Bapatla College of Pharmacy, Bapatla.
Cancer incidence increases significantly with advancing age, making chemotherapy a commonly used treatment modality in elderly patients. However, the effectiveness of chemotherapy in older adults is often limited due to factors that extend beyond tumour biology alone. Ageing is associated with complex physiological, pharmacokinetic, pharmacodynamic, and immunological changes that influence drug response, tolerance, and therapeutic outcomes. Declining organ function, altered drug metabolism and elimination, increased susceptibility to toxicity, and the presence of comorbidities contribute to variability in treatment response. Additionally, age-related modifications in tumour biology, DNA repair mechanisms, drug resistance pathways, and the tumour microenvironment further reduce chemotherapy efficacy. Clinical factors such as frailty, polypharmacy, and frequent dose reductions also play a critical role in treatment failure. This review explores the multifactorial reasons behind chemotherapy failure in older adults, emphasising biological, pharmacological, and clinical determinants. Understanding these interconnected mechanisms is essential for optimising chemotherapy strategies, improving safety, and enhancing therapeutic outcomes in the growing elderly cancer population
1.1 Cancer Prevalence in Elderly Patients
Cancer occurs more frequently in elderly individuals due to age-related biological changes and long-term exposure to risk factors [1, 7]. As people live longer, the number of cancer cases among older adults continues to increase, making cancer a major health concern in this population (1, 20).
1.2 Role of Chemotherapy in Cancer Treatment
Chemotherapy is an important method used to treat cancer by destroying rapidly growing cancer cells (3). It is used alone or in combination with surgery and radiotherapy to control tumour growth, reduce symptoms, and improve survival (3, 20).
1.3 Why Chemotherapy Response Differs in Older Adults
Older adults often respond differently to chemotherapy due to reduced organ function, changes in drug metabolism, and lower tolerance to treatment (2, 5, 9).
Ageing brings gradual and natural changes in the structure and function of the human body (7). These changes affect almost all organ systems and influence how the body responds to diseases and medical treatments (5, 9). In elderly individuals, the ability to maintain normal physiological balance declines, increasing vulnerability to illness and altering the response to medications, including chemotherapeutic agents (6,7). Understanding these age-related changes is essential when managing cancer therapy in older patients (6, 8).
2.1 Physiological Changes Associated with Ageing
With increasing age, the body undergoes several physiological modifications such as reduced muscle mass, increased body fat, and decreased cellular repair capacity (7, 9). The immune system becomes less efficient, leading to reduced defence against cancer cells (7). Additionally, bone marrow activity gradually declines, lowering the production of blood cells (9). These physiological changes reduce the body’s ability to tolerate aggressive chemotherapy and influence treatment outcomes in elderly patients (6, 8).
2.2 Reduced Organ Function in Elderly Patients
Ageing is associated with a progressive decline in the functional capacity of major organs. Liver function decreases, resulting in slower drug metabolism (5, 9), while reduced kidney function leads to delayed elimination of drugs and their metabolites (10). Cardiac function may also decline, limiting blood circulation and oxygen delivery to tissues (7). These organ-related changes increase the risk of drug accumulation and toxicity, making chemotherapy management more challenging in elderly patients (6, 9).
2.3 Impact of Ageing on Drug Handling
Age-related physiological and organ function changes significantly affect how drugs are absorbed, distributed, metabolised, and excreted (2, 9). Reduced gastric motility and blood flow can alter drug absorption, while changes in body composition influence drug distribution (9). Slower metabolism and excretion prolong drug action, increasing the risk of adverse effects (5, 10). As a result, elderly patients often require careful dose adjustment and monitoring to achieve safe and effective chemotherapy (6).
3 Basics of Chemotherapy Resistance
Chemotherapy resistance refers to the reduced ability of cancer cells to respond to anticancer drugs that were once effective (3). When resistance develops, chemotherapeutic agents fail to destroy cancer cells adequately, leading to poor treatment outcomes and disease progression [19]. Chemotherapy resistance is a major challenge in cancer therapy and is influenced by tumour-related factors as well as patient-related factors such as age, health status, and drug tolerance [3, 6].
3.1 Meaning of Chemotherapy Resistance
Chemotherapy resistance is the condition in which cancer cells survive and continue to grow despite the administration of chemotherapeutic drugs [3]. This resistance may be present from the beginning of treatment or may develop gradually during therapy. Resistant cancer cells can evade medication action through various biological adaptations, resulting in reduced drug effectiveness and increased chances of cancer recurrence [3, 9].
