Sudhakarrao Naik Institute of Pharmacy Pusad.
In the treatment of respiratory conditions like asthma and chronic obstructive pulmonary disease (COPD), dry powder inhalers (DPIs) have emerged as a crucial substitute for pressurized metered-dose inhalers (pMDIs). The desire for more effective and user-friendly drug delivery systems, as well as environmental concerns about the chlorofluorocarbon (CFC) propellants used in pMDIs, have been major factors in the move towards DPIs. The removal of propellants, enhanced drug stability, increased dose capacity, and greater patient compliance are just a few benefits that DPIs provide. These inhalers aerosolize and deliver micronized medication particles—often combined with carriers like lactose—directly to the lungs by using the patient's inspiratory effort. This technique improves treatment efficacy while lowering systemic adverse effects by enabling a quick commencement of action and tailored distribution to the respiratory system. The patient's breathing technique, formulation properties, and device design are some of the variables that affect how effective DPIs are. Optimizing particle size (usually 1–5 µm), enhancing powder flowability, and guaranteeing dosage uniformity are important components of DPI technology. To obtain the required particle qualities, a variety of production techniques are used, including solvent evaporation, micronization, spray drying, and freeze drying. DPIs have drawbacks despite their benefits, including manufacturing complexity, dosage inaccuracy, and patient variability. The goal of ongoing research is to create optimal DPI systems that are easy to use, affordable, portable, and able to administer a constant, therapeutically appropriate dose for a variety of illnesses. DPIs are anticipated to become progressively more important in respiratory and systemic medication delivery as technology develops.
Introduction to Dry Powder Inhalers
Inhalation drug delivery has been a longstanding method for administering active pharmaceutical agents to treat respiratory diseases. Traditional asthma treatments, including bronchodilators, steroids, mast cell stabilizers, and anticholinergic drugs, have predominantly utilized pressurized metered-dose inhalers (pMDIs). However, concerns about the environmental impact of chlorofluorocarbon (CFC) propellants have led to the development and widespread evaluation of alternative devices such as dry powder inhalers (DPIs). DPIs use fine drug particles (about 5 µm) combined with a carrier, such as lactose, to improve flow and dose uniformity. The medication powder is inhaled into the deep lungs via a dry powder inhaler device. In DPIs, the patient's inspiratory effort is used to aerosolize and de-agglomerate the powder. Turbulence is necessary for successful drug administration because it breaks up bigger agglomerates into smaller, inhalable particles. This turbulence is caused by producing resistance to airflow within the DPI device, and the amount of effort required to generate the requisite airflow is determined by the resistance. Although flow rates vary amongst DPIs, a range of 60-90 L/min is typically required. Dry powder inhalers have grown in popularity due to their propellant-free design, good patient compliance, capacity to transport greater doses, enhanced drug stability, and potential for patent protection. These benefits have fueled significant developments in DPI technology, boosting the potential for pulmonary drug delivery in both local and systemic treatments. However, DPIs are complex, and their efficiency is regulated by a number of parameters, including inhaler design, powder formulation, and patient airflow. DPI performance has improved significantly over the last decade thanks to customized drug particles and redesigned excipient systems. For millennia, the concept of medicine administration by inhalation aerosols has been critical in the treatment of respiratory diseases. According to historical documents, the practice of breathing powdered substances originated in ancient Egypt and Greece. Newton and Nelson patented early DPIs in the nineteenth century, but inhalation therapy did not take off until 1948, when Abbott introduced the Aerohalor, which delivered penicillin. While inhalation drug delivery has been around for a long time, early devices had issues with variable dose. After the pharmaceutical industry developed precise dose control, inhalation therapy transformed the treatment of respiratory illnesses, particularly asthma. Drug delivery through inhalation has greatly improved in recent years, offering efficient drug administration for both systemic and local lung diseases. There are still issues, though, especially with guaranteeing steady dosage administration and reducing toxicity from excessive lung deposition. Each of the four main inhalation aerosol delivery systems—dry powder inhalers (DPIs), pressurized metered-dose inhalers (PMDIs), and nebulizers—has unique benefits, drawbacks, and formulation compatibility. Research on respiratory drug delivery during the last 20 years has mostly concentrated on enhancing drug bioavailability and substituting CFC propellants. While CFC-based inhalers have been effectively supplanted by hydrofluoroalkane (HFA) propellants and DPIs, nanotechnology is still being investigated for targeted pulmonary medication delivery. However, there are still issues with attaining constant dose delivery and greater percentages of respirable medication. The basic working principles of inhaler devices, formulation optimization, patient noncompliance, inappropriate inhaler handling, inappropriate therapy selection, and patient preference for particular inhaler types are the causes of these challenges. To further increase the efficacy of DPI-based drug delivery systems, these issues must be resolved. [1],[2],[3]
Inhalers
Inhalers are devices made especially to administer drugs directly to the lungs; they usually contain either a mixture of co-spheronized drug and lactose or micronized drug particles that are loosely aggregated into tiny spherules. The primary goal of inhaler design and production is to guarantee effective and efficient drug delivery, focusing on the respiratory system to produce quick therapeutic effects. Compared to conventional oral drugs, inhalers work in a very different way. Inhalers release a tiny mist or aerosol that patients inhale straight into their lungs, bypassing the digestive process and the stomach.
