-explanatory. The WHO's CNS-5 classification divides CNS tumors into six classes, which include: 1) Adult-type diffuse gliomas (most primary brain cancers, such as (a) glioblastoma multiforme (GBM),
IDH-wild type, (b) oligodendroglioma, IDH-mutant and 1p/19q-codeleted, and (c) astrocytes, isocitrate dehydrogenase (IDH)-mutant 2) Diffuse low-grade gliomas of the paediatrics kind (prognoses excellent) 3) Aggressive diffuse high-grade gliomas of the pediatric kind 4) Astrocytic gliomas that are circumscribed (have a solid growth pattern) 5) Tumors of neurons and gliopolin (with neural differentiation) and 6) Ependymomas. Thes is important to explain a few broad changes in grading before talking about specific tumors. The first is the switch to Arabic numerals for WHO grades, which were formerly displayed in Roman numerals (6,7).
Major brain malignant neoplasms such as Glioblasts (GB) (World Health Organization (WHO) Grade 4) are associated with poor prediction. Intermediate overall survival is 12-18 months in patients eligible for maximum safe resection, followed by adjuvant radiation and chemotherapy with temozolomide (TMZ) [1]. The average survival rate over 5 years is less than 6% [2]. The main concern of GB is its pronounced resistance to treatment and the high probability of recurrence. This contributes to tumor initiation, regrowth and treatment resistance mechanisms. Recurrent GB is usually inaccessible to surgical resection due to tumor invasion and invasion of nearby brain structures [3].
Treatment for GB has occurred in recent decades.Several adjuvant treatment options have been developed. In other words, topical drugs such as Carmustin Depots (Gliadel®) that release therapeuticcoal mine concentrations up to 120 hours postoperative time [4] have been developed and administered systemically with chemotherapy such as temozolomide and nitroso yeast. Unfortunately, nitrosoreas (e.g. Carmustin) is associated with considerable side effects, including bone marrow elevation, hepatotoxicity, nephrotoxicity, and interstitial lung disease. For this reason, they are primarily used to treat recurrent GB [5].
1.2 Concept of nanotechnology
A lot of medications have issues with solubility and instability, which can reduce their efficacy. Hydrophobic medications can be stabilized and made more soluble using nanoparticles, extending their shelf life.
By engineering nanoparticles to target particular cells or tissues, the therapeutic efficacy can be increased and off-target effects can be minimized. This is accomplished by adding ligands to the surface of nanoparticles that attach to particular target cell receptors
Nanoparticles can reduce the exposure of non-target tissues to medications by transporting them directly to the target region. This improves safety and minimizes negative effects.
1.3 BBB
The blood brain barrier (BBB) and the blood cerebrospinal fluid barrier (BCSFB) are two barrier systems that shield the brain from potentially dangerous chemicals. The BBB is made up of a complex network of endothelial cells, astroglia, pericytes, perivascular macrophages, and a basal lamina. Endothelium cells in the brain form "tight junctions" or zonula occludens, which are special structures seen in the central nervous system. In peripheral tissues, this is the closest cell-to-cell contact. The main obstacle remains the effective transfer of these substances over the blood-brain barrier, even with the substantial increase in CNS medication discovery. The main factor controlling the diffusion of drugs is the biologically active molecule's capacity to pass through lipid membranes (8).
1.4 Current GB Treatments And Its Challenges
The supply criteria for GB patients consist of a multimodal approach based on maximum safe surgical resection (to reduce tumor site diagnosis to maintain histological diagnosis and potential lifesuppression mass effects and tumor degradation) followed by radiation and chemotherapy [6].
Surgical resection is usually the first stage of treatment when GB patients have good performance status (in clinical settings, Karnowsky performance statuses of over 60% are generally considered cheap). Surgical resection of the tumor improves symptoms and neurological defects and reduces tumor edema associated with mass effects. Furthermore, surgery allows tumor rehearsals for histopathological and genetic characterization that affect the treatment and chemotherapy regime of selected beams [6]
After Roger Stuppp and colleagues' studies, adjuvant treatment for GB was standardized after maximum safe resection. In this study, 573 patients from 85 centers were randomized with radiation therapy or radiotherapy treatment and TMZ chemotherapy. This improved moderate survival rates for patients in the combined treatment group with minimal additional toxicity [7]. As a result of this study, GB patients will be treated after radiation therapy and surgical resection with TMZ.