3.2 Types of Chemotherapy Resistance
Chemotherapy resistance is generally classified into two main types based on the time and manner in which resistance occurs.
3.2.1 Primary (Intrinsic) Resistance
Present before chemotherapy begins.
Tumour cells already possess natural defence mechanisms.
Anticancer drugs fail to act effectively.
No meaningful therapeutic response observed
Leads to early treatment failure [3]
3.2.2 Acquired Resistance
Develops after an initial positive response to chemotherapy
Continuous drug exposure triggers adaptive cellular changes.
Activation of survival and repair pathways
Gradual loss of drug sensitivity
Results in tumour progression or relapse [19]
4 Biological Factors Contributing to Resistance in the Elderly
Biological changes that occur with ageing play an important role in reducing the effectiveness of chemotherapy in elderly cancer patients. As the body ages, both normal and cancerous tissues undergo structural and functional alterations that influence how cancer cells respond to anticancer drugs. These age-related biological factors can limit drug action and promote survival of cancer cells, thereby contributing to chemotherapy resistance in older adults [7, 19].
4.1 Reduced Cell Proliferation in Aged Tissues
Many chemotherapeutic agents act by targeting rapidly dividing cells [3]. In elderly patients, both normal and cancer cells often divide more slowly due to age-related changes in cellular activity. This reduced rate of cell proliferation lowers the sensitivity of cancer cells to chemotherapy, as the drugs are less effective against slowly growing or dormant cells. As a result, treatment outcomes may be less favourable in older individuals [19].
4.2 Altered DNA Damage and Repair Mechanisms
Chemotherapy commonly works by causing damage to the DNA of cancer cells, leading to cell death. In elderly patients, cancer cells may develop changes in their DNA damage response systems that allow them to tolerate or repair this damage more effectively. At the same time, ageing can disrupt normal DNA repair balance, enabling cancer cells to survive despite drug-induced damage. These alterations reduce the ability of chemotherapy to eliminate cancer cells completely [3, 19].
4.3 Increased Drug Efflux from Cancer Cells
Another important factor contributing to chemotherapy resistance in the elderly is the increased ability of cancer cells to expel anticancer drugs. Cancer cells may express higher levels of drug transport proteins that actively pump chemotherapy agents out of the cell. This process lowers the concentration of the drug inside the cancer cells, reducing its effectiveness and allowing the cells to survive treatment [3, 11].
5 Tumour Microenvironment and Ageing
The tumour microenvironment refers to the surrounding tissues, blood vessels, immune cells, and signalling substances that support tumour growth. In elderly patients, ageing-related changes in the body significantly alter this microenvironment. These changes can reduce the effectiveness of chemotherapy by protecting cancer cells and limiting drug access to the tumour site. Understanding how ageing affects the tumour microenvironment is important for improving treatment outcomes in older cancer patients [19].
5.1 Chronic Inflammation in Elderly Patients
Ageing is often associated with a long-lasting, low-grade inflammatory state. In elderly patients, this persistent inflammation creates a favourable environment for cancer cells to survive and grow. Inflammatory substances released in the tumour surroundings can reduce the sensitivity of cancer cells to chemotherapy and promote resistance. This chronic inflammatory condition also interferes with the body’s ability to eliminate damaged or abnormal cells effectively [7, 19].
5.2 Reduced Blood Supply to Tumours
With advancing age, blood vessel function gradually declines, leading to reduced blood flow in many tissues, including tumours. Poor blood supply limits the delivery of chemotherapeutic drugs to the tumour site. As a result, cancer cells may receive lower drug concentrations than required for effective treatment, allowing them to survive and develop resistance [19].
5.3 Effect of Tissue Changes on Drug Penetration
Ageing causes structural changes in tissues, such as increased stiffness and fibrosis. These changes make it more difficult for chemotherapy drugs to penetrate deep into the tumour mass. Limited drug penetration results in uneven drug distribution within the tumour, leaving some cancer cells untreated. Over time, these surviving cells contribute to chemotherapy resistance and disease progression [19].
6. Pharmacokinetic Changes in Elderly Patients
Pharmacokinetics describes how the body absorbs, distributes, metabolises, and eliminates drugs. In elderly patients, normal ageing leads to gradual changes in these processes, which can significantly affect the behaviour of chemotherapeutic agents. These changes may result in altered drug levels, increased toxicity, or reduced treatment effectiveness, making chemotherapy management more complex in older adults [2, 9].