This allows for a more immediate onset of action, as the medication can quickly reach the site of action within the airways and alveoli, where it can exert its effect. [4], [5], [6]
Types of Inhalers
There are different types of Inhalers they are as below. [7] [8] [9] [10]
1. Pressurized metered-dose inhalers (PMDIs)
2. Soft mist inhaler (SMI)
3.Nebulizer
4. Dry powder inhalers (DPIs)
1. Pressurized Meterd-Dose Inhaler (PMIDS): -
A Pressurized Metered Dose Inhaler (PMDI) is a portable device designed to provide a precise, measured dose of aerosolized medication straight into the lungs. It is frequently recommended for respiratory issues like asthma and chronic obstructive pulmonary disease (COPD). Below are the essential details regarding PMDIs.:
Canister: Holds the medication in a solution or suspension along with a propellant.
2. Actuator: The part of the device that releases the drug when pressed.
3. Mouthpiece: Directs the medication into the patient's airways.
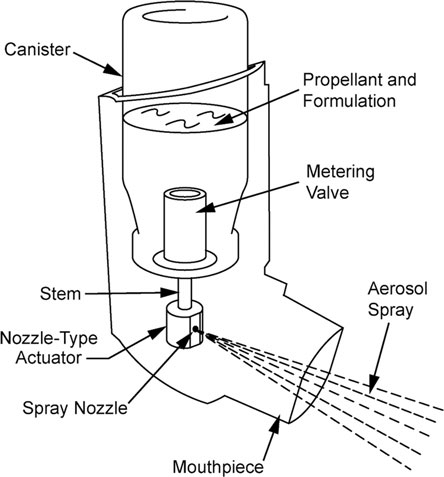
Figure 1: Pressurized Metered Dose Inhaler
2. Soft mist inhaler (SMI): -
A Soft Mist Inhaler (SMI) is a more recent form of inhaler that provides medication in a gentler, slow-moving mist, enhancing the deposition of the drug in the lungs. It is mainly utilized for managing respiratory issues such as asthma and chronic obstructive pulmonary disease (COPD). Below are the main features and details regarding SMIs:
Components:
Cartridge: Holds the liquid medication.
Actuation Mechanism: A spring-driven system creates the soft mist without the need for a propellant.
Mouthpiece: Delivers the mist directly into the patient’s airways.
