1Department of Industrial Pharmacy, Bharat Technology, Jadurberia, Uluberia, Howrah, West Bengal-711316.
2Department of Pharmacology, JIS University
3Department of Pharmaceutices, JIS University
In this essay; I have discussed the various factors relating to breast cancer and the factors that cause it. According to the analysis, it emerged that over the past forty years breast cancer has been and still is one of the most common and fatal disease affecting women. This problem affects the social, mental, and physical aspects of a woman’s life. Nevertheless, related aspects like family and friends' support during the sickness can mitigate it. Despite the uncertainty surrounding its specific aetiology, researchers have linked threat factors to breast cancer. Threat factors for breast cancer include age, a family history of the disease, particular changes to one or both breasts, genetic changes, menopausal and productivity histories, lack of physical activity, alcohol use, rotundity, nutrition, race, and radiation treatment to the chest.
Breast cancer is one of the types of cancer that occur in the breast but affect the breast tissue only. It occurs when abnormal breast cells grow and spread outward at a rapid rate in a disorderly fashion and form a tumor. Breast cancer has been the common cancer among women to be diagnosed, and it is the second most common killer disease in women all over the world. The secretions are external to the pectoralis major muscle and are pliable mated glands of which some organs differ in size and consistency. Lobules contain milk-producing cells; several lobules are combined to form lobes containing dispersed fat. Acini forms milk and other surreptitious fluids, they are squeezed through lactiferous ducts and oozed out of the nipple. Cooper suspensory ligaments attach the gland to the sheath of the supporting muscles and sustain the breast. Breast cancer could also develop in the lobules, but the most regular kind of it originates in the ductal epithelium (ductal melanoma). A variety of factors that increase the risk of breast cancer have been described above in detail. Most breast tumors in Western countries have been successfully connected through webbing as opposed to symptoms thanks to webbing programs. But breast lump or irregular nipple discharge may present the first sign in many poor countries most of the time. Owel vivisection, physical examination, and breast imaging are the methods used in diagnosing breast cancer. The common treatment methods available include surgery, chemotherapy, radiation therapy, and hormone therapy; immunotherapy is relatively new to the list. Specific treatment advices are abbreviated depending on the correspondence of histology, cytoarchitectonics, labelling of excrescence, and heritable abnormalities. There are various breast regions where breast cancer might develop, including the Ducts (malignant ducts), Lobular carcinoma or lobules and Sarcoma, or connective tissue respectively.
Paget’s disease begins with the invasion of the skin over the chest wall but is secondary to ductal carcinomas that originate in the milk ducts and are most common.
Classification-
Breast cancer may be classified using various parameters, which include the molecular and biochemical nature of the disease, its histological features, and the anatomical site of origin. This is an excellent presentation of the method of breast cancer staging.
Invasive Breast Cancer - Invasive breast cancer is defined as breast cancer that has progressed into the surrounding tissue from its original location within the breast's ducts or lobules. In contrast to non-invasive breast cancer, which does not spread, breast cancer invasion occurs when cancer cells infiltrate the surrounding tissues and may spread to other organs.
Invasive Ductal Carcinoma (IDC): This type of breast cancer is the most common. IDC starts in the breast ducts and spreads throughout the surrounding tissue. If left untreated, it can also spread to other organs and lymph nodes.
Invasive Lobular Carcinoma (ILC): Invasive Lobular Carcinoma, or ILC, starts in milk-producing units known as lobules and invades the surrounding tissues. ILC compared with IDC typically manifests growth in a different architectural arrangement, which at times may pose diagnostic challenges on mammography.
Non-Invasive Breast Cancer - Sometimes breast cancer has not extended to the surrounding tissue from the ducts and/or lobules of the breast; then the cancer is known as non-invasive breast cancer. There are various types of non-invasive breast cancer, of which DCIS is the most frequent; the cancer cells remain within the ducts in the breast and have not invaded the tissues surrounding them. Another is called lobular carcinoma in situ (LCIS), which is not a real breast cancer per se but increases the risk for subsequent breast cancer.
