1Department of Pharmaceutical Chemistry, University college of technology Osmania University, Hyderabad, 500007, Telangana, India.
2Department of Pharmacology, Vaagdevi College of Pharmacy (Affiliated Kaktiya University), Ramnagar, kishanapura, Hanamkonda, 506001, Telangana, India.
3Department of pharmaceutical chemistry, Matoshri College of Pharmacy, Eklahare, Nashik, 422105, Maharashtra, India.
Tuberculosis (TB) continues to be a pressing global health concern, particularly in low- and middle-income countries where healthcare infrastructure and resources are limited. The situation is further exacerbated by the rise of multidrug-resistant TB (MDR-TB) and rifampicin-resistant TB (RR-TB), which undermine global TB control efforts. MDR-TB is defined by resistance to at least isoniazid and rifampicin, the two cornerstone first-line anti-TB medications, while RR-TB refers specifically to resistance against rifampicin, with or without concurrent resistance to other drugs. These drug-resistant strains are more difficult to diagnose and treat, often requiring longer, costlier, and more toxic regimens that may result in poor patient adherence and treatment failure. This review provides a comprehensive analysis of MDR/RR-TB, addressing key issues such as the underlying biological mechanisms of drug resistance, current trends in global and regional epidemiology, and risk factors contributing to the emergence and spread of resistant strains. Significant attention is given to the evolving diagnostic landscape, particularly the development and implementation of rapid molecular tests such as Xpert MTB/RIF and line probe assays, which have significantly improved the timeliness and accuracy of diagnosis. Furthermore, the paper explores the latest World Health Organization (WHO) recommendations for treatment, including standardized shorter all-oral regimens and individualized long-term therapies incorporating newer drugs like bedaquiline, delamanid, and pretomanid. The challenges of treatment, including drug toxicity, high costs, and poor adherence, are discussed alongside the importance of psychosocial support and community-based interventions. Additionally, the review highlights emerging solutions, such as host-directed therapies, novel diagnostics utilizing artificial intelligence, digital health technologies, and promising vaccine candidates like M72/AS01E. It emphasizes the importance of a multi-pronged approach involving medical innovation, patient-centered care, and international collaboration to effectively manage and eventually eliminate MDR/RR-TB as a global public health threat.
Tuberculosis (TB), caused by Mycobacterium tuberculosis, continues to be a major cause of illness and death worldwide, particularly in low- and middle-income countries. Despite long-standing global efforts to control TB, the disease remains among the top ten causes of mortality and ranks as the leading cause of death from a single infectious agent, surpassing HIV/AIDS [1]. One of the most concerning developments in recent decades has been the rise of drug-resistant forms of TB, especially multidrug-resistant TB (MDR-TB) and rifampicin-resistant TB (RR-TB), which pose substantial challenges to TB control programs globally. MDR-TB is characterized by resistance to at least isoniazid and rifampicin, the two most effective first-line anti-TB drugs [1]. RR-TB refers specifically to resistance against rifampicin, with or without resistance to other first-line drugs [1]. These forms of TB are more difficult and expensive to treat, often requiring prolonged therapy with second-line drugs that are associated with increased toxicity and reduced effectiveness [13,16]. In 2022, an estimated 410,000 people developed MDR/RR-TB globally, and approximately 160,000 deaths were attributed to these drug-resistant strains [1]. Countries with the highest burdens include India, China, and Russia, although MDR/RR-TB is a growing concern worldwide [6]. The development of drug resistance can occur through the transmission of resistant strains (primary resistance) or through improper treatment and non-adherence to therapy (acquired resistance) [5]. Multiple risk factors contribute to the emergence and spread of MDR/RR-TB, including previous TB treatment, HIV co-infection, malnutrition, poverty, and inadequate access to healthcare services [7]. Socioeconomic conditions and limited healthcare infrastructure often lead to delayed diagnosis and treatment interruptions, further exacerbating resistance development [12]. In addition, stigma and mental health issues play a