6.1 Absorption of Chemotherapeutic Drugs
Ageing can influence drug absorption due to reduced gastric acid secretion, slower stomach emptying, and decreased blood flow to the gastrointestinal tract. Although the extent of absorption may not change greatly for all drugs, the rate at which chemotherapeutic agents enter the bloodstream can be slower in elderly patients. This delay may affect the onset of drug action and contribute to variability in treatment response [2].
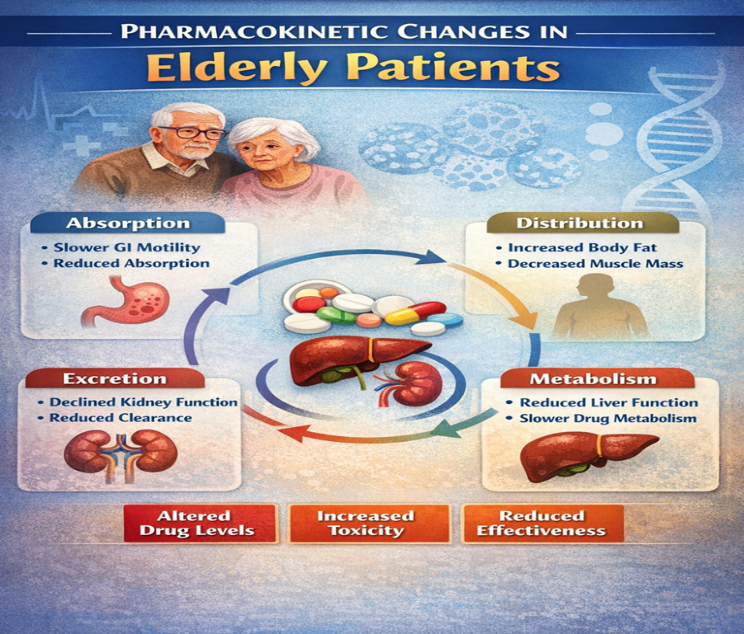
Fig 1 Pharmacokinetic Changes in Elderly Patients
6.2 Distribution Changes Due to Body Composition
With increasing age, body composition undergoes noticeable changes, including increased fat mass and reduced muscle and water content. These changes affect how drugs are distributed within the body. Lipid-soluble chemotherapeutic drugs may accumulate in fat tissues, while water-soluble drugs may reach higher concentrations in the blood. Such distribution changes can alter drug effectiveness and increase the risk of adverse effects [9].
6.3 Reduced Metabolism in the Liver
Liver size and blood flow tend to decrease with age, leading to reduced metabolic capacity. As a result, chemotherapeutic drugs that are metabolised in the liver may be broken down more slowly in elderly patients. This slower metabolism can cause drugs to remain in the body for longer periods, increasing the likelihood of toxicity and requiring careful dose adjustment [5, 9].
6.4 Decreased Renal Excretion
Kidney function gradually declines with ageing, resulting in reduced elimination of drugs and their metabolites. Chemotherapeutic agents that are primarily excreted through the kidneys may accumulate in elderly patients if doses are not adjusted appropriately. Reduced renal excretion increases the risk of adverse drug reactions and highlights the importance of regular kidney function monitoring during chemotherapy [10].
7 Pharmacodynamic Changes
Pharmacodynamics refers to how drugs interact with their targets in the body to produce a therapeutic effect. In elderly patients, age-related changes at the cellular and molecular level can reduce the effectiveness of chemotherapeutic drugs. These changes are different from pharmacokinetics, as they affect drug response at the target site rather than drug movement in the body [9].