Non-invasive breast cancers are generally detectable by mammography or biopsies and are usually treated by surgery, radiation therapy, and hormone therapy in order to prevent the non-invasive breast cancer from turning into invasive cancer. For non-invasive breast cancer treatment, the expected outcome is quite favourable, especially in instances where the condition is diagnosed in infancy.
Ductal Carcinoma In Situ (DCIS): It says it to have ducts which are filled with cancer cells though these cells have not infiltrated the surrounding tissue. It is considered as a forerunner of cancer.
Lobular Carcinoma In Situ (LCIS): The lobules contain abnormal cells, but they haven't spread to the nearby tissues. It is regarded as a sign of elevated risk rather than a confirmed case of cancer.
Histological Classification –
Invasive Ductal Carcinoma (IDC) The most prevalent kind, IDC, begins in the milk ducts and spreads to surrounding tissues.
Luminal A - Progesterone receptor-positive (PR+), estrogen receptor-positive (ER+), and HER2-negative cells make up luminal A. has a better prognosis in general.
Luminal B- ER+ and/or PR+, but HER2-positive or higher grade. It may be more aggressive than Luminal A.
HER2-Positive: HER2 protein overexpression is a defining feature. Although it often exhibits greater aggression, targeted therapies can significantly enhance its outcomes.
Triple-negative: It does not have HER2, PR, or ER receptors. It means there are fewer opportunities for individual approaches, and it is often more intensive. Lobular Carcinoma
Invasive (ILC): is less frequent than IDC; it might have a different pattern than IDC and often presents with aberrant, minute nodules that are not technically palpable.
Other types -
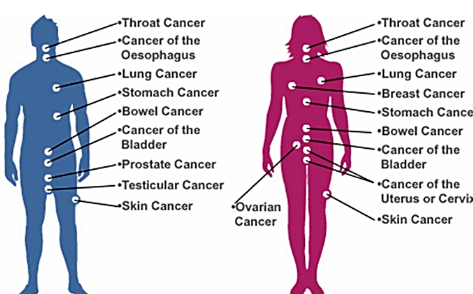
Fig 1 - Types Of Cancer
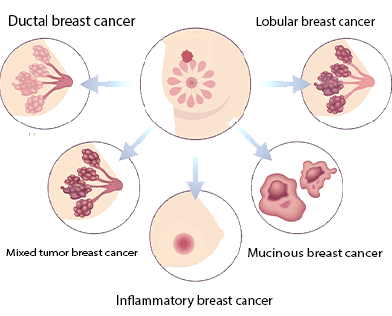
Fig 2- Types Of Breast Cancer
Molecular Classification
Hormone Receptor Status - Estrogen Receptor-Positive (ER+): Estrogen receptors are present in cancer cells and can promote the formation of tumors.
Estrogen Receptor-Positive (ER+): Estrogen receptors, which are present in cancer cells, can promote tumor formation.
Progesterone Receptor-Positive (PR+): Cancer cells have receptors for progesterone.
Hormone Receptor-Negative (ER-/PR-): Since these receptors are not found in cancer cells, the cells often behave differently when receiving treatment.
HER2 Status
HER2-Positive: Cancer cells produce more of the HER2 protein that stimulates the growth of cells. Medicines like trastuzumab (Herceptin) are applied.
HER2-negative: Non-small lung cancer cells do not overexpress HER2, and there are other therapies used.
Genetic and Molecular Subtypes-
(i)Luminal A and Luminal B: Determined by HER2 status and hormone receptor positivity.
(ii)HER2-Enriched: defined by elevated HER2 expression levels.
(iii)Base-like: Frequently triple-negative, these cells resemble breast basal cells and are typically linked to more aggressive behaviour.
4. Staging
Stage 0: Carcinoma in situ, where cancer cells are present but have not invaded surrounding tissues.
Stage I: Small invasive cancer, localized to the breast.
Stage II: Larger tumors or cancer that has spread to nearby lymph nodes.
Stage III: Locally advanced cancer that has spread to nearby tissues or lymph nodes.
Stage IV: Metastatic cancer that has spread to distant organs or tissues.