role in reducing treatment adherence, particularly in marginalized communities [7]. In response to this global crisis, the World Health Organization (WHO) has implemented updated guidelines to improve diagnosis, treatment, and surveillance of drug-resistant TB. Recent advances in diagnostic tools, such as the Xpert MTB/RIF assay and line probe assays, have enabled more rapid detection of both TB and rifampicin resistance, allowing for earlier initiation of appropriate therapy [9,10]. Moreover, new therapeutic options, including bedaquiline, delamanid, and pretomanid, have improved outcomes for many patients and are central to shorter, all-oral treatment regimens now recommended by WHO [14,15]. However, challenges remain, especially in resource-limited settings where access to rapid diagnostics and newer drugs is restricted, and where health systems are overburdened [12,13]. The COVID-19 pandemic has further disrupted TB programs, leading to reduced case detection and treatment delays [12]. To combat MDR/RR-TB effectively, a multifaceted approach is required—one that combines innovations in diagnostics and therapeutics with strong public health policies, global collaboration, and support for affected individuals and communities. This review explores the complex landscape of MDR/RR-TB by examining the pathophysiology of drug resistance, current epidemiological trends, advancements in diagnostics and treatment, and emerging strategies for disease control. Through a synthesis of recent research and WHO guidelines, this paper aims to highlight both the persistent challenges and the promising developments in managing drug-resistant TB.
Pathophysiology And Mechanisms of Drug Resistanc:
Biology of Mycobacterium Tuberculosis:
Mycobacterium tuberculosis (M. tuberculosis), the causative agent of TB, is a slow-growing, acid-fast, aerobic bacillus with a uniquely complex cell wall rich in mycolic acids. This lipid-rich structure confers resistance to many conventional antibiotics and disinfectants and allows the organism to evade immune responses by surviving within macrophages [2]. The bacteria replicate slowly, with a generation time of 15–20 hours, contributing to the chronic nature of TB and complicating treatment strategies [2]. The pathogen primarily infects the lungs but can also disseminate to other organs through hematogenous spread. Inside the host, M. tuberculosis persists within granulomas—a structured immune response where macrophages, lymphocytes, and other immune cells attempt to contain the infection. However, the bacteria can remain dormant for years in a latent state and reactivate when host immunity is compromised [2].
Mechanisms of Drug Resistance:
Drug resistance in M. tuberculosis arises through spontaneous chromosomal mutations rather than plasmid-mediated gene transfer, as seen in many other bacteria [3]. The most common mechanism of rifampicin resistance involves mutations in the rpoB gene, which encodes the β-subunit of RNA polymerase. These mutations alter the drug-binding site, thereby reducing the affinity of rifampicin for its target and rendering it ineffective [3]. Isoniazid resistance typically results from mutations in the katG gene, which encodes catalase-peroxidase needed for isoniazid activation. Loss of function in katG prevents the drug from converting into its active form [4]. Additionally, mutations in the inhA promoter region can lead to the overexpression of enoyl-acyl carrier protein reductase, the target of activated isoniazid, resulting in resistance [4]. These mechanisms compromise the efficacy of the cornerstone drugs in TB therapy (Figure No. 1).
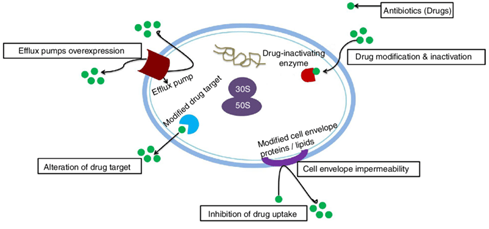
Figure No. 1: Mechanisms of Drug Resistance in M. tuberculosis
Transmission Vs. Acquired Resistanc:
Resistance to anti-TB drugs can be either primary or acquired. Primary resistance occurs when individuals are infected with drug-resistant strains directly from other people. In contrast, acquired resistance develops during the course of TB treatment, usually as a result of improper therapy, inadequate drug regimens, poor patient adherence, or substandard drug quality [5]. In many high-burden settings, both types of resistance coexist and contribute to the growing challenge of MDR/RR-TB. Notably, the acquisition of resistance does not significantly reduce the fitness of M. tuberculosis, meaning resistant strains can spread efficiently, just like drug-susceptible ones [5]. These characteristic underscores the importance of early detection and effective treatment to prevent further transmission.