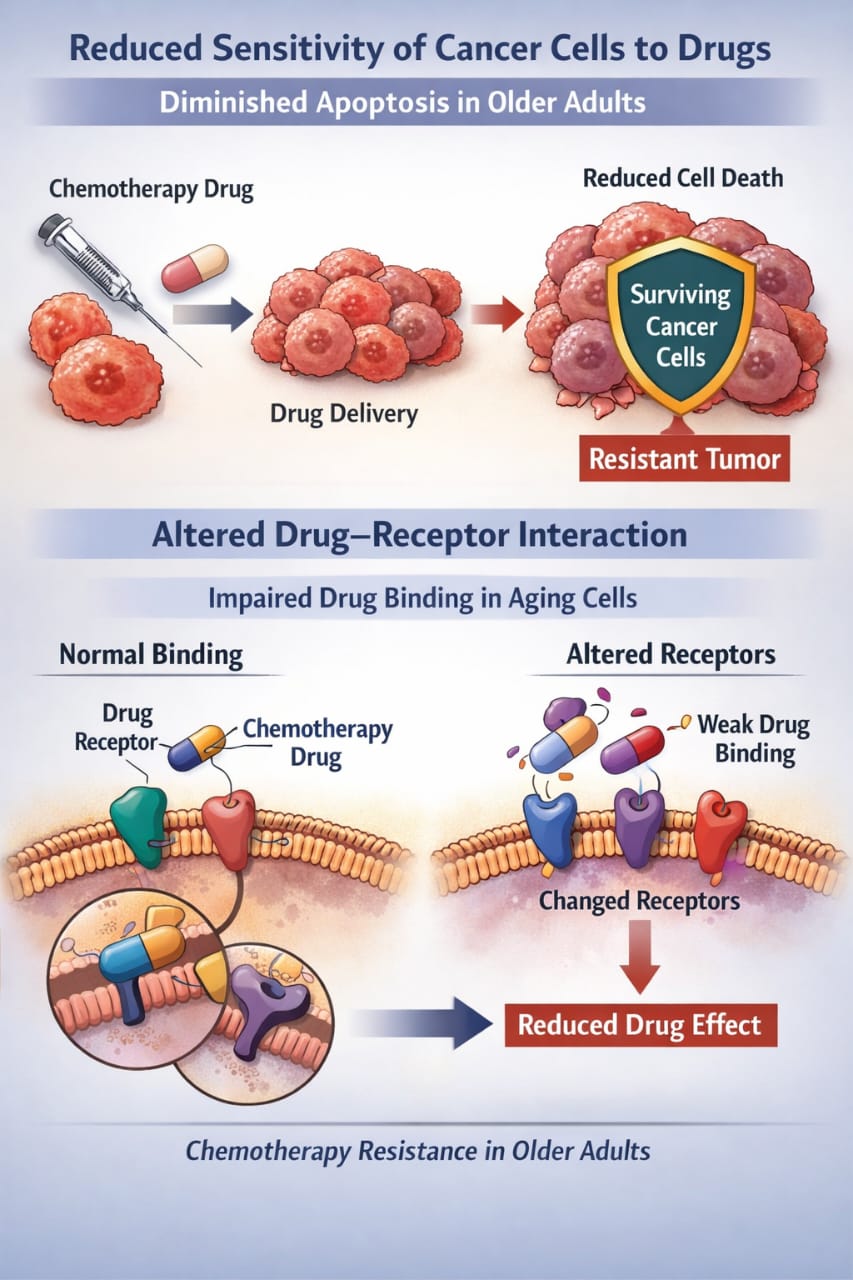
Fig 2 shows Chemotherapy Resistance in Older Adults
7.1 Reduced Sensitivity of Cancer Cells to Drugs
In older adults, cancer cells may become less responsive to chemotherapy due to changes in cellular mechanisms that control growth and death. For example, the ability of drugs to trigger cell death (apoptosis) may be diminished. As a result, even when the drug reaches the tumour in adequate amounts, its effect on killing cancer cells is reduced, contributing to chemotherapy resistance [3].
7.2 Altered Drug–Receptor Interaction
The effectiveness of many chemotherapeutic drugs depends on their interaction with specific receptors or enzymes in cancer cells. Ageing can lead to changes in these receptors or signalling pathways, which may reduce drug binding or interfere with the intended cellular response. Consequently, the drug may not work as efficiently, and higher doses or alternative therapies may be required for effective treatment [9].
8 Clinical Factors Affecting Chemotherapy in the Elderly
Several clinical factors unique to elderly patients can influence the effectiveness and safety of chemotherapy. These factors are often linked to the overall health status, medical history, and treatment tolerance of older adults, and they play a key role in determining treatment outcomes.
8.1 Frailty and Poor Tolerance to Chemotherapy
Frailty is a common condition in older adults characterised by decreased strength, stamina, and physiological reserve. Frail patients may struggle to tolerate standard chemotherapy doses, leading to increased side effects such as fatigue, infections, and organ toxicity. Poor tolerance often limits the intensity of treatment and may reduce its overall effectiveness [6, 8].