Symptoms Changes in the Nipple. Enlarged appearance Signs and symptoms of breast cancer may include: Breast nodularity, or an abnormal thickening of the breast that feels distinctly in texture to the remaining tissue. Breasts that are shaped like a table or inverted. Skin color of the breast remains unchanged. For people with a white complexion, the skin on the chest may even appear rather pink or red. In people with brown and black skin, the skin of the breast area may be darker than the rest of the skin, red or purple. The size, form, or shape of the breast differ. Presentation as lumps that are hard and have irregular margins; Nipple retraction; skin ulceration; skin irritation or inflammation; skin that has become thin, itchy, red, or swollen; swelling of the axillary or internal mammary lymph nodes.
Causes
While it is not clear what exactly triggers breast cancer, the disease is believed to develop from genetic mutations in breast cells that make them divide uncontrollably. These mutations could be caused by a number of factors:
1. Genetic Factor-
Gene mutations inherited: Certain women are predisposed to breast cancer due to inherited mutations in particular genes. The most well-known of these are BRCA1 and BRCA2 gene mutations, which dramatically raise the risk of ovarian and breast cancer. These genes aid in the repair of damaged DNA and, in the event that repair is not possible, aid in the death of cells. On the other hand, mutations in these genes cause DNA damage to mount up and result in malignant growths.
That is why, other inherited mutations include TP53, PALB2, CHEK2, and PTEN causing high risk of BC as well, although less common than BRCA ones. Special care should be taken for women who carry gene mutations that increase their risk of breast cancer in their families, especially first-degree relatives.
Family History- Breast cancer risk can be heightened even by having a family history of the disease without molecular alterations identified. A woman, for instance, is twice likely to get breast cancer if one or both of her close members of the family have had the disease.
2. Hormonal Factors-
Exposure to Hormones: The two primary female hormones, progesterone and estrogen, are crucial for breast development and function, but they may also hasten the growth of some breast cancer cells. Multiple factors are associated with an increased risk of breast cancer associated with lifetime exposure to estrogen:
Early menstruation (before the age of twelve): A lifetime of higher estrogen exposure raises the risk of breast cancer. Prolonged exposure to progesterone and estrogen also increases the risk in late menopause (beyond age 55).
Hormone Replacement Therapy (HRT): After menopause, women who receive combination estrogen and progesterone therapy are more likely to develop breast cancer, particularly if they use it for an extended period of time.
Reproductive History:
Breastfeeding and pregnancy may influence a woman's risk of breast cancer. A slightly greater risk of breast cancer exists for women who either have no children at all or have their first child after the age of thirty. On the other hand, nursing, particularly for prolonged periods of time, can somewhat mitigate the risk since it lessens a woman's overall exposure to estrogen by reducing the number of menstrual cycles she goes through.
3. Environmental and Lifestyle Factors-
(i) Obesity and Weight Gain: After menopause, the body uses adipose tissue as its main source of estrogens. Fat cells make more estrogens than other cells, increasing the risk for breast cancer if you're overweight or obese, especially after menopause. Additionally, obesity ties to higher insulin levels, a hormone that’s associated with some cancers.
(ii) Alcohol Consumption: Drinking alcohol might cause the body to produce more estrogen, which may increase the risk of breast cancer. According to studies, women who drink alcohol are more likely to develop breast cancer, and the risk rises with use. In comparison to women who abstain from alcohol entirely, even moderate drinking—one drink per day—can increase risk.
(iii) Absence of Physical Activity: Experts say that women who are physically active usually have a smaller chance of breast cancer development. It is also good for maintaining a healthy weight. Exercising may also lower your breast cancer risk by lowering your estrogen levels, boosting your immune system, and lowering insulin levels.
(iv) Radiation Exposure: Women who have had radiation exposure, especially in the chest region, are more likely to get breast cancer. Since breast tissue is still forming during childhood and adolescence, exposure during these years increases the risk significantly. This exposure includes radiation therapy for other tumors, including Hodgkin's lymphoma.
4. Others risk factors
(i) Age: The risk for breast cancer increases as women age. Most women are diagnosed over age 50, and risk rises with age.