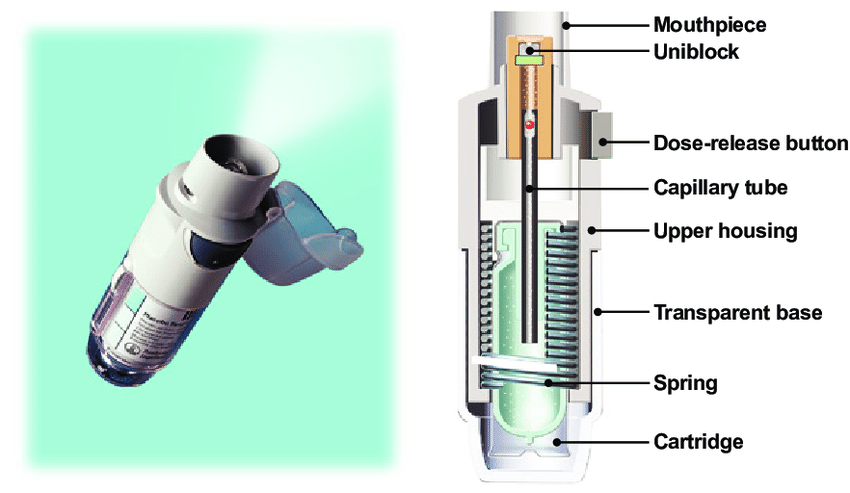
Figure 2: Soft Mist Inhaler
3. Nebulizer: -
A nebulizer is a healthcare instrument that converts liquid medication into a fine mist or aerosol, allowing it to be inhaled straight into the lungs. It is frequently employed for managing respiratory ailments like asthma, chronic obstructive pulmonary disease (COPD), and various other lung disorders. Nebulizers are particularly beneficial for patients who struggle with using inhalers, including young children, older adults, or individuals with significant respiratory challenges. [11]
Components of nebulizer: -
Compressor: Powers the nebulizer, forcing air through the liquid medication to create the mist.
Nebulizer cup: Holds the liquid medication.
Tubing: Connects the nebulizer cup to the compressor.
Mouthpiece or Mask: Used by the patient to inhale the mist.

Figure 3: Nebulizer
4. Dry Powder Inhalers: -
The technology behind DPI devices is essential for dispersing powder mixtures into a fine aerosol of drug particles that can be inhaled effectively through aerodynamic processes. DPIs are composed of either micronized drug particles that are loosely aggregated into small spheres or a mixture of the drug and lactose particles. The primary objective in the design and production of DPIs is to create powders with a high potential for aerosolization, which guarantees that a large drug dose is effectively delivered to the lung surface. The efficiency of DPIs is largely determined by how well the particles aerosolize, which is greatly affected by the physicochemical characteristics of the formulation. These characteristics include particle size distribution, density, surface morphology, shape, inter-particle interactions, and solid state. Particles in the 1–5 µm range work better for deep lung administration, while those with an aerodynamic diameter of 5–10 µm are often appropriate for deposition in the airways. Usually, bottom-up methods are used to produce respirable-sized particles. Spray drying, a one-step process that turns a medication solution into dry particles with a limited size distribution, is one popular approach. The physical and chemical characteristics of the final particles can be precisely controlled by varying the spray-drying parameters, such as the type and concentration of the solution, as well as the drying gas temperature, flowrate, and inlet conditions.

Figure 4: Different types of dry powder inhales (Single -Dose, Multi unit dose, Multi dose DIPS)
Advantages of Dry Powder Inhalers:
1. Dry power via inhalation allows for the direct delivery of medication into the lungs.
2. The lungs are a perfect entry point for the systemic distribution of small molecules for the treatment of COPD because of their large number of capillaries and thin air-blood barrier.
3. The market for asthma and COPD devices is expanding at the quickest rate among dry powder inhalers (DPIs).
4. As an alternative, DPI particles may integrate poorly soluble compounds as smaller, distinct crystalline particles.
5. Powder can be made physically stable by creating amorphous or completely crystalline particles.
6. Compared to oral delivery, attain therapeutic benefits in the lungs at lower dosages. [12]
DISADVANTAGES:
1. Spray dryer is bulky and also expensive to install.
2. It has a low thermal efficiency that is a lot of heat is wasted during operation.
3. Maintenance Issues for Spray dryer mostly involves issues with the nozzle used.
Aspects of DPI Design [12] [13]
Formulation of Powders for Inhalation
Drugs that are administered by dry powder inhalers (DPIs) are made as mixes with an inactive excipient or as pure drug powders. The budesonide preparation utilized in the Turbuhaler DPI (AstraZeneca) is an illustration of a pure medication formulation. On the other hand, powder blends usually include an excipient, most often lactose, along with micronized medication particles. Although it can also be micronized, the lactose is often made up of bigger "carrier" particles. The best particle size distribution for an inhaled dry powder asthma medicine is widely thought to be approximately 5 µm, or possibly as much as 15 µm, for maximum therapeutic efficacy. However, because of cohesiveness and static charge, particles of this size are usually not free-flowing, which might make handling drugs during production and inhaler filling more difficult. These problems can lead to drug retention in the device, decrease dosage uniformity, and impact metering accuracy. Since a bigger powder mass is typically easier to meter precisely, the addition of excipients aids in improving dosage uniformity. Micronized particles can be produced into stabilized agglomerates with regulated homogeneity and hardness under particular manufacturing circumstances. For example, mometasone furoate and lactose agglomerates are used in the Twisthaler DPI (Schering-Plough), which is designed for handling and metering by controlled stabilization. These drug or drug-lactose agglomerates must be broken up into small particles by shear forces during inhalation so that airflow may carry them into the lungs. Particles smaller than 5 µm can reach the deeper airways, where deposition correlates with improved clinical outcomes.
Applications [25]
A Dry Powder Inhaler (DPI) is a device used to deliver medication directly to the lungs in the form of a dry powder. Here are some of its primary uses:
1. Treatment of Asthma: DPIs are commonly used to deliver bronchodilators (e.g., salmeterol) and corticosteroids (e.g., budesonide) to help open airways and reduce inflammation.
2. Chronic Obstructive Pulmonary Disease (COPD): DPIs provide medications that relax muscles in the lungs and reduce mucus production for those with COPD.
3. Pulmonary Fibrosis: DPIs are used to deliver antifibrotic drugs to help slow the progression of the disease.
4. Allergic Rhinitis: Sometimes used for the delivery of anti-allergy medications.
5. Emergency Relief: Fast-acting bronchodilators in DPI form can be used to relieve acute breathing difficulties.
6. Prevention: DPIs are often used daily as a maintenance therapy to prevent asthma attacks or exacerbations in chronic conditions.
Dry powder inhaler (DPI) devices
Dry powder inhalers (DPIs) are dry, free-flowing powdered medication formulations that can be made by micronating or spray-drying a mixture of the drug and an appropriate inert carrier. The resulting medication particles ought to enter the deep lung or act locally in the upper respiratory system. DPI devices are used to distribute DPI formulations as aerosols. As a result, a DPI device usually includes the dry formulation, an actuator, and a metering system (Figure 6). The formulation is contained in the bulk chamber, which is protected by an over-cap. To avoid contamination, a dust-cap is placed over the mouthpiece. The powder is drawn out of the chamber and sent to the mouthpiece for inhalation by the metering valve, which also features a repeatable measuring feature. To deliver the medication as a "respirable" aerosol, the patient must inhale negatively; however, this technique is difficult for patients with shallow breathing patterns, the elderly, and youngsters. The size and velocity of particles determine how they move through the respiratory system. By creating relatively big particles (above 5 µm) for deposition in the upper part of the respiratory system or smaller particles (e.g., below 4 µm) for deposition in the lower respiratory tract, the precise site of deposition can be regulated.
Inhaler Design and the Goals of Asthma Management [26]
Effectiveness and Compliance
Even while corticosteroids and inhaled bronchodilators work well to treat asthma, incorrect inhaler use can result in poor adherence and treatment failure. With the right composition and design, an inhaler can improve therapeutic results, increase adherence, and possibly decrease the frequency of doses. The design of the inhaler determines how comfortable it is for people to use and how easily healthcare professionals can show how to use it. Maintaining compliance depends heavily on the patient's comfort and level of pleasure with their inhaler. As a result, an inhaler should be affordable, discrete, long-lasting, and simple to use. A dose counter is helpful for self-management because the majority of portable asthma inhalers contain numerous doses. A dose counter facilitates timely refills, helps avoid inadvertently using an empty inhaler, and improves the ability of medical professionals to keep an eye on patient compliance.
Inhalers must give constant doses over the course of their lifetime and across several units in order to guarantee stable and predictable therapeutic outcomes. Regulatory agencies including the U.S. Food and Drug Administration (FDA) and the European Pharmacopoeia (EP) have set requirements for inhaler dose consistency in recognition of this.