EPIDEMIOLOGY:
Global and Regional Prevalence:
TB remains a pressing global health threat, with MDR and RR forms complicating control efforts. According to the WHO, an estimated 410,000 individuals developed MDR/RR-TB in 2022, and 160,000 deaths were attributed to these forms of the disease [1]. India, China, and the Russian Federation continue to bear the highest burden, collectively accounting for a significant proportion of global cases [6]. MDR/RR-TB is found in virtually every country, but its prevalence varies depending on regional healthcare infrastructure, TB control programs, and socioeconomic conditions. In certain settings with high HIV prevalence or weak TB programs, the proportion of MDR/RR-TB among new TB cases can exceed global averages [6].
Risk Factors:
A range of biological and socioeconomic risk factors contribute to the development and spread of MDR/RR-TB. The most significant risk factor is a history of previous TB treatment, especially if the regimen was inadequate or if the patient did not complete therapy [7]. HIV co-infection also significantly increases the risk of TB progression and complicates treatment due to immune suppression [7]. Other contributing factors include malnutrition, diabetes, smoking, alcohol use, incarceration, and exposure to polluted environments [7]. Socioeconomic determinants—such as poverty, overcrowding, and limited access to healthcare services—further exacerbate the problem, particularly in low-income countries [7].
Trends in Resistance Development:
Although the total number of TB cases has been increasing due to improved case detection, the relative proportion of MDR/RR-TB among new TB cases has shown a slight decline—from 4.0% in 2015 to 3.3% in 2022 [1]. This suggests that efforts to prevent the emergence of drug resistance are having some impact. However, among previously treated cases, the prevalence of MDR/RR-TB remains considerably higher, reflecting persistent challenges in managing TB recurrences and treatment failures [1]. The emergence of resistance to second-line drugs in some regions is a growing concern, potentially leading to extensively drug-resistant TB (XDR-TB), which is even more difficult to treat and control [1,16]. Continued surveillance, investment in diagnostic infrastructure, and adherence to WHO-recommended treatment protocols are critical to halting the spread of resistant TB strains [1].
Diagnosis of MDR/RR-TB:
Accurate and timely diagnosis of multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) is essential for initiating appropriate treatment, preventing further transmission, and improving patient outcomes. Traditional diagnostic approaches have long relied on culture and phenotypic drug susceptibility testing (DST), but these methods are slow and often unavailable in low-resource settings. Recent advances in molecular diagnostics have significantly enhanced the speed and accuracy of detection, especially for rifampicin resistance, which serves as a reliable proxy for MDR-TB in many contexts [8,9].
Traditional Methods:
Culture-based methods remain the gold standard for diagnosing TB and determining drug susceptibility. These include solid media such as Lowenstein–Jensen (LJ) and liquid culture systems like the Mycobacteria Growth Indicator Tube (MGIT) system. However, these techniques are time-consuming; growth can take 4–8 weeks, and DST results may require additional weeks. Moreover, culture facilities demand stringent biosafety standards and skilled laboratory personnel, which are often lacking in high-burden countries [8]. Despite these limitations, culture and phenotypic DST are still necessary for confirming resistance to second-line drugs and for detecting resistance patterns that may not be identified by molecular assays [8].
Molecular Techniques:
Molecular diagnostics have revolutionized TB detection and the identification of drug-resistant strains. These techniques are faster, more accessible, and can be deployed closer to the point of care. The most widely used molecular tool is the Xpert MTB/RIF assay, a real-time PCR-based test that detects Mycobacterium tuberculosis complex DNA and mutations in the rpoB gene responsible for rifampicin resistance [9]. This assay delivers results within two hours and can be used directly on sputum samples, offering a rapid and reliable alternative to traditional culture methods. The Line Probe Assay (LPA), such as the Genotype MTBDRplus and MTBDRsl, identifies resistance-conferring mutations in both first-line (isoniazid and rifampicin) and second-line drugs (fluoroquinolones and injectable agents). LPAs are endorsed by the WHO for their high sensitivity and specificity and play a crucial role in guiding individualized therapy [10]. More recently, Whole Genome Sequencing (WGS) has emerged as a powerful tool for comprehensive resistance profiling. WGS can detect known and novel resistance mutations across the genome, providing a detailed map of drug susceptibility. However, it remains costly and requires high-level laboratory infrastructure, making it less feasible in many TB-endemic regions [11].