(ii) Gender: Although males can also develop breast cancer, women are far more likely to do so than men. The reason behind the disparity is hormonal levels, with levels of estrogen falling especially low in men.
(iii) Dense Breast Tissue: Select factors increase a woman’s risk of breast cancer, including densities (this is the degree that the breast tissue is made up of glandular and fibrous tissues as compared to the fat tissues in the body). Dense breast tissue also increases the likelihood that mammograms won't detect the cancer.
(iv) Chemical Exposure: Some chemicals in the environment and in products such as plastics, such as bisphenol A (BPA), can act like estrogen and raise breast cancer risk. More research is needed to be certain that chemical exposure and breast cancer are in fact linked.
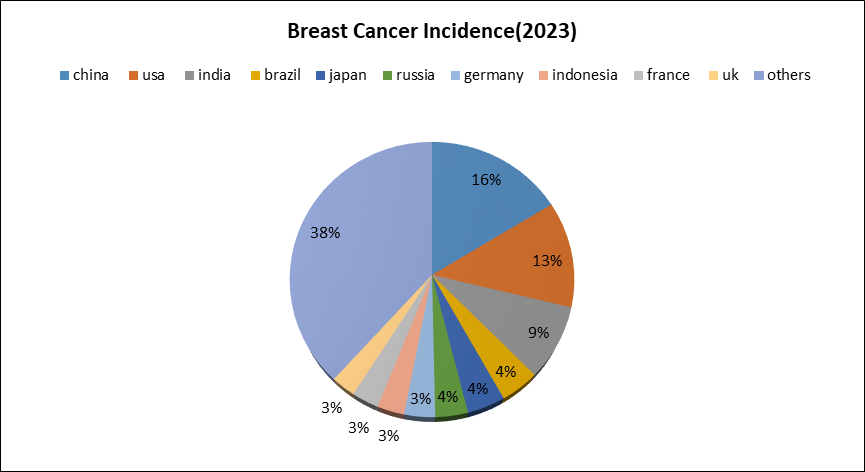
(fig3- Global Breast Cancer Incidence by Country 2023)
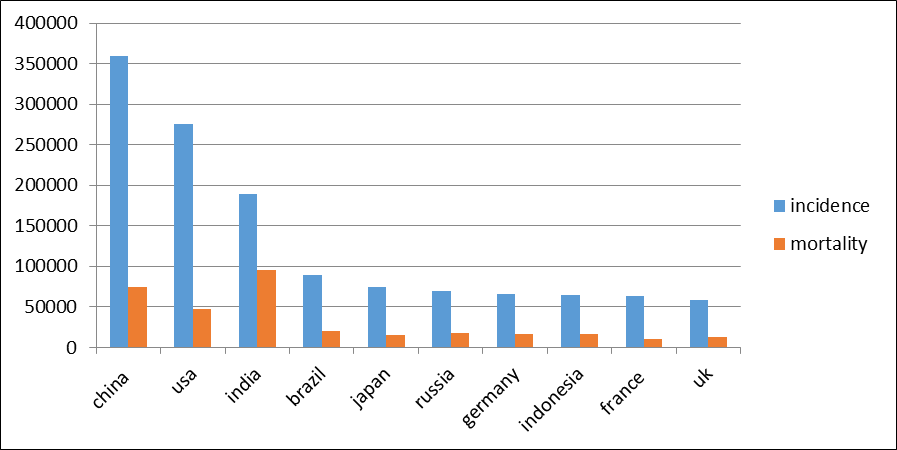
(fig5- Breast Cancer Incidence and Mortality by Country 2023)
Etiology- In the development of breast cancer, genetic, hormonal, environmental, and lifestyle factors are possible factors. Genetic factors: Other genes such as BRCA1 and BRCA2 almost triple the chances of developing breast cancer. Other factors, such as other gene changes and family history, could also contribute.
Hormonal factors: Therefore, progesterone and estrogen control the growth of breast cancer. Early commencement of menstruation, late onset of menopause, and early use of hormone replacement therapy are specific lifestyle variables that raise the risk.
Lifestyle Factors: Breast cancer risk is associated with alcohol consumption, physical activity, diet, and obesity. It could also be associated with smoking and some environmental toxics.