Development of an Ideal DPI [27]
An inhalation device's design is essential to guaranteeing that drugs are delivered to the lungs effectively. The perfect gadget should be portable, reasonably priced, and easy to use. Additionally, it must offer a setting that preserves the physicochemical stability of the medication while guaranteeing reliable and consistent dosage. Furthermore, a high fine particle fraction (FPF) from the formulation should be delivered more easily by the device(Srichanaetal.,1998).
However, in order to provide the required airflow, patients must exert more inspiratory force when using devices with higher resistance. Children and newborns, as well as those with severe asthma, may find this difficult. Therefore, to optimize the therapeutic efficacy of DPI formulations, striking a balance between these parameters is crucial.
Key Characteristics of an Ideal DPI
For a DPI to be reliable, clinically effective, and widely accepted by patients, it should possess the following attributes:
Accessibility and ease of use: The gadget should be easy to use, lightweight, able to store several doses, andfitted with a dose counter that offers either visual or audio feedback. [28]
Precise and reliable dosage: It should provide constant dosages over a wide range of inspiratory flow rates, guaranteeing reliability over the inhaler's life and in comparison, to other devices of a similar nature. [28]
Particle size optimization: For efficient deep lung administration, the medication particles should fall within the ideal size range. [29]
Versatility:
The DPI ought to work with a range of medications and dose levels.
Minimum adhesion: To avoid drug loss and guarantee appropriate dosage, the formulation should contact with the device as little as possible.
Drug stability: During the drug's shelf life, the device needs to maintain it stable life
Costeffectiveness: the device should be reasonably priced without sacrificing performance.[29]
The mechanism to provide consumer feedback:
An integrated system should reassure the patient about correct inhaling technique and notify them of the number of doses left. An optimal DPI can guarantee efficient drug administration, improve patient adherence, and improve treatment outcomes by combining these characteristics.
Methods of preparation of dry powder
1.Spray Drying
2.Freeze Drying (Lyophilization)
3.Micronization
4.Solvent Evaporation
Spray Drying [15] [16]
The procedure known as "spray drying" turns an emulsion, solution, or other pharmaceutical preparation into powder in the form of nanoparticles or microparticles, which are then used to make tablets, capsules, or powder. One well-known method for producing particles is spray drying, which involves turning a liquid substance into dried particles. The idea behind the spray drying method Both procedures are spray drying and spray congealing, which depend on whether the solvent is removed or the solution is cooled. The most used industrial method for drying and particle creation is spray drying.
Principle: Three steps involved in spray drying:
1Atomization: of a liquid feed change into fine droplets.
2.Mixing: it involves the passing of hot gas stream through spray droplets which result in evaporation of liquids and leaving behind dried particles.
3.Dry: Dried powder is separated from the gas stream and collected.
Working: -
The drying of the medication and polymer mist in the air is the foundation of these procedures. These techniques are referred to as spray drying depending on how much solvent is removed.
The polymer is dissolved in a volatile organic solvent, such as acetone or dichloromethane, during the spray drying process. With rapid homogenization, the solid drug is distributed throughout the polymer solution.
A stream of hot air is then used to atomize this dispersion. The atomization leads to the development of tiny drops or a fine mist in which the solvent evaporates immediately leading to the formation of the microspheres in a size range 1-100µm.
Applications of spray drying method: -
Due to its exceptional performance and ability to meet GMP regulations, the spray drying process is highly popular among customers in the food and pharmaceutical industries.
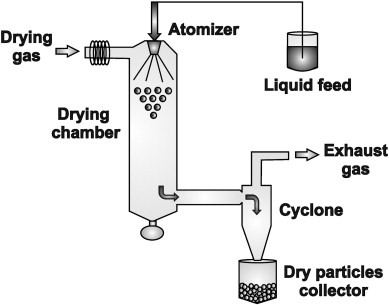
Figure 5: Spray drying
Advantages of spray drying method: -
1.A quick drying method.
2. Materials can be powered by drying them immediately.
3. Modifying the drying conditions and the requirements for product quality is simple.
4. The drying room has a specific negative pressure that ensures hygienic conditions during manufacturing, prevents dust from blowing into the workplace, and enhances product purity.