Emerging Diagnostic Approaches:
Novel diagnostic technologies are under development to overcome current limitations. Techniques like Raman spectroscopy, when integrated with machine learning algorithms, show promise in rapidly distinguishing TB bacteria based on their molecular signatures [10]. These non-culture-based methods may allow for faster and more accessible testing in the future. Additionally, loop-mediated isothermal amplification (LAMP) and CRISPR-based diagnostics are being explored for their simplicity, speed, and potential for point-of-care use, particularly in rural settings where conventional PCR equipment may not be available [11].
Challenges in Diagnosis:
Despite these technological advances, significant diagnostic challenges persist. Many high-burden countries still lack access to molecular testing due to financial and infrastructural barriers. Limited availability of diagnostic equipment, shortages of trained personnel, and supply chain issues hinder widespread implementation [12]. Moreover, patients in rural or remote areas often face long travel distances to reach facilities equipped for molecular testing, causing delays in diagnosis and treatment initiation [12]. Another concern is the variable sensitivity of molecular assays in detecting isoniazid resistance. While rifampicin resistance serves as a proxy for MDR-TB, not all cases of isoniazid resistance are identified unless specific tests are performed, potentially leading to incomplete treatment regimens [9]. Furthermore, diagnostic strategies must evolve to keep pace with emerging resistance patterns, including pre-extensively drug-resistant TB (pre-XDR-TB) and extensively drug-resistant TB (XDR-TB). This necessitates continued investment in research, infrastructure, and global partnerships to expand access to reliable, rapid diagnostics in all affected populations [1,12].
Treatment and Management Strategies:
Effective treatment of multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) is complex, resource-intensive, and requires prolonged use of second-line anti-TB drugs. These regimens are often associated with higher toxicity, longer duration, and increased costs compared to drug-susceptible TB therapy. The World Health Organization (WHO) has updated its treatment guidelines multiple times in response to growing evidence, availability of new drugs, and real-world challenges in MDR/RR-TB control [13–16].
First-Line vs. Second-Line Drugs:
Standard treatment for drug-susceptible TB includes four first-line medications: isoniazid, rifampicin, pyrazinamide, and ethambutol. However, MDR-TB—defined by resistance to at least isoniazid and rifampicin—necessitates the use of second-line drugs, which include fluoroquinolones (e.g., levofloxacin, moxifloxacin), injectable agents (e.g., amikacin, capreomycin), and newer oral agents such as bedaquiline and linezolid [13]. These drugs are generally less effective, more toxic, and require a longer duration of administration than first-line agents.
WHO-Recommended Regimens:
The WHO now endorses all-oral, shorter treatment regimens for eligible MDR/RR-TB patients to minimize toxicity and improve adherence. The 6-month BPaLM regimen—consisting of bedaquiline, pretomanid, linezolid, and moxifloxacin—has demonstrated promising efficacy and safety, especially in patients without fluoroquinolone resistance [14]. For patients who are ineligible for the BPaLM regimen, the 9-month all-oral regimen is an alternative. This regimen typically includes bedaquiline, high-dose isoniazid, levofloxacin or moxifloxacin, clofazimine, ethambutol, pyrazinamide, and either linezolid or ethionamide, depending on drug susceptibility patterns and patient tolerance [15]. For individuals with extensive drug resistance or intolerance to shorter regimens, longer individualized treatment regimens lasting 18–20 months are used. These regimens are designed based on detailed drug susceptibility testing (DST) and often incorporate newer drugs such as delamanid and pretomanid in combination with conventional second-line agents [16].
