1,2 Saraswathi Vidya Bhavan College of Pharmacy, Dombivli, Thane-421204, India
3Department of Pharmaceutics, OES’s Oriental College of Pharmacy, Sanpada, Navi-Mumbai:400705, India
Nasal drug delivery offers several benefits, including rapid absorption through the nasal mucosa, quick onset of action, and the ability to bypass presystemic metabolism. In the present study, nasal mucoadhesive in situ gels of the anti-epileptic drug Topiramate were developed using Gellan gum and Xanthan gum. These gels were evaluated for various parameters such as pH, gelling time, viscosity, drug content, drug diffusion, and ex vivo permeation. The pH of the formulations ranged from 5.9?±?0.01 to 6.3?±?0.03, which falls within the acceptable range, suggesting minimal risk of nasal irritation. In vitro drug release studies demonstrated a controlled release profile, with the optimized formulation (G3) achieving a maximum drug release of 97.16?±?0.54% within 210 minutes. Ex vivo permeation testing of the G3 formulation over 5 hours showed a permeation rate of 85.56?±?0.20%. The G3 formulation was also subjected to a one-month stability study, during which it maintained its stability and performance. Overall, the results suggest that this in situ gel system is a promising approach for nasal delivery of Topiramate.
Epilepsy is one of the most common neurological disorders worldwide, characterized by recurrent and unpredictable seizures due to abnormal brain nerve cell activities [1]. However, despite the availability of many antiepileptic drugs (AEDs), a significant number of people with epilepsy still have poor seizure control, unacceptable side effects and low compliance to therapy [2]. The need for new therapeutic strategies that can address these challenges is still paramount.
Over the years there has been increasing interest in intranasal drug delivery as an alternative method for administering AEDs [3]. Intranasal administration offers several advantages over oral or parenteral routes such as rapid onset of action, avoiding first-pass metabolism and enhanced patient compliance [4]. Furthermore, the development of in situ gel formulations has further improved the therapeutic potential of intranasal delivery by enhancing drug retention within the nasal cavity and prompting sustained drug release [5].
This research article focuses on exploring how intranasally administered in-situ gel formulations can be used to deliver Topiramate; a broad-spectrum AED that is currently widely prescribed for various types of seizures and epileptic syndromes [6]. Topiramate exhibits multiple mechanisms of action, including enhancement of γ-aminobutyric acid (GABA)ergic neurotransmission, inhibition of voltage-gated ion channels, and modulation of glutamatergic neurotransmission, making it a versatile therapeutic option for epilepsy [7]. One of the reasons behind the development of an intranasal in situ gel formulation for Topiramate is overcoming the limitations of traditional dosage forms such as low bioavailability, high variability in absorption and dose-dependent adverse effects. The introduction of an intranasal in situ gel formulation allows the sustained release of drugs after permeation into the brain through exploiting the sustained release of the in-situ gels. This was inspired by the advantages of intranasal drug delivery together with the sustained-release property of the in-situ gel aiming for optimal therapeutic outcomes in the management of epilepsy [8-9].
The purpose of the present work was to develop a nasal delivery system of an antiepileptic drug- Topiramate based upon the concept of ion activated in situ gelation and simultaneously to evaluate its performance by various in-vitro and ex-vivo tests so as to check the applicability of formulation for nasal use.
Material
Topiramate was generously supplied as a gift sample by Kopran Ltd., Mumbai. The dialysis membrane with a molecular weight cut-off of 12,000–14,000 was obtained from Sigma Aldrich. All other chemicals and analytical reagents used in the study were of analytical grade, sourced from S.D. Fine Chemicals Ltd. (Mumbai, India), and utilized without further modification. Fresh drug and buffer solutions were prepared prior to each use.
Formulation of Intra Nasal In-situ Gel of Topiramate
A polymeric solution containing gellan gum and xanthan gum was prepared by dissolving the polymers in distilled water, followed by mechanical stirring for 2–3 minutes to achieve a uniform mixture. Preservatives such as ethyl paraben, mannitol, and polyethylene glycol were added to the solution, which was then briefly heated in a water bath. After heating, the mixture was allowed to cool to room temperature. Topiramate, the active drug, was dissolved in a small amount of ethanol and subjected to sonication to ensure even dispersion. This drug solution was gradually incorporated into the polymer mixture under continuous stirring until complete dissolution of the drug was achieved. The final formulation was transferred to a clean glass beaker and made up to 10 mL with distilled water. It was then stored in refrigerated conditions until further use [10-11].