5. Reduced operator count and high production efficiency.
6. High-quality products and a large production capacity. Several hundred tons of spray can be produced every hour.
Disadvantages of spray drying method: -
1. The equipment is complicated, expensive, and covers a lot of ground.
2. Spray dryers and powder recovery devices are somewhat expensive.
3. The heat consumption is significant and the thermal efficiency is low.
Freeze Drying (Lyophilization) [17] [18]
Lyophilization, another term for freeze drying, is a sophisticated dehydration method that is frequently employed in the food, biotechnology, and pharmaceutical sectors. This approach is particularly useful for preserving perishable products, prolonging shelf life, and assuring the stability of temperature-sensitive chemicals. By removing moisture from a substance while keeping its structural integrity and bioactivity, freeze drying plays a significant role in boosting product quality and use.
The process of freeze drying involves three main stages:
Freezing: To turn the water content into solid ice, the substance is first frozen at very low temperatures. Maintaining the material's original composition, texture, and shape requires this procedure. Smaller ice crystals are formed via rapid freezing, which helps preserve the product's structure while it dries.
Primary Drying (Sublimation): In this stage, the ice turns straight into vapor without going through the liquid phase since the ambient pressure is drastically lowered in a vacuum chamber. We call this sublimation. This procedure is aided by controlled heating, which keeps heat-sensitive materials from degrading.
Secondary Drying (Desorption): Any residual bound moisture is recovered by progressively raising the temperature while under vacuum after the majority of the water has been removed. This stage guarantees that the finished product is stable for long-term storage and totally dry.
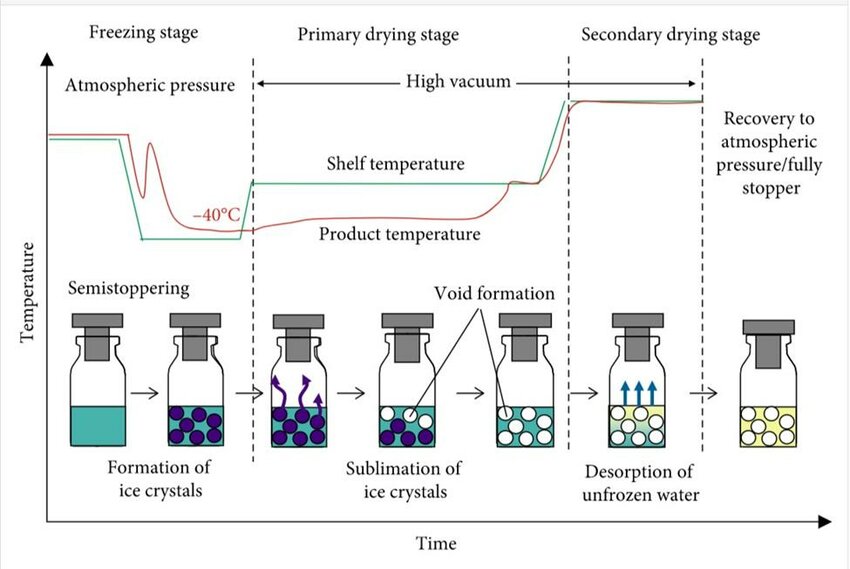
Figure 6: Freez Drying
Uses and Advantages of Freeze-Drying
Pharmaceuticals-Freeze drying
Pharmaceuticals Producing stable injectable medications, vaccines, antibiotics, and biologics such proteins and peptides requires freeze drying. Prior to administration, it makes reconstitution simpler and helps retain potency.
Food Industry: Freeze drying preserves nutrition, flavour, and texture while greatly increasing shelf life. It is used to preserve fruits, vegetables, coffee, and fast meals.
Biotechnology & Diagnostics: To preserve their stability and activity, enzymes, bacteria, probiotics, and diagnostic reagents are frequently freeze-dried.
Cosmetics & Skincare: High-performance skincare formulas employ lyophilized components to provide improved efficacy and a longer shelf life.
The advantages of freeze drying include:
Longer Shelf Life: Prevents microbiological development and deterioration, which facilitates easier transportation and storage.
