Kamalakshi Pandurangan College of Pharmacy, Ayyampalayam Tiruvannamalai, Tamilnadu, India.
Bioelectronic medicine (BEM) is an interdisciplinary field integrating neuroscience, bioengineering, and clinical medicine to diagnose and treat disease through targeted modulation of the body’s electrical signaling networks. Using implantable or wearable devices, BEM can influence neural circuits, regulate organ function, and modulate immune responses with high precision[1]. Unlike pharmaceuticals, which rely on chemical pathways, BEM directly interfaces with the nervous system, enabling rapid and reversible therapeutic effects. Recent advances in flexible electronics, microfabrication, and artificial intelligence have accelerated the development of minimally invasive, closed-loop systems capable of realtime, personalized therapy[2]. Clinical applications now span neurology, cardiology, psychiatry, and immunology, addressing conditions such as epilepsy, Parkinson’s disease, heart failure, and autoimmune disorders. This article reviews the principles, historical evolution, core technologies, clinical applications, regulatory aspects, and future directions of BEM, highlighting its potential to transform patient care.
The human body functions as a complex bioelectrical network, with the nervous system using precisely timed electrical impulses to coordinate organ and cellular processes. Unlike pharmaceuticals, which try to alter these processes by means of chemical routes, bioelectronic medicine aims to directly affect electrical communication [1]. Advances in materials science, neurophysiology, and computational modelling are driving this paradigm change, making precise, flexible, and reversible treatments possible [2]. BEM is seen as the "next therapeutic frontier" following the biologics era and combines systems biology, electronics, and neuroscience [3]. It touches on immunology, psychology, cardiology, endocrinology, and rehabilitation medicine in addition to neurology.
Historical Evolution of Bioelectronic Medicine
While contemporary BEM is a 21st-century invention, its origins can be found in centuries-old methods. Early attempts to electrically stimulate muscle and nerve tissue began in the 18th century when Luigi Galvani demonstrated "animal electricity"[4] . A major turning point was the mid-20th century clinical acceptance of cardiac pacemakers, which demonstrated the viability of chronic bioelectronic intervention[5] . The present concept of BEM was established over the last 20 years by the development of vagus nerve stimulation (VNS) for depression, responsive neurostimulation for epilepsy, and deep brain stimulation (DBS) for Parkinson's disease [6].
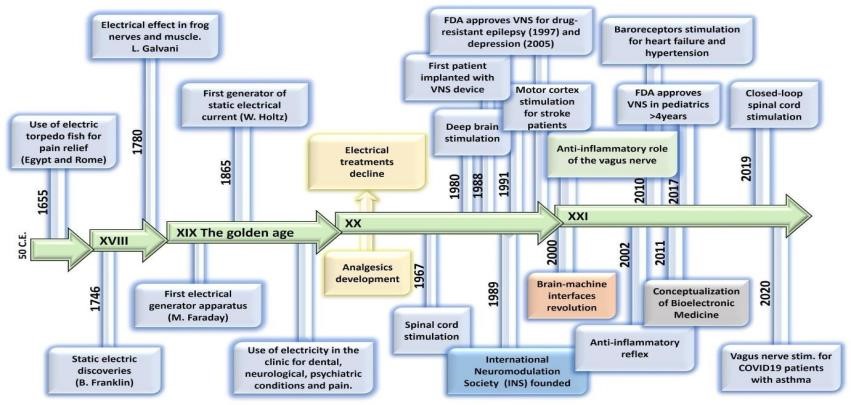
Fig.1 Evolution of Bioelectronic Medicine
Core Principles & Technologies
Neural Interfaces and Signal Decoding:
Biocompatible neural interfaces that can read and activate specific nerve fibres are the foundation of BEM devices[7]. Selective therapeutic route targeting is made possible by the decoding of peripheral nerve signals utilising methods including multi-electrode recordings, optogenetics, and high-resolution electroneurography [8].
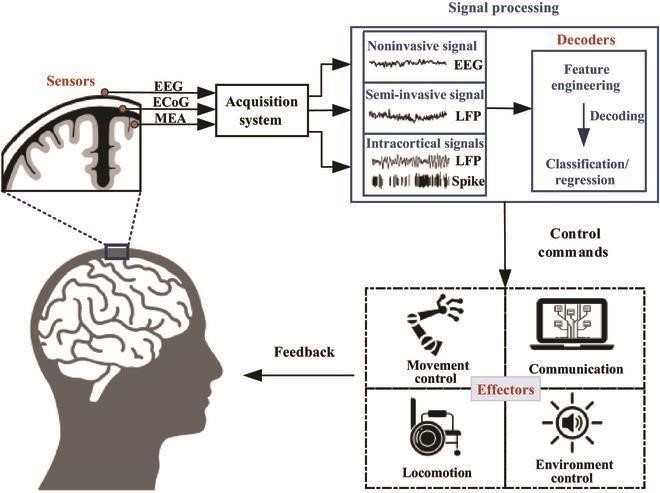
Fig.2 Neural Interfaces and Signal Decoding Closed-Loop Neuromodulation:
Real-time physiological status monitoring and dynamic stimulation parameter adjustment are made possible by closed-loop devices that combine sensors and processors[9]. This method increases therapy personalisation, minimises negative effects, and uses less energy.