Table 1: Composition of different formulation of intra nasal in-situ gel of topiramate
|
Sr. No. |
Ingredients |
G1 %w/v |
G2 %w/v |
G3 %w/v |
G4 %w/v |
|
1. |
Topiramate |
0.25 |
0.25 |
0.25 |
0.25 |
|
2. |
Xanthan Gum |
0.25 |
0.25 |
0.25 |
0.25 |
|
3. |
Gellan Gum |
0.5 |
1.0 |
1.5 |
2.0 |
|
4. |
Ethyl Paraben |
0.10 |
0.10 |
0.10 |
0.10 |
|
5. |
PEG |
0.2 |
0.2 |
0.2 |
0.2 |
|
6. |
Mannitol |
0.15 |
0.15 |
0.15 |
0.15 |
|
7. |
Distilled Water |
q.s. |
q.s. |
q.s. |
q.s. |
Characterisation of Intranasal In situ Gel
Prepared formulations were evaluated for the following physical parameters:
All the prepared formulations were visually examined for their color, clarity, consistency, and to check for the presence of any lumps in the preparation [12].
The gelation process refers to the transformation of the formulation from a liquid (sol) to a gel state upon administration. To determine the gelling time, 2 mL of the prepared formulation is placed in a test tube, followed by the addition of a small quantity of simulated nasal fluid. This fluid, designed to replicate the nasal environment, consists of sodium chloride (0.745 g), potassium chloride (0.12 g), calcium chloride dihydrate (0.005 mg), and distilled water up to 100 ml. The addition of this simulated nasal fluid triggers the gelation process, and the time required for the formulation to convert into a gel is recorded as the gelling time [13].
The syringeability test was conducted by transferring the freshly prepared formulations into a 5 mL plastic syringe fitted with a 20-gauge needle, filling it to a consistent volume of 1 mL. Formulations that could be easily expelled through the syringe were marked as "pass," while those that were difficult to dispense were classified as "fail" [14].
One ml of the prepared in situ gel was diluted with distilled water, A Digital pH meter which was previously calibrated was used for the determination of pH of the resulting solution [15].
Spreadability was evaluated by placing an excess amount of the in situ gel sample between two glass slides. A 100 g weight was placed on top for 5 minutes to apply uniform pressure, ensuring even thickness of the gel layer. Spreadability was measured as the time (in seconds) it took for the two slides to slide apart under the applied load. The spreadability value was expressed in gram-centimeter per second [16].
The viscosities of the formulations, both before and after gelation, were measured using a Brookfield™ viscometer (AMETEK) fitted with Spindle 61. To mimic physiological conditions, the temperature was maintained at 37?±?0.5°C. Measurements were taken at a constant rotational speed of 100 revolutions per minute (rpm). The viscosity of each sample was determined by assessing the resistance faced by the spindle while rotating within the formulation [17].
1ml of prepared formulation were taken in volumetric flask containing 50ml of methanol. The flask was then sonicated to solubilize the drug. The resultant solution was then filtered through a 0.45μm membrane filter. Measurements were made by UV visible spectrophotometer at 263 nm using methanol as blank. The procedure was followed for all the developed formulations individually [12,18].
The in vitro diffusion study of the formulated in situ gels was performed using a Franz diffusion cell with a diameter of 2.0 cm and a capacity of 12 mL. A dialysis membrane with a molecular weight cut-off of 12,000–14,000 kDa was used as the diffusion barrier. Prior to the experiment, membrane sections were soaked in phosphate buffer (PB) at pH 6.6 for 24 hours. The diffusion cell was filled with the same buffer, and the pre-soaked dialysis membrane was carefully mounted. The temperature was maintained at 35°C to simulate physiological conditions. A 1 mL sample of the gel formulation was placed in the donor compartment, and gelation was triggered using simulated nasal fluid (SNF). At predetermined time intervals (30, 60, 90, 120, 150, 180, and 210 minutes), samples were withdrawn from the receptor chamber and replaced with fresh PB pH 6.6. The collected samples were appropriately diluted with the same buffer, and the drug content was analyzed using a UV spectrophotometer at 263 nm, using PB pH 6.6 as the blank [19].