Newer and Repurposed Drugs:
The introduction of bedaquiline, the first novel anti-TB drug in over four decades, has significantly improved treatment outcomes in MDR/RR-TB. Bedaquiline inhibits the bacterial ATP synthase enzyme, thereby halting energy production in Mycobacterium tuberculosis [17]. When used appropriately, it shortens treatment duration and reduces mortality rates. Delamanid, another recent addition, inhibits mycolic acid synthesis—essential for maintaining the mycobacterial cell wall. It is particularly useful in patients who cannot tolerate injectable drugs or are resistant to multiple drugs [18]. Pretomanid, a nitroimidazole agent, works synergistically with bedaquiline and linezolid, especially in the BPaL regimen. These drugs offer a more effective and better-tolerated treatment for MDR/RR-TB, especially when used in novel combinations [14,18]. Linezolid, although initially developed as an antibacterial for gram-positive infections, has shown potent anti-TB activity. However, its use is often limited by dose-related toxicities, including bone marrow suppression and peripheral neuropathy [14,19].
Side Effects and Adherence Issues:
Adverse effects associated with second-line drugs pose a significant barrier to treatment success. Common toxicities include hepatotoxicity (from pyrazinamide, high-dose isoniazid), nephrotoxicity and ototoxicity (from injectable agents like amikacin), and neurotoxicity (from linezolid and cycloserine) [13,19]. Managing these side effects requires regular clinical and laboratory monitoring. The involvement of trained health personnel, psychosocial counselling, and nutritional support is critical to helping patients adhere to lengthy and demanding regimens. Patient-centred care approaches, including directly observed therapy (DOT), community-based treatment support, and mobile health tools, are essential in improving adherence and treatment completion [19].
Role of Surgery:
Although medical management remains the cornerstone of MDR/RR-TB treatment, surgical resection of infected lung segments may be considered in patients with localized, non-responsive disease. This approach is typically reserved for cases with significant cavitary lesions or extensive drug resistance where pharmaceutical therapy alone is insufficient [20]. Surgical intervention, when coupled with effective medical therapy, can enhance treatment outcomes and reduce bacterial load.
Challenges In Controlling MDR/RR-TB:
The control of multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) remains one of the most complex public health challenges of the 21st century. Despite innovations in diagnostics and therapeutics, MDR/RR-TB continues to spread, particularly in resource-limited settings. The convergence of biological complexity, socioeconomic disparities, systemic health infrastructure issues, and global disruptions like COVID-19 has made the containment of MDR/RR-TB particularly difficult. A thorough understanding of the multifaceted barriers to control is necessary to improve patient outcomes and reduce transmission rates [1,12].
Delayed and Inaccurate Diagnosis:
One of the foremost challenges in controlling MDR/RR-TB is the delay in diagnosis or complete failure to detect drug resistance, which facilitates ongoing transmission and worsens clinical outcomes. In many high-burden countries, diagnostic facilities are concentrated in urban areas, making access difficult for rural populations [12]. Although Xpert MTB/RIF and line probe assays (LPA) have dramatically reduced time to diagnosis, their implementation remains limited due to high costs, equipment requirements, and the need for trained technicians [9,10,12]. In particular, whole-genome sequencing (WGS), while capable of detecting resistance to both first- and second-line drugs with high accuracy, is still largely confined to research or reference laboratories due to its complexity and cost [11]. Additionally, conventional culture-based drug susceptibility testing (DST) takes several weeks to yield results, further delaying the initiation of effective therapy [8].
High Cost and Toxicity of Second-Line Treatments:
Another significant barrier is the cost and toxicity of second-line treatment regimens. While first-line treatment for drug-susceptible TB is relatively inexpensive and well-tolerated, MDR/RR-TB regimens are expensive and require prolonged administration, often extending to 9–20 months depending on the resistance pattern and drug availability [13]. Drugs like linezolid, bedaquiline, clofazimine, and delamanid have improved outcomes, but their side effects are substantial and include hematologic toxicity, QT prolongation, hepatotoxicity, and neuropathy [14,17,18]. Moreover, access to these newer drugs is uneven globally, and in many countries, outdated regimens containing injectable agents like kanamycin or amikacin are still in use, despite their well-documented risks such as irreversible hearing loss [13,19].