Recently, tumor treatment facilities (TTFs) have been created as a therapeutic modality that selectively promotes antihyphal effects on GB cells using headsets that produce low-intensity, moderate frequency (200 Hz), causing replication cycle arrest and arrest. Roger Stupp and colleagues conducted a randomized clinical study involving 695 patients who underwent surgical resection or biopsy. Patients were randomized in two groups: TTF plus maintenance TMZ or TMZ alone. Progression - Free Survival (6.7 compared to 4.0 months) and Overall Survival (20.9 vs. 20.9 16.0 months) was superior in the TTF-TMZ group compared to TMZ [8].
INTRANASAL DRUG DELIVERY FOR BRAIN TARGETING
It has been observed that the olfactory and trigeminal nerves transport pharmacological drugs to the brain when they are administered to the nasal cavity. The amount of the chemotherapy agent that is absorbed by the nose-to-brain pathway depends on a number of factors, including the duration of contact with the nasal mucosa, the rate of mucus clearance, the drug's solubility and metabolic stability in mucus, and others. It is yet uncertain how exactly the nose-to-brain transmission occurs (9).
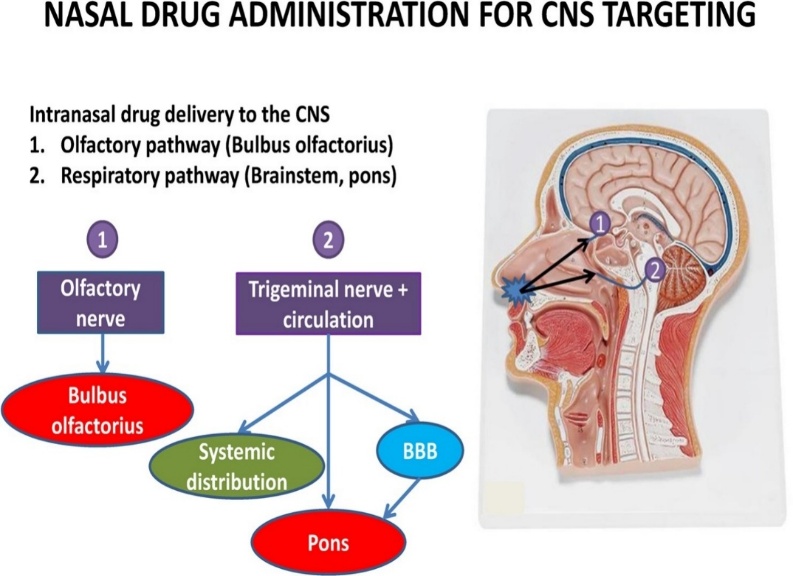
Fig 2: - Intra nasal (IN) administration
Nanocarriers can be modified for targeted drug delivery by using various ligands, aptamer conjugation for specific tumor targeting (10). A variety of nanocarriers are used in nanoparticle drug delivery systems to deliver drugs to the intended organs (11). Drug molecules are thought to enter the nasal cavity and go to the brain via two main routes: the neuronal pathway (major pathway) and the systemic circulation, which involves bridging the blood-brain barrier (minor pathway).