Retention of Quality: Preserves food and medication's natural composition, flavor, color, and nutritional content.
Rehydration Capability: Freeze-dried products are very useful for a variety of applications since they can be readily reconstituted with water.
Despite its advantages, freeze drying is a time-consuming and energy-intensive procedure that frequently calls for specialized tools and carefully monitored temperatures. Nonetheless, it is a favored option in sectors where stability and quality are crucial due to its capacity to efficiently keep delicate materials.
Micronization [19][20]
A specialized method of lowering particle size, micronization entails shrinking solid particles to the micrometre or sub-micrometre range, usually fewer than 10 micrometres. This technique is frequently used to enhance the solubility, bioavailability, and performance of different compounds in the food processing, cosmetics, and pharmaceutical industries.
The following mechanical milling processes are commonly used to achieve micritization:
Jet milling: is a process that breaks down particles into small powders by accelerating them against one another with high-pressure air or gas. For materials that are sensitive to heat, this process creates ultra-fine particles with a limited size distribution.
Ball milling: The material is ground into fine particles in a revolving chamber filled with steel or ceramic balls. This technique is frequently applied to materials that need consistent particle size.
High-Pressure Homogenization: Often employed for emulsions and suspensions in pharmaceutical applications, this process involves forcing liquid formulations through a high-pressure system to minimize particle size.

Figure 7: Micronization Process
Applications and Benefits of Micronization
Pharmaceutical Industry: By expanding the surface area of poorly water-soluble medications, micronization improves their bioavailability and speeds up their dissolution and absorption in the body. Micronized particles are essential for accurate dosage and efficacy in a number of controlled-release formulations and inhalable medications.
Food Industry: Used to enhance the solubility, texture, and mixability of powdered food ingredients, including nutritional supplements, flavors, and spices.
Cosmetics and Skincare - Micronized pigments and active chemicals are utilized in makeup, sunscreens, and skincare formulations to increase product performance and stability.
Chemical and Agricultural sectors: Fine particles enhance the efficacy and dispersion of insecticides, fertilizers, and specialty chemicals in the chemical and agricultural sectors.
The primary advantages of micronization include:
Improved Bioavailability and Solubility: Smaller particles dissolve more easily, increasing the effectiveness and absorption of drugs.
Better Stability and Uniformity: This guarantees a steady distribution of particles, which is essential for industrial applications and medication formulations.
Improved Mixing and Dispersion: The uniformity of the final product is enhanced by the more efficient blending of micronized powders with additional additives. However, there are drawbacks to micronization as well, namely the possibility of electrostatic charge accumulation and material loss during processing. Furthermore, sophisticated milling methods may be needed to achieve ultra-fine particle sizes, which can be costly.
Solvent Evaporation Technique for Dry Powder Inhalers (DPIs) [20] [21]
One popular technique for creating microparticles and nanoparticles for dry powder inhalers (DPIs) is solvent evaporation. For effective lung deposition and therapeutic efficacy, this method works especially well for creating drug-loaded particles with regulated size, porosity, and drug dispersion.
Principle of Solvent Evaporation:
In order to create an emulsion or suspension, the medicine and excipient (such as a polymer or carrier material) are dissolved in a volatile organic solvent using the solvent evaporation method. The solid medication particles with the required properties for inhalation are then left behind after the solvent is eliminated through evaporation.
Steps Involved in the Solvent Evaporation Process
1. Preparation of the Drug Solution or Emulsion
A volatile organic solvent, such as acetone, ethyl acetate, or dichloromethane, dissolves the medication. If necessary, a polymer (such PVP or PLGA) is added to improve stability, regulate drug release, or alter particle characteristics. To create an emulsion, the medication solution is dissolved in an aqueous phase that contains stabilizers or surfactants (like PVA or lecithin). The solubility of the drug and the desired properties will determine whether the emulsion is single (O/W) or double (W/O/W), depending on the technique.
2. Evaporation of the Solvent
The organic solvent is allowed to evaporate by stirring the emulsion at a higher temperature or with less pressure. Drug particles precipitate and solidify as microspheres or nanospheres as the solvent evaporates.