Patient Adherence and Treatment Completion:
The complexity of treatment regimens and the length of therapy present another formidable obstacle. Patients are often required to take multiple pills daily for 9 to 20 months, which is psychologically and physically exhausting. Adverse effects often cause patients to interrupt or discontinue treatment, leading to suboptimal outcomes and the emergence of extensively drug-resistant TB (XDR-TB) [19]. Socioeconomic challenges such as loss of income, travel costs to health centres, and lack of family support further diminish adherence [7,13]. Strategies like directly observed treatment (DOT), digital adherence technologies (DAT), psychosocial counselling, and nutritional support have been shown to enhance adherence, but are inconsistently implemented due to funding limitations [19].
Social Stigma and Mental Health Burden:
MDR/RR-TB patients often suffer from social stigma, which leads to delayed diagnosis, concealment of symptoms, and poor health-seeking behaviour. This stigma is more pronounced in communities where TB is associated with poverty, HIV, and substance abuse, contributing to social isolation and discrimination [7]. Many patients experience anxiety, depression, and psychological trauma during treatment due to side effects, prolonged hospitalization, and fear of transmitting the disease to loved ones [19]. Mental health support remains largely neglected in national TB programs, despite evidence linking psychological care to better treatment adherence and outcomes.
Weak Health Systems and Infrastructure Gaps:
In many high-burden countries, the healthcare system is ill-equipped to manage MDR/RR-TB effectively. Challenges include shortages of trained personnel, limited diagnostic infrastructure, drug stock-outs, and weak supply chain management systems [1,12]. Surveillance systems are often inadequate for tracking drug resistance trends or monitoring treatment outcomes, which hampers timely interventions. Moreover, in many settings, TB services are not integrated with primary healthcare, leading to missed opportunities for early diagnosis and treatment initiation [1]. International funding and technical assistance, such as that provided by the Global Fund and the Stop TB Partnership, remain essential to strengthening national TB control programs.
Disruption Due to COVID-19 Pandemic:
The COVID-19 pandemic severely disrupted TB control efforts worldwide. Resources including health workers, diagnostic tools, and hospital beds were diverted toward COVID-19 response, leaving TB services under-resourced and inaccessible [12]. According to WHO, there was a substantial drop in TB case notifications during 2020–2021, and many patients experienced interrupted treatments, raising concerns about a surge in drug-resistant TB cases in the post-pandemic period [1]. The pandemic also highlighted the fragility of health systems and the need for resilient TB programs capable of withstanding public health emergencies.
Drug Supply and Global Inequity:
There are significant global disparities in access to new and repurposed TB drugs such as bedaquiline, pretomanid, and delamanid [14,17,18]. Regulatory approval, high drug prices, and intellectual property issues limit widespread access in low- and middle-income countries, which bear the highest burden of MDR/RR-TB. Even when these drugs are available, many countries lack guidelines or infrastructure to implement recommended regimens such as the BPaLM 6-month regimen [14]. Moreover, long procurement timelines and inconsistent supply chains lead to treatment delays and interruption, further contributing to poor outcomes.
Poor Contact Tracing and Community Engagement:
Contact tracing and active case finding are essential components of TB control, yet these strategies are underutilized in many endemic countries due to limited personnel, funding, and logistical support [1,12]. Community health workers are often not adequately trained or supported, and cultural barriers may prevent households from cooperating with public health efforts. Furthermore, lack of community education about MDR/RR-TB reduces the effectiveness of awareness campaigns and leads to persistent transmission in high-risk groups.
Lack of Integration with HIV and Other Comorbidities:
HIV co-infection increases the risk of developing active TB and complicates the management of MDR/RR-TB [7]. However, TB and HIV services are still siloed in many health systems, resulting in missed opportunities for co-management and comprehensive care. Additionally, other comorbidities such as diabetes and malnutrition are often neglected in TB care, despite their known impact on treatment success and relapse rates [7].