ANATOMY AND PHYSIOLOGY AND CELLULAR STRUCTURE OF THE HUMAN NASAL CAVITY
Defining the nasal cavity's function and cellular and anatomical makeup is essential for researching nasal drug absorption and the paths molecules must travel through before reaching the brain. The nose is in charge of several physiological processes, including breathing and smell. The septum, which runs along the midsagittal plane, separates its two symmetrical compartments. The palatine bone serves as a barrier between the nasal and oral cavities. Both nasal cavities have an approximate combined area of 150–160 cm, and they are coated with a layer of mucosa. Three zones can be distinguished inside these voids. The first is the vestibular area, which is situated just at the nose openings and is the most anterior. With a surface area of around 0.6 cm2, it has nasal hairs that filter particles that are inhaled. Squamous epithelial cells predominate in this region, with ciliated cells being scarce or non-existent. Drug absorption in this location is severely restricted because of the cellular structure and narrow surface area of the nasal cavity (12,13,14).
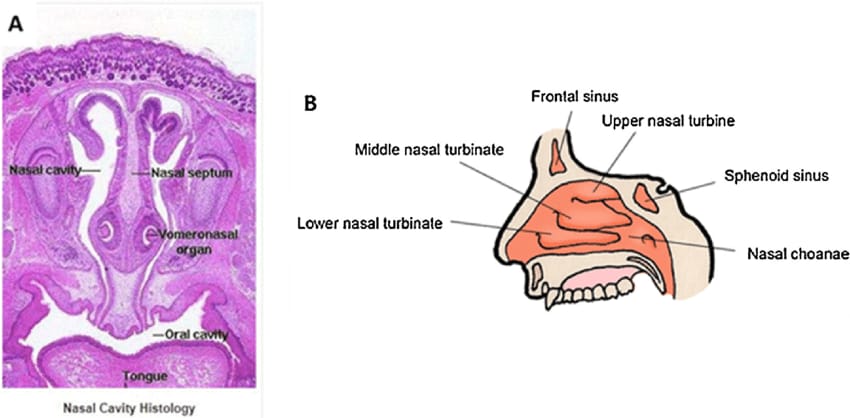
Fig 2: - Anatomy and physiology of the nasal cavity
Anatomy of the nasal cavity, Classified into three types
A. The vestibular region,
B. The respiratory region, and
C. The olfactory region.
A. Vestibular Region
The frontal area of the nasal cavity, known as the vestibular region, is rich in mucus and ciliated cells called hairs that use mucocilliary clearance to keep out foreign objects. The substantial section of the nasal cavity that follows is referred to as the respiratory area. With an approximate area of 130 cm2, it is the largest part of the nasal cavity.
B. Respiratory region
In apart from having many blood arteries, the respiratory region also has trigeminal sensory neurons. While trigeminal neurons are in charge of drug transport from the nasal cavity to the brain's pons and cerebrum, as well as, to a lesser extent, the olfactory and frontal brains, the blood vessels found in the respiratory region aid in drug absorption into the systemic circulation.
C. Olfactory region
The olfactory region is located beneath the cribriform plate of the ethmoid bone in the upper part of the nasal cavity, also known as the roof. It also comprises four main cell types: basal cells, microvillar cells, supporting cells, and olfactory receptor neurons, which make up the majority of the cells with a little fraction of trigeminal neurons. In addition to these, the lamina propria includes Bowman's gland, perivascular spaces, axons, connective tissues, lymphatic network, and blood vessels beneath the olfactory and respiratory epithelium (15).
Pathway for transport into brain via nasal route
Routes for nasal transfer into the brain The nasal cavity has a lot of potential for brain targeting because to its direct connection to the brain, free from interference from the blood-brain barrier and other external factors. Most drug transport happens through both a circulatory and neurological channel, including the olfactory and trigeminal nerves. Additionally, the lymphatic and CSF systems play a little part in the movement of drugs from the nose to the brain. The several brain transport mechanisms are then discussed.
A. Neuronal pathway
B. Olfactory nerve pathway
C. Trigeminal sensory nerve pathway
D. Vascular pathway
A. Olfactory and trigeminal nerve pathway
Drug transfer via intracellular and paracellular channels via olfactory neurons and supporting cells from the nasal cavity to the central nervous system Through its ophthalmic division (V1), maxillary division (V2), or mandibular division (V3), the trigeminal nerve transmits sensory data from the nasal cavity, oral cavity, eyelids, and cornea to the central nervous system. The dorsal nasal mucosa and the front part of the nose are innervated by branches of the trigeminal nerve's ophthalmic division, whilst the nasal mucosa's lateral walls are innervated by branches of the maxillary division. There are no direct neurological inputs to the nasal cavity from the trigeminal nerve's mandibular division, which reaches to the lower jaw and teeth (16).