3. Collection and Drying of Particles
After being gathered by centrifugation or filtration, the solid particles are cleaned to get rid of any remaining stabilizers or surfactants. To guarantee total solvent elimination and improve stability, the particles are subsequently vacuum-dried or freeze-dried (lyophilized).
Advantages of Solvent Evaporation for DPIs
Control over Particle Size and Morphology: The procedure makes it possible to adjust the properties of the particles for the best lung deposition.
Increased Drug Stability: Drugs can be shielded from deterioration and have their shelf life extended by encapsulation in polymers or excipients.
Enhance drug Dispersion: In DPI formulations, enhances flowability and decreases particle agglomeration.
Sustained or regulated Release: Using polymers can help reduce the frequency of doses by enabling regulated medication release.
Compatibility with a Range of Drugs: It works well with hydrophilic and hydrophobic medications, such as proteins, peptides, and tiny compounds.
Challenges & Considerations
Removal of Residual Solvents: In order to comply with safety and regulatory requirements, organic solvents must be completely removed.
Particle Size management: Accurate management of process parameters is necessary to achieve the optimal 1–5 µm particle size range for pulmonary medication administration.
Aggregation & Flow Properties: Additives, such lactose, are necessary to improve dispersibility since fine particles may stick to one another.
Scale-Up Limitations: Because of batch-to-batch variability and the requirement for specialized equipment, industrial-scale production might be difficult.
Applications in Dry Powder Inhalers
Pulmonary Drug Delivery – Used for asthma, COPD, and other respiratory diseases, ensuring deep lung penetration.
Encapsulation of Biologics – Effective for stabilizing proteins, peptides, and mRNA-based therapeutics.
Combination Therapy – Enables co-formulation of multiple drugs in a single DPI formulation.
Regulatory considerations
A number of factors must be taken into account in order to determine the performance and quality of inhaled medicinal products. ICH Q1 and Q2, which regulate the components (Q1) and their quantitative proportion (Q2) in the preparation, must be followed while controlling the medication formulation. The gadget is accompanied by a drug master file providing requirements and controls on its manufacturing. According to the US Food and Drug Administration (US FDA), assay, impurities and degradants, leachables, foreign particle matter, moisture content, net content, microbiological load, and device characteristics are critical quality aspects of DPI formulations. As outlined in compendia (such as the United States Pharmacopeia [USP], European Pharmacopeia [EP], and Japanese Pharmacopoeia [JP]) and regulatory guidance documents, like those issued by the US FDA, the drug product (formulation and device) is also subject to performance testing to assess the APSD and delivered dose uniformity (DDU). [24]
Evaluation Test [22][23]
CONCLUSION:
Because they provide a dependable, propellant-free, and patient-friendly substitute for conventional inhalation systems, dry powder inhalers (DPIs) have completely changed the respiratory drug delivery landscape. Rapid therapeutic action, enhanced drug absorption, and less systemic side effects are made possible by their capacity to transport medication straight to the lungs. The desire for more effective drug delivery systems and ecologically friendly devices has fueled the development of DPIs. Although DPIs have several benefits, such as increased portability, stability, and dose accuracy, they also have drawbacks because of formulation complexity, inhaler design, and patient-specific variables including inhaling technique and strength. To maximize their therapeutic potential, these issues must be resolved by continued developments in particle engineering, device innovation, and patient education. The perfect DPI should be simple to use, affordable, compatible with a wide range of drugs, and able to administer accurate and consistent dosages. DPIs are positioned to play an increasingly important role in treating respiratory illnesses as well as facilitating the systemic distribution of a variety of medications, as research continues to improve device performance and refine the physicochemical qualities of powders. The future influence and use of DPIs in clinical practice will ultimately depend on how well technical advancements and user-centric design are integrated.
REFERENCES

Bhumika Bidwaik*, Dr. Ravikiran Wakade, Aman Noorani, Sakshi Patil, Rehan Beniwale, Dry Powder Inhalers (DPI): A Comprehensive Review Article on Dry Powder Inhaler (DPI), Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 1758-1773. https://doi.org/10.5281/zenodo.15878066
 10.5281/zenodo.15878066
10.5281/zenodo.15878066