8.2 Presence of Multiple Diseases (Comorbidities)
Elderly patients often have additional health conditions such as diabetes, hypertension, or heart disease. These comorbidities complicate chemotherapy treatment because they may worsen drug toxicity or limit the choice of drugs. The presence of multiple diseases can also interfere with the patient’s overall ability to recover from chemotherapy-related side effects [7].
8.3 Polypharmacy and Drug Interactions
Many older adults take multiple medications for various health conditions, a situation known as polypharmacy. Chemotherapeutic drugs can interact with these medications, leading to reduced drug effectiveness, unexpected side effects, or increased toxicity. Careful evaluation of all medications is necessary to minimise harmful interactions during cancer treatment [13-17].
8.4 Dose Reduction and Treatment Discontinuation
Due to frailty, comorbidities, or toxicity, chemotherapy doses are often reduced, or treatment schedules are altered in elderly patients. In some cases, therapy may need to be temporarily or permanently discontinued. While these adjustments improve patient safety, they can also reduce the therapeutic effect of chemotherapy and contribute to resistance or disease progression [6, 8].
9 Chemotherapy-Induced Toxicity in Elderly Patients
Chemotherapy is designed to kill rapidly dividing cancer cells, but it can also affect healthy tissues, leading to toxicity. In elderly patients, age-related physiological changes make them more susceptible to side effects. Toxicities can limit treatment tolerance, require dose adjustments, or even lead to treatment discontinuation, reducing overall chemotherapy effectiveness [4, 9].
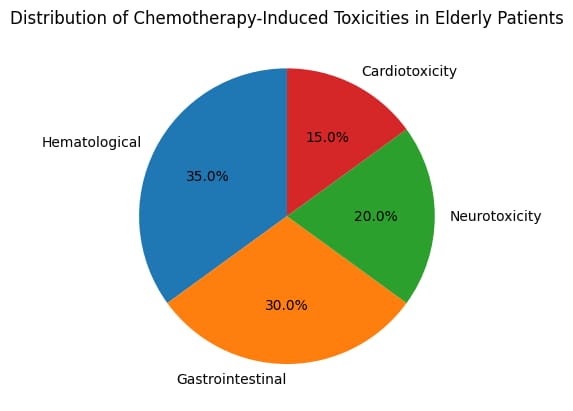
Fig 3 shows the distribution percentages of chemotherapy-induced toxicities in elderly patient
9.1 Haematological Toxicity
Haematological toxicity affects the blood-forming cells in the bone marrow, resulting in lower production of red blood cells, white blood cells, and platelets. This can cause anaemia, increased risk of infections, and bleeding tendencies. Elderly patients are particularly vulnerable because bone marrow function naturally declines with age, making them more prone to severe blood-related side effects [9].
9.2 Gastrointestinal Toxicity
Chemotherapy can irritate the lining of the digestive tract, causing nausea, vomiting, diarrhoea, loss of appetite, and mucositis. In older adults, reduced gastrointestinal motility and decreased repair capacity increase the severity of these symptoms. Poor nutrition and dehydration from gastrointestinal side effects can further compromise treatment outcomes [3].
9.3 Neurotoxicity
Certain chemotherapeutic drugs can damage nerves, leading to peripheral neuropathy, cognitive changes, or “chemo brain.” Elderly patients may experience heightened sensitivity to neurotoxic effects due to age-related changes in the nervous system. Symptoms such as numbness, tingling, or memory difficulties can reduce quality of life and may necessitate treatment modifications [9].
9.4 Cardiotoxicity
Some chemotherapy agents, particularly anthracyclines and targeted therapies, can impair heart function. Elderly patients are at higher risk of cardiotoxicity because of pre-existing heart conditions or decreased cardiac reserve. Cardiac complications can range from mild arrhythmias to severe heart failure, requiring careful monitoring during treatment [7].
10. Strategies to Improve Chemotherapy Outcomes in the Elderly [6, 8, 13]
Elderly cancer patients often face challenges such as reduced drug tolerance, comorbidities, and age-related physiological changes that affect chemotherapy effectiveness. Implementing specific strategies can help improve treatment outcomes, reduce side effects, and enhance the quality of life for older adults undergoing chemotherapy.