Figure 1: Immediate gel formation upon administration, indicating the rapid in situ gelation process of the formulated solute
The ex vivo permeation study was carried out using a Franz diffusion cell with a 12 mL receptor compartment filled with phosphate-buffered saline (PBS) at pH 6.6. Goat nasal mucosa, sourced from a local slaughterhouse and trimmed to appropriate size, was used as the permeation membrane due to its close resemblance to human nasal tissue. The mucosal tissue was carefully positioned over the receptor compartment to ensure firm contact with the PBS. 1 mL sample of the in-situ gel was placed in the donor chamber of the cell and gelation was triggered using simulated nasal fluid (SNF). At predetermined time points, samples were collected from the receptor compartment and replaced with fresh PBS. These samples were then suitably diluted and analysed spectrophotometrically at 263 nm to determine drug content. This study specifically examined the optimized G2 in situ formulation to assess its drug permeation profile across the goat nasal mucosa [20-21].
The optimised insitu gel formulation (G3) underwent stability evaluation for 1 month at room temperature (30±2ºC) and analysed for appearance, pH, drug content and in-vitro drug release [22].
RESULT AND DISCUSSION
All the developed formulations were found to be clear and transparent exhibited excellent homogeneity, with no lumps observed, indicating a uniform distribution of the drug throughout the formulation.
The gelling time of the formulations varied from 10.2?±?0.35 seconds to 4.6?±?0.48 seconds, with formulation G3 demonstrating the most favorable gelling time. Detailed gelling times for all formulations are presented in Table 2 and Figure1.
Formulations ranging G1-G3 successfully passed the syringeability test and showed good syringeability, while formulation G4 did not, as detailed in Table 2. This test was performed to confirm that the formulations possessed appropriate flow properties to allow smooth delivery of the in-situ sol to the target site. Syringeability is mainly affected by three factors: the system’s viscosity, flow rate, and needle specifications, with polymer concentration and viscosity being the most critical determinants.
The pH of all in situ gel formulations ranged from 5.9?±?0.01 to 6.3?±?0.03, demonstrating their appropriateness and compatibility for nasal delivery while minimizing the risk of irritation to the nasal tissues. Detailed pH values for each formulation are provided in Table 2.
The prepared in situ gel exhibited good spreadability, allowing for easy application of the drug. The spreadability of the optimized formulation was measured at 36.6?±?1.32 gm·cm/sec. Results of the spreadability studies are presented in Table 2.
Viscosity is a key factor for intranasal in situ gel formulations, as they should have low viscosity during administration for easy application, and higher viscosity afterward to ensure they stay at the site of application. In formulations G1 through G4, viscosity increased with polymer concentration. Viscosity measurements for both the in-situ sol and gel states were performed at 100 rpm, with the G4 formulation showing the highest viscosity. The viscosity of the G3 formulation was deemed ideal for the intended nasal delivery. The viscosities of the in-situ sol and gel formulations are illustrated in Figure 2.
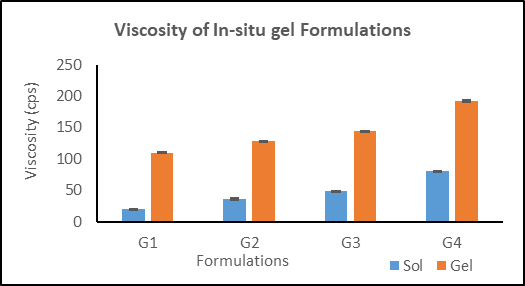
Figure 2: Viscosity of In-situ gel Formulations
The drug content of all prepared in situ gel formulations was measured, with results falling within an acceptable range of 92.68?±?0.61% to 97.32?±?0.41%, indicating uniform drug distribution across the formulations. The highest drug content was observed in the G3 formulation, at 97.32?±?0.41%. While drug content generally increased proportionally with polymer concentration, formulations with excessively high polymer levels showed slightly lower drug content compared to others. The detailed drug content data is presented in Table 2.