Advances and Future Directions:
The battle against multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) is entering a new era marked by scientific innovations, advanced diagnostics, novel therapeutics, and enhanced public health strategies. Despite formidable challenges, recent years have witnessed a shift in global efforts to strengthen the detection, treatment, and prevention of drug-resistant TB. These advances offer promising avenues to reduce disease burden, improve patient outcomes, and move toward the World Health Organization's (WHO) End TB Strategy goals [1,14].
Advances in Diagnostic Technologies:
Rapid and accurate diagnosis is critical for effective management and control of MDR/RR-TB. Recent diagnostic breakthroughs have transformed TB detection. The Xpert MTB/RIF assay has allowed for the simultaneous detection of TB and rifampicin resistance within two hours, significantly reducing the diagnostic delay [9]. Line probe assays (LPAs) further enhance diagnostic accuracy by identifying genetic mutations associated with both first- and second-line drug resistance [10]. Moreover, whole-genome sequencing (WGS) is now being utilized in reference laboratories to provide a comprehensive resistance profile, enabling individualized treatment regimens [11]. However, its use is still limited by cost and technical requirements. Newer techniques such as Raman spectroscopy combined with machine learning algorithms are under development, offering rapid and non-invasive detection of TB and drug resistance markers, which may eventually be deployed in point-of-care settings [10].
Development of Novel Therapeutics and Shorter Regimens:
The treatment landscape for MDR/RR-TB has improved markedly with the development of shorter and more effective regimens. The WHO now recommends a 6-month all-oral BPaLM regimen (bedaquiline, pretomanid, linezolid, and moxifloxacin) for patients with confirmed MDR/RR-TB who meet specific criteria [14]. This regimen not only shortens treatment duration but also avoids the use of toxic injectable drugs. Other regimens, such as the 9-month modified shorter regimen incorporating bedaquiline, levofloxacin or moxifloxacin, clofazimine, pyrazinamide, ethambutol, high-dose isoniazid, and linezolid or ethionamide, offer alternatives for patients with limited drug resistance [15]. These regimens have demonstrated improved adherence and better treatment outcomes due to reduced duration and pill burden [14,15]. In addition, bedaquiline (targets ATP synthase) and delamanid (inhibits mycolic acid synthesis) have become cornerstones of MDR/RR-TB treatment due to their potent sterilizing activity and favorable safety profiles when used correctly [17,18]. Pretomanid, a nitroimidazole, works synergistically with other agents and is now part of WHO-recommended regimens [14]. Ongoing clinical trials continue to investigate combinations of new and existing drugs to further reduce treatment time, toxicity, and resistance emergence [18].
Host-Directed Therapies (HDTs):
A promising area of research is the development of host-directed therapies (HDTs) aimed at modulating the immune response to improve treatment efficacy and reduce tissue damage. Unlike traditional antimicrobial therapies that target the bacterium directly, HDTs focus on enhancing the host’s innate and adaptive immunity, potentially accelerating bacterial clearance and minimizing side effects [18]. Agents under investigation include non-steroidal anti-inflammatory drugs (NSAIDs), statins, and immunomodulators such as interleukin inhibitors. HDTs may also help in managing inflammatory lung damage caused by TB, which can persist even after microbiological cure, improving long-term pulmonary outcomes and quality of life [18].
Advances in TB Vaccine Development:
Vaccines remain a crucial element in TB prevention. The BCG vaccine, though widely used, offers limited protection against pulmonary TB in adults. Recent advancements in vaccine research have led to the development of promising candidates such as M72/AS01E, which demonstrated about 50% efficacy in preventing active pulmonary TB in latently infected individuals during Phase IIb trials [20]. Other vaccine strategies, including recombinant protein subunits, viral vectors, and live attenuated mycobacterial strains, are currently under various stages of clinical evaluation. If successful, these vaccines could significantly reduce the incidence of TB and curb the transmission of drug-resistant strains, especially in high-burden countries [20].