Table 1: Strategies to enhance Chemotherapy Outcomes in Elderly Cancer Patients
|
Strategy |
Key Aspects |
Contributions to Improved Outcomes |
|
Individual Dose Selection
|
Chemotherapy doses are tailored according to age-related physiological changes, organ function, comorbid conditions, and performance status. Continuous assessment through laboratory monitoring and clinical response evaluation guides dose modifications. |
Reduces the risk of severe toxicity while preserving anti-cancer efficacy, thereby improving treatment safety and tolerability in older patients. |
|
Supportive Care and Toxicity Management |
Incorporates proactive measures such as antiemetics, hematopoietic growth factors, pain control, nutritional supplementation, and adequate hydration to manage treatment-related adverse effects. |
Enhances patients' ability to tolerate chemotherapy, minimises complications, and decreases the need for delays or discontinuation. |
|
Rational Use of Combination Therapy |
Selection of drug combinations is based on toxicity profiles, potential interactions, and organ reserve. Strategies such as reduced-dose combinations or sequential drug administration are preferred in frail patients. |
Achieves effective tumour control while limiting cumulative toxicity and preserving functional independence |
|
Role of Pharmacists in Elderly Cancer Care |
Pharmacists assist in dose optimisation, identify and prevent drug-drug interactions, provide patient counselling, and support adherence to therapy and supportive medications. |
Improves medication safety, optimises therapeutic outcomes, and supports individualised treatment planning in geriatric oncology |
11. Current Challenges and Limitations
Managing chemotherapy in elderly patients remains complex due to multiple overlapping factors. Age-related changes, coexisting medical conditions, and individual variability make standard treatment approaches less reliable. Several key challenges currently limit the effectiveness and safety of chemotherapy in older adults.
11.1 Limited Representation of Older Adults in Research
Elderly patients are often underrepresented in clinical trials, which creates a gap in knowledge about optimal drug selection, dosing, and treatment schedules for this age group. Without sufficient trial data specific to older adults, physicians must rely on protocols designed for younger patients, which may not account for the physiological and metabolic differences of ageing [12, 20].
11.2 Difficulty Balancing Effectiveness and Safety
Elderly patients are more vulnerable to drug toxicity due to declining organ function and reduced physiological reserves. Aggressive chemotherapy can control cancer effectively but may lead to severe side effects, while conservative dosing may reduce toxicity but also lower therapeutic benefits. Striking the right balance remains a persistent clinical challenge [6].
11.3 Challenges in Maintaining Consistent Treatment
Frailty, cognitive decline, transportation issues, and complex medication schedules can all affect a patient’s ability to follow the prescribed chemotherapy regimen. Missed doses, delays, or early discontinuation reduce the overall effectiveness of treatment and can contribute to drug resistance or disease progression [8].
11.4 Individual Variability in Drug Response
Each elderly patient responds differently to chemotherapy due to variations in metabolism, drug absorption, and sensitivity of cancer cells. This unpredictability makes it difficult to generalise treatment strategies and emphasises the need for personalised approaches that consider the patient’s health status and functional capacity [2, 9].
CONCLUSION:
Chemotherapy failure in older adults is the result of a complex interaction between ageing-related biological changes, altered drug handling, tumour adaptations, and clinical limitations rather than tumour factors alone. Declining organ function, reduced cellular proliferation, impaired drug metabolism, and increased vulnerability to toxicity significantly influence treatment effectiveness and tolerance in elderly patients. Furthermore, changes in the tumour microenvironment, chronic inflammation, and enhanced drug resistance mechanisms reduce the cytotoxic impact of chemotherapy. Clinical challenges such as frailty, multiple comorbidities, polypharmacy, and frequent treatment modifications further compromise therapeutic outcomes. The underrepresentation of elderly patients in clinical trials continues to limit evidence-based decision-making in geriatric oncology. Addressing these challenges requires a personalised and multidisciplinary approach that integrates geriatric assessment, individualised dosing, supportive care, and careful monitoring. By tailoring chemotherapy strategies to the unique physiological and clinical characteristics of older adults, it is possible to improve treatment tolerability, enhance efficacy, and ultimately achieve better quality of life and survival outcomes for this vulnerable population [1-20].
REFERENCES:
PubMed
Cancer Network
OUP Academic
PubMed
SpringerLink
SpringerLink
SpringerLink
PubMed
Cancer Network
OUP Academic
PubMed
SpringerLink
SpringerLink
SpringerLink





Nadendla Balu1*, Mandru Ramyakumari2, Allu Pavithra3, Talakonda Rajeswari4, Yeluri Chinmayi sri5, Why Chemotherapy Fails in Older Adults: Mechanisms Beyond the Tumour, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 743-753. https://doi.org/10.5281/zenodo.18492506
 10.5281/zenodo.18492506
10.5281/zenodo.18492506