NANOCARRIERS FOR NASAL DRUG DELIVERY
Drug delivery has seen an upsurge in interest in nano carrier systems due to their potential benefits, which include improving the solubility and, consequently, the bioavailability of active ingredients that are poorly soluble in water and fall under BCS classes II and IV. Recent research has started to concentrate on liposomes as a potential medication delivery system for AD treatment. For formulation scientists, the use of nanotechnology in drug delivery has created a number of potential for improved therapeutic agent administration to the central nervous system. Apart from improving brain support, these systems also offer other benefits including regulated or prolonged drug release and protection against degradation before the drug reaches the intended location, resulting in a lower dosage or frequency with fewer or no side effects. By using appropriate nano-formulations, many medication molecules have been made to pass through the blood-brain barrier, improving the medicine's therapeutic activity and efficacy (17).
POLYMERIC NANOPARTICLE
Polymers and co-polymers, which are big molecules made up of repeating subunits, make up a class of nanomaterial called polymeric nanoparticles (PNPs). These nanoparticles, which typically range in size from 1 to 1000 nanometers, have attracted a lot of interest from a range of industries due to their numerous applications and versatile properties. PNPs can increase the drug's bioavailability, prolong the half-life of its plasma circulation, and allow the pharmaceutical molecule to remain in the targeted tissue for a longer amount of time. However, the creation of intranasally administrable PNPs for brain-targeted administration is dependent on the polymers' nontoxic, biocompatible, and biodegradable properties; the breakdown products of the polymers must likewise be non-toxic and readily excreted from the body (18).
Components:
a. Phospholipid
Phospholipids are amphipathic molecule i.e., having affinity for both aqueous & non-polar moieties, as they have a hydrophobic tail & hydrophilic head. The tail portion consist of 2 fatty acid chains having 10-24 carbon atoms & 0-6 double bonds in each chain. The head or polar portion consist of phosphoric acid bound to a water-soluble molecule.
b. Polymer
A range of polymers are used to create polymeric nanoparticles (PNPs), which are selected for their biocompatibility, biodegradability, and suitability for certain uses such tissue engineering, medication administration, and diagnostics. Several typical polymers used to create nanoparticles are categorized as:
Natural polymers: Chitosan, alginate, gelatine.
Synthetic polymers: poly (lactic co-glycolic acid) (PLGA), poly (lactic acid) (PLA), polycaprolactone (PCL).
Semi-synthetic polymers: cellulose acetate.
c. Surfactant
Solid lipid colloidal systems are produced in large part by surfactants. By attaining colloidal stability during the nanoparticle creation process, they simplify the growth of nanoparticles and reduce the interfacial tension between the hydrophilic and lipophilic phases of the colloidal dispersion. A hydrophilic (ethylene oxide) and lipophilic (hydrocarbon chain) moiety combine to generate the head and tail of surfactants, which are amphipathic in nature. Most people believe that ionic and non-ionic surfactants provide electrostatic stability and steric repulsion stability, respectively. To assume true steric stability, tiny amounts of non-ionic surfactants are used.
d. Liposomes
Liposomes are closed bilayered structures, formed by phosphates with phosphate heads and hydrophobic lipid tails, which are capable of transporting unqualified drugs regardless of their physical and chemical properties. The drug can be placed on the hydrophobic lipid tail or on the hydrophilic polar head [26, 28]. According to the number of phospholipid bilayers, liposomes are classified as monolayers or multilayered vesicles [26]. The monolayer vesicles are further divided based on the size of small monolayer vesicles (<100 nm), large monolayer vesicles (100 nm–1 µm), and giant monolayer vesicles (>1 µm) [28]. Liposomes can be administered hydrophobic and hydrophobic agents as cancer treatments, immunomodulatory active ingredients, and even genetic therapy [28].