Table 2: Gelling time, Syringeability, pH, Spreadability, Gel strength, and Drug content of different insitu gel formulations
|
Formulations |
Gelling Time (sec) |
Syringeability |
pH |
Spreadability (gm.cm/sec) |
Drug Content (%) |
|
|
G1 |
10.2± 0.35 |
Pass |
5.9± 0.01 |
25.8± 1.17 |
94.68± 0.61 |
|
|
G2 |
8.5± 0.21 |
Pass |
6.1± 0.02 |
28.3± 1.24 |
96.52± 0.56 |
|
|
G3 |
5.2± 0.61 |
Pass |
6.2± 0.02 |
36.6± 1.32 |
97.32± 0.41 |
|
|
G4 |
4.6± 0.48 |
Fail |
6.3± 0.03 |
44.2± 1.51 |
92.85± 0.75 |
In-vitro release studies of various drug-loaded in situ gel formulations were conducted over a period of 210 minutes using PBS at pH 6.6, chosen to simulate the nasal environment. The pH and temperature were maintained consistently throughout the experiment. Among the formulations, G3 exhibited the highest drug release, reaching 97.16?±?0.54%. The polymer concentration was found to significantly influence the drug release pattern, with drug release generally increasing as polymer concentration increased. However, excessively high polymer concentrations, as seen in formulation G4, negatively impacted the in vitro drug release. Therefore, the G3 formulation, which demonstrated the greatest percentage of drug release, was identified as the optimized formulation.
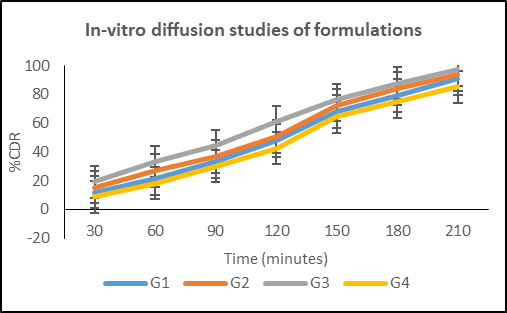
Figure 3: In-vitro diffusion studies of in-situ gel formulations
The G3 formulation was further evaluated through ex-vivo permeation studies using goat nasal mucosa. The permeation profile of the G3 formulation is illustrated in Figure 4, showing that the percentage of drug permeated after 300 minutes was 85.26?±?0.20%.
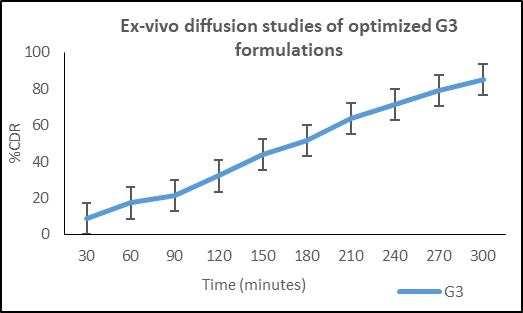
Figure 4: Ex-vivo diffusion studies of optimized G3 formulations
The stability study of the optimized formulation (G3) was conducted at 30 ± 2°C and 60 ± 5% relative humidity for one month. Throughout this period, the formulation maintained its clarity, with no significant changes detected in pH, drug content, or in vitro drug diffusion profile. Therefore, the optimized formulation demonstrated good stability under the specified temperature and humidity conditions.
CONCLUSION
The objective of this study was to develop a nasal delivery system for the antiepileptic drug Topiramate, utilizing the ion-activated in situ gelation properties of gellan gum. The optimized in situ gel formulation, G3, exhibited favorable pH, gelling time, viscosity, and drug release characteristics. Additionally, the formulation maintained good stability at room temperature for up to 30 days. Delivering Topiramate via this in situ gel to the nasal cavity shows promise as an effective and practical alternative to traditional treatment methods. The results of this study indicate strong potential for the clinical application of this formulation in epilepsy management.
STATEMENTS AND DECLARATION
Originality of Work: This manuscript represents original work that has not been previously published and is not under consideration for publication elsewhere. All authors have contributed significantly to the study and have reviewed and approved the final manuscript.
Conflict of Interest: The authors declare that they have no conflicts of interest, Financial or otherwise.
Funding: The authors did not receive any funding for the submitted work.
Ethical Considerations: Not applicable.
REFERENCES



Krish Shetty*, Madhuri Jain, Suraj Yadav, Formulation And Evaluation of In-Situ Gelling System of Topiramate for Epilepsy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 4030-4037. https://doi.org/10.5281/zenodo.15731949
 10.5281/zenodo.15731949
10.5281/zenodo.15731949