Integration of Digital Health Tools and Artificial Intelligence (AI):
Digital innovations are transforming TB care delivery. Mobile health (mHealth) tools, such as smartphone-based applications and digital pillboxes, enable remote monitoring of treatment adherence and improve communication between patients and healthcare providers [19]. AI-driven algorithms are increasingly used in radiographic interpretation, enabling rapid and accurate TB screening in settings where radiologists are unavailable. In addition, electronic health records and data analytics platforms are being utilized to track patient progress, monitor drug resistance trends, and guide policy decisions. These technologies, when effectively implemented, can improve program efficiency, optimize resource allocation, and personalize care [19].
Strengthened Global Policies and Initiatives:
Global initiatives continue to play a pivotal role in combating MDR/RR-TB. The WHO End TB Strategy aims to reduce TB incidence by 90% and deaths by 95% by 2035, focusing on early diagnosis, universal drug susceptibility testing, shorter and effective treatment regimens, and social protection for patients [1]. Other global partnerships, such as the Stop TB Partnership, advocate for increased funding, innovation, and equitable access to diagnostics and treatments. The integration of TB services into universal health coverage (UHC) frameworks is also being prioritized, ensuring that all individuals, regardless of socioeconomic status, receive timely and quality TB care [1]. International funding mechanisms like the Global Fund to Fight AIDS, Tuberculosis and Malaria remain instrumental in supporting programmatic expansion in low-income countries.
CONCLUSION:
Multidrug-resistant and rifampicin-resistant tuberculosis (MDR/RR-TB) continues to pose a serious global health threat, particularly in low- and middle-income countries where healthcare infrastructure is often inadequate. Despite extensive public health efforts, the rising incidence of drug-resistant TB strains reflects critical gaps in the timely diagnosis, effective treatment, and management of the disease [1,6]. Delays in diagnosis, patient non-adherence, toxicity of treatment regimens, stigma, and socio-economic barriers further compound the problem [7,12,13]. However, the past decade has seen notable advancements in the fight against MDR/RR-TB. Molecular diagnostic techniques, such as Xpert MTB/RIF and Line Probe Assays, have significantly shortened the time to diagnosis and facilitated early initiation of appropriate therapy [9,10]. Whole-genome sequencing and other advanced tools like Raman spectroscopy are paving the way for more precise and comprehensive resistance profiling [10,11]. On the treatment front, the introduction of shorter, all-oral regimens such as the 6-month BPaLM regimen and newer drugs like bedaquiline, delamanid, and pretomanid represent significant progress in reducing treatment duration, improving tolerability, and enhancing adherence [14,17,18]. Novel strategies like host-directed therapies and digital health interventions hold promise for further improving outcomes and personalizing care [18,19]. In addition, the development of TB vaccines such as M72/AS01E and the growing application of AI in TB diagnostics and management underscore a future of integrated, technology-driven healthcare [19,20]. These advancements, coupled with global initiatives like the WHO End TB Strategy and expanded public-private partnerships, can accelerate progress toward TB elimination if adequately supported [1]. Nonetheless, challenges remain. Ensuring equitable access to new tools and medications, addressing the social determinants of health, and strengthening health systems are essential components of a comprehensive MDR/RR-TB response. Sustained political commitment, increased funding, robust surveillance systems, and community engagement are necessary to translate scientific innovations into real-world impact. In conclusion, while MDR/RR-TB remains a formidable challenge, recent scientific and policy advances provide a foundation for optimism. Continued global collaboration, research, and implementation of evidence-based strategies will be pivotal in ending the TB epidemic and achieving the ambitious targets set by the international community [1,14,19].
REFERENCES



Soniya Dommati*, Poojitha Gottimukkula, Ragini Patil, Multidrug-Resistant and Rifampicin-Resistant Tuberculosis: Challenges and Advances in Diagnosis and Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 1349-1361. https://doi.org/10.5281/zenodo.15852361
 10.5281/zenodo.15852361
10.5281/zenodo.15852361