Risk Factors - Another factor believed to increase the risks of breast cancer is described as high breast density. Breast density might add to the risk of breast cancer in women as compared to those women who have less breast density.
Evaluation of Breast Density Factor Risk: Conventionally, one of the four levels of glandularity is defined during a mammography. By knowing levels of density among women, doctors can be in a better position to decide whether or not to recommend use of other imaging or screening techniques such as MRIs or ultrasounds on women, particularly those with thick breasts.
Menopause hormone treatment Breast cancer risk may rise if menopause symptoms are managed with certain hormone therapy drugs. The mix of progesterone and estrogen used in hormone replacement therapy is the cause of this issue. The risk can be decreased by quitting these drugs. Breast cancer is a risk factor for those who are overweight. Radiation exposure. You are more likely to have breast cancer if you were exposed to radiation to the breast as an adult or kid.
Geographic and Ethnic Variations
Geographic Variations: There are notable regional differences in incidence rates. Higher incidence rates are typically reported in high-income nations, most likely as a result of improved detection and lifestyle variables. Conversely, countries with lower incomes tend to record lower rates, but because they may have fewer access to screening and treatment, they may also have greater mortality (Ferlay et al., 2020).
Ethnic Variations: The prevalence of breast cancer varies by ethnicity. For example, although having a somewhat lower incidence rate, African American women in the United States had a higher fatality rate than White women. When compared to Western populations, Asian women often have lower incidence and fatality rates (American Cancer Society, 2021).
Screening and Early Detection
Mammography: Studies have shown that through diagnosis at the pre-advanced state that screening mammography reduces the mortality rate of the disease (Saslow et al., 2007).
Genetic Testing: Genetic testing can yield important information for early intervention methods for women with a family history or other risk factors (Kuchenbaecker et al., 2017).
Survival Rates: Thanks to developments in tailored medicines, early identification, and treatment alternatives, survival rates have increased throughout the years. In high-income nations, the 5-year survival rate for women with breast cancer is approximately 90% (Cancer Research UK, 2021).
Treatment and management
1. Surgery
(i) Lumpectomy: More commonly known as lumpectomy, this procedure involves removal of the tumor, and a rim of macroscopically normal tissue around it. Radiation therapy is often given after it to ensure all remnants of cancer cells are cleared out (Early Breast Cancer Trialists’ Collaborative Group, 2011).
(ii) Mastectomy: This entails the partial or whole removal of one or both breasts. Different forms of mastectomy exist, including skin-sparing or nipple-sparing mastectomy, modified radical mastectomy, and total mastectomy. The decision is based on the cancer's location, size, and stage (Fisher et al., 2002).
2. Radiation Therapy
(i) External Beam Radiation: There are two broad categories of radiation, which differ in the way they are delivered to the body: external beam radiation and internal radiation therapy Other parts of the body affected include the breast and the chest wall, and sometimes the axillary or under arm area in an attempt to eliminate cancer cells (Smith, 2008).
(ii) Brachytherapy: This means placing of a radioactive source within or near the tumor. However, for some people who have undergone lumpectomy, it can be a replacement for external beam radiation (Kauer-Dorner et al., 2020).
3. Chemotherapy
It is used therefore, depending on the stage of cancer and features of the cancer cells, to annihilate those cells that are dividing with remarkable speed. Chemotherapy can also be given before surgery (neoadjuvant), with the aim of shrinking the tumor and making its removal easier, or can be given after the surgery (adjuvant) in order to eliminate possible cancer cells remaining in the body and reduce the risk of their further growth. In later stages of the disease, treatment through chemotherapy is also possible to manage this disease. Adriamycin, cyclophosphamide, Taxol, and Taxotere are some of the chemotherapeutic drugs used in the treatment of cancer; they are used in cycles with breaks in between to exempt the patient’s body. However, there are supportive treatments that may help manage these side effects. Major negative outcomes of chemotherapy include opportunities like nausea, hair loss, exhaustion, and susceptibility to infections.