e. Solid Lipid Nanoparticles
Fixed lipid lipids (SLNs) are composed of lipids that remain in the solid state at physiological temperature [26]. These particles have a lipid (hydrophobic) compact core coated with phospholipids, which can improve the efficiency of taking hydrophobic drugs [26]. The mechanisms that allow SLNs to enter the central nervous system are positive discussion [33]. Paraspherebased invasion of nanoparticles through the temporary opening of narrow connections between endothelial cells in the BBB was previously supported as the main pathway for brain nanoparticle availability [33,34,35], but recent studies have shown common NP NP endocytosis [33,36].
f. Nanogels
This class of nanoparticles consists of networked hydrophilic polymer networks, indicating the promise of recent growth [28]. Nanogels have numerous hydrophilic groups that contribute to NP swelling, expanding the internal grid and releasing confined drugs by passive diffusion [28,40]. Nanogels can be finely tuned in terms of size (50500 nm) and conformation according to the physicochemical properties of microworld factors. Temperature, pH values, ion changes, redox states, and light are used as stimuli for drug release [28, 41]. The GB microenvironment is usually acidic because it is usually the war effect of tumor cell death and Warburg's war effect (aerobic glycolism metabolism identification characteristic of cancer cells) [42]. Song P. et al. pH/talksensitive carboxymethyl chitosan nanogels (CMCSNs) were prepared. It is modified by targeting the peptide-agiopep2 (ANG) and is carried with doxorubicin (dox@ang@cmcsn). Addition of ANG for nanoform simulation resulted in BBB penetration and tumor penetration in both in vitro and in vivo models. Mice containing C6 tumors treated with DOX@CMCSN-NanoFormulation showed a twofold increase in cell recording and antitumor activity [43].
POLYMERIC-BASED DRUG CARRIERS
Polymeric nanoparticles (polymer-drug conjugates)
Naturally occurring polymers like albumin, chitosan, and heparin have long been the preferred medium for delivering medications, proteins, DNA, and oligonucleotides (19). Due to their ability to both encapsulate pharmaceuticals, protecting them from excretion and metabolism, and carry active agents across the blood-brain barrier without causing any harm to the brain, polymeric nanoparticles have been demonstrated to be promising carriers for CNS drug delivery (20). A variety of polymers and approaches have been employed; most recently, the use of ligands to improve the specificity of medications administered to the central nervous system has been contemplated. Disseminated and extremely aggressive brain cancers have been proven to respond well to NP therapy. In rats with intracranially transplanted glioblastomas, doxorubicin-loaded polysorbate 80-coated NPs administered intravenously were able to decrease mass tumors (21). The idea offers a better medication targeting method for delivering a pharmacologically active material to a mammal's central nervous system across the blood-brain barrier. A pharmacologically active material was added to NPs based on poly (DL-lactide) (PLA) and/or poly lactide-co-glycolide) (PLGA) in order to accomplish this goal (22). Invented a medication delivery system that resembles the size, capsid-like protein capsule, cell-specific entry, release of toxins, killing of infected cells, and migration to nearby cells of viruses. This vehicle, known as a virogel, is made up of a ligand, a hydrophilic outer shell, a hydrophobic polymeric core, and a hydrophilic inner shell. Poly(L-histidine-co-phenylalanine) is the core of an examssple drug-loaded virogel, which also contains doxorubicin, PEG as the inner shell, bovine serum albumin as the outer shell, and folic acid as the ligand (23).
REFERENCES


Disha Patil, Vishwadeep Dhurandhar, Vrushali Gangurde, Dr. Khandareo Jadhav, Nanoparticulate Systems for Treatment of Glioblastoma by Intranasal Administration: A Non-Invasive Approach, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 1384-1398. https://doi.org/10.5281/zenodo.15613746
 10.5281/zenodo.15613746
10.5281/zenodo.15613746