Fig.3 Loop Neuromodulation
Power and Wireless Communication:
To operate for extended periods of time without requiring periodic battery replacement surgery, modern devices employ wireless charging, inductive coupling, or biofuel cells[10] . Secure wireless communication methods enable real-time monitoring and external programming.
AI Integration:
Robots can autonomously optimise stimulation and understand patient-specific brain patterns thanks to artificial intelligence[11]. In the case of complicated, varying illnesses such as mood disorders, chronic pain, and epilepsy, AI-driven neuromodulation holds particular promise.
Translational Research and Clinical Trials
Bringing bioelectronic medicine from laboratory innovation to bedside therapy requires a multidisciplinary translational pathway involving engineers, neuroscientists, clinicians, and regulatory bodies. Early-stage research often begins with preclinical models that map neural circuits, characterize electrical signatures of disease states, and assess the safety of prototype devices. Animal studies—ranging from rodents to large mammals—are critical for understanding both the efficacy and the long-term biocompatibility of neural implants. Following preclinical validation, first-in-human feasibility studies are conducted to test device safety, tolerability, and initial therapeutic effects. These pilot studies help refine stimulation parameters, electrode placement strategies, and closed-loop algorithms before scaling to larger trials.
Spinal cord stimulation for chronic pain management showed long-term analgesia without opioid dependency. Ongoing multicenter trials are now exploring organ-specific neuromodulation, AI-assisted closed-loop devices, and minimally invasive bioelectronic systems that can be deployed in outpatient settings. These studies not only generate evidence for clinical adoption but also inform device design for safety, durability, and cost-effectiveness. The success of translational research in BEM depends on collaborative frameworks that integrate academic research, industry expertise, patient advocacy, and regulatory oversight— ensuring that innovative therapies can reach patients while maintaining the highest standards of safety and efficacy.
Clinical Applications
? Immunomodulation:
Through the cholinergic anti-inflammatory route, vagus nerve stimulation has been demonstrated to inhibit the release of pro-inflammatory cytokines[12]. Clinical trials for Crohn's disease and rheumatoid arthritis show decreased drug reliance and disease activity[13].
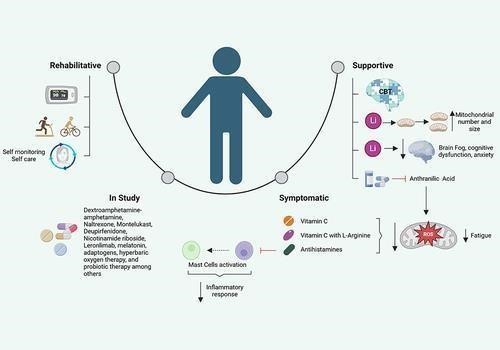
Fig.4 Clinical Applications
For severe Parkinson's disease, DBS is still the gold standard, but responsive neurostimulation gives refractory epilepsy fresh hope[14]. Obsessive-compulsive disorder and treatment-resistant depression are examples of psychiatric applications[15].
? Cardiology and Metabolism:
Through the modulation of autonomic nervous system activity, BEM therapies are being developed for heart failure, arrhythmias, hypertension, and possibly diabetes[16].
Peripheral nerve stimulation promotes functional recovery in stroke and spinal cord injury patients, while spinal cord stimulation relieves pain without the need of opioids[17].
Emerging Areas
Devices that monitor cerebral activity in real time can be used as diagnostic tools, detecting arrhythmias, anticipating seizures, or spotting flare-ups of inflammation before symptoms appear[18].
To target certain nerve branches that govern organs such as the kidneys, pancreas, or spleen, researchers are creating "electroceuticals"[19].
Ultra-thin, flexible electronics are replacing stiff implants, which decrease foreign body response and increase device longevity[20].
Challenges And Future Directions
ADVANTAGES
DISADVANTAGES
CONCLUSION
Healthcare is being redefined by bioelectronic medicine, which combines the intricacy of biology with the accuracy of electronics. Personalised, flexible, and reversible therapies that address underlying pathophysiology in addition to symptoms hold promise. As the field develops, its incorporation into routine clinical practice will depend on the integration of deep circuit mapping, flexible materials, and artificial intelligence.
REFERENCES





Radhakrishnan Ramesh*, Omprakash Ariyan, Senthil Kumar Krishnan, Kannabirran Vaikundam, Gnanasekar Natarajan, Bioelectronic Medicine - Engineering the Body’s Electrical Language for Health, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1490-1497. https://doi.org/10.5281/zenodo.16869157
 10.5281/zenodo.16869157
10.5281/zenodo.16869157