4. Hormone Therapy ( Endocrine Therapy)
This happens if your cancer has putative receptors to hormones; thus, endocrine therapy, also known as hormone therapy, is used. The aromatase inhibitors and tamoxifen testosterone level inhibitors prevent the impact of estrogen on the breast cancer cells. Menstruating women should also consider the option of ovarian suppression in the premenopausal phase.
5. Targeted Therapy
Targeted therapies are designed to specifically attack molecular characteristics associated with cancer growth.
Drugs such as trastuzumab (Herceptin), pertuzumab, and ado-trastuzumab emtansine target the HER2 protein, which fuels the growth of HER2-positive breast cancer.
Often combined with chemotherapy for better outcomes.
Additional Considerations
Genetic testing: Determining mutations (such as BRCA1/BRCA2) may help inform treatment decisions and family member preventive measures.
Lifestyle and Supportive Care: For general well-being, controlling side effects, eating a balanced diet, getting regular exercise, and receiving psychological support are essential.
Palliative Care: Treatments targeted at delaying the course of advanced cancer are given priority along with symptom management and enhancements to quality of life.
Typically, the treatment plan is customized depending on the unique features of the cancer as well as the health of the patient; multi disciplinary teams collaborate to guarantee the best results.
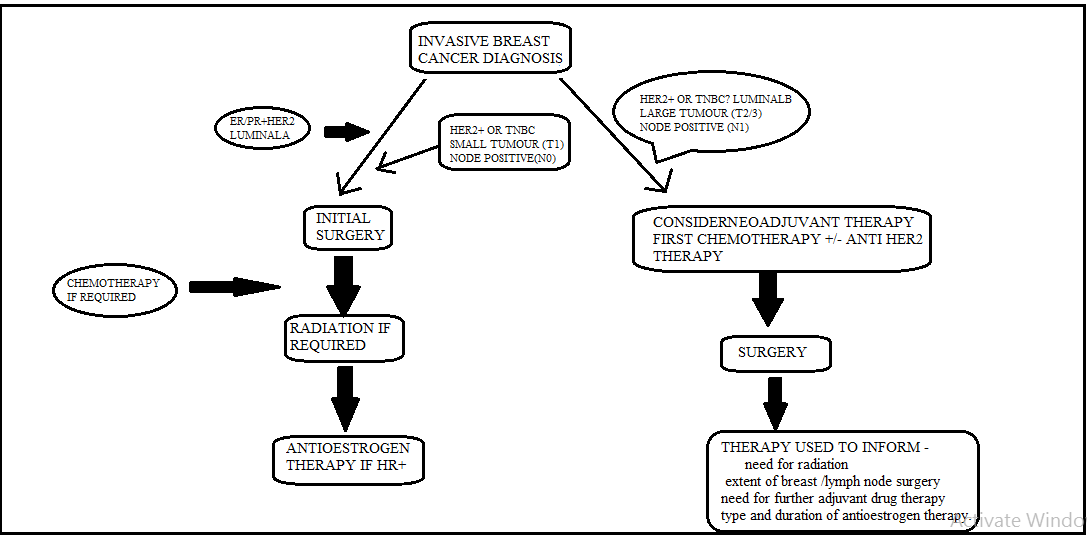
Flow Chart Of The Breast Cancer Treatment

Breast Cancer Treatment Sequencing Algorithm
CONCLUSION
This research aims to gather and improve the current understanding of breast cancer, with a focus on the disease's epidemiology, risk factors, classification, prognostic biomarkers, and available treatment choices. Significant increases in breast cancer morbidity and mortality rates over the past few decades underscore the urgent need for more potent preventative measures, especially those that target modifiable risk factors. The most widely used screening tests at the moment are sonography and mammography, which allow for the early diagnosis of breast cancer. The ongoing quest for prognostic markers and potential biological therapy targets has significantly improved the treatment and clinical outcomes for patients with breast cancer.
REFERENCES



Adarsha Ganguly, Debapriya Dey, Debarghya Karforma, Hirak Bhowmik, A Fundamental Understanding of Breast Cancer & Treatment of Breast Cancer, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 437-447. https://doi.org/10.5281/zenodo.14992139
 10.5281/zenodo.14992139
10.5281/zenodo.14992139
