Fabtech College of Pharmacy Sangola, Solapur, Maharashtra-413307
AA is a long-term, immune-mediated disorder that causes non-scarring alopecia . It usually manifests and abrupt, patchy baldness on the head and other parts of body that bear hair. An immunological attack on hair follicles causes it, usually in people who are genetically predisposed. Although the illness can occur at any year and affects collectively male and female same, it most frequently shows up in childhood or early adulthood. Alopecia areata is characterised by localised patches, while alopecia totalis is characterised by entire scalp or body hair loss. A complicated interaction between immunological dysregulation, environmental stressors, and genetic susceptibility—particularly T-cell-mediated inflammation—makes up the aetiology.
Alopecia areata (AA) is a prevalent, immunological-mediated, Non-scarring alopecia with a clinically varying range. Alopecia totalis or alopecia universalis can influence the entire head or body, or it may just impact one or more prominent, identifiable round or oval regions of loss of hair on your head or skin.[1] Additionally, the course of the condition is unexpected; renewed episodes can occur at any time, and 80% people suffer spontaneously development of hair in the initial year. [2, 3] The subgroups of total hair loss and universalized alopecia have a poor prognosis because,well as aspects such related nail lesions, hair loss that has lasted longer than ten years, and a positive family history. In addition to making it a mental difficulty, AA sufferers are more likely than the general population to experience anxiety and depression. (4)" Research on immune system and genetic factor, specifically in area of dentritics units, is advised for AA because there is poof that DC may be used to treat other autoimmune disorders like cancer and multiple sclerosis. Promising therapies for AA therapy include PRP and JAK-STAT inhibitors. The disorder unclear pathologic mechanisms and variable remission rates make it difficult to implement and assess treatment procedures for AA. [5] Although dermatologic application medications been utilised for Alopecia areate, the effectiveness of these therapies varies greatly, and the therapy should also address the client psychosocial necessary which makes care extra challenging[6 ]
The recommended course of treatment includes corticosteroid therapy. For patients with mild to moderate AA, topical and intralesional corticosteroids are both suitable and efficacious. [7,8]
It is more difficult to treat severe AA conditions such as alopecia universalis, totalis, and ophiasis.[9] In these patients, systemic corticosteroids are typically beneficial and can be given intravenously, orally, or intramuscularly. [10].

Fig.No.1 :Alopecia Aereta in Male and Female
HISTORICAL BACKGROUND :
Alopecia Areata's Historical Context One of the earliest known dermatological conditions is alopecia areata (AA), which has been described for several millennia. There are allusions to AA-like patchy, non-scarring hair loss in ancient Egyptian, Greek, and Roman medical texts. Inspired by the patchy hair loss observed in fox mange, the word alopecia is derived from the Greek word "alopex" (fox). Early Accounts (Ancient to Medieval Period) Hippocrates (5th century BCE) and Galen (2nd century CE) recorded instances of abrupt, confined hair loss that closely resemble contemporary accounts of alopecia areata. Due to similar clinical features, the illness was frequently mistaken for infectious causes in the Middle Ages, particularly tinea capitis.[11]
CLINICLE PRESENTATION :
Alopecia areata can appear clinically in a variety of ways both within and between individuals. Clinically, the illness is divided into multiple variations according on the outer skin layer affected, pattern, and the level of hair loss. Table 1
Table 1. Alopecia areata clinical variations and their distinctive symptoms
|
Clinical variations of alopecia areata |
Feature |
|
Patchy alopecia areata |
Most common type; well-defined,Circular or elliptical areas ,Reduced hair density or other hair-bearing areas. |
|
Alopecia totalis |
Entire scalp hair fall , progression from patchy alopecia. |
|
Alopecia universalis |
Complete Total loss of all body including scalp, eyebrows, eyelashes, beard, and body hair. |
|
Ophiasis alopecia areata |
Linear pattern hair loss along temporal sides and occipital base of the scalp margins (“snake-like” pattern); often resistant to treatment. |
|
Inverse-ophiasis (or sisaipho) alopecia areata |
Opposite of ophiasis; sparing temporal and occipital margins, with hair loss in central/scalp vertex areas. |
|
Diffuse alopecia areata/ Alopecia areata incognita |
Sudden, widespread thinning of scalp hair resembling telogen effluvium; difficult to diagnose without biopsy. |
|
Reticular Alopecia areata |
Net-like or patchy, interconnecting pattern of hair loss. |
|
Marie-Antoinette Syndrome |
Abrupt whitening of hair due to preferential loss of pigmented hair shafts (sparing white hairs). |
A number of localized regions of head hair loss are the hallmark of patchy AA, which is the most prevalent kind of AA (Fig.2a). These irregular regions could be distinct, stand alone, or merge with neighboring lesions to form a larger, hairless area. The skin inside the lesions is smooth, healthy-looking, and intact, despite the rare little edema that is palpable but doesn’t show up as redness or other signs of infection. Based on the activity of the condition, an area may grow in width or stay the same shape. Additionally, it could naturally cure and either entirely or in part regrow. Baldness or alopecia universalis , a form of which is the complete absence of scalp scalp hair, can result from patchy alopecia Areata. May lead to a condition called alopecia totalis , characterized by an overall reduction in head hair, or alopecia universalis , or is a total lack of all body hair (Fig. 2b). These are more clinically types of alopecia areata of the head because it can manifest in various manners.[12]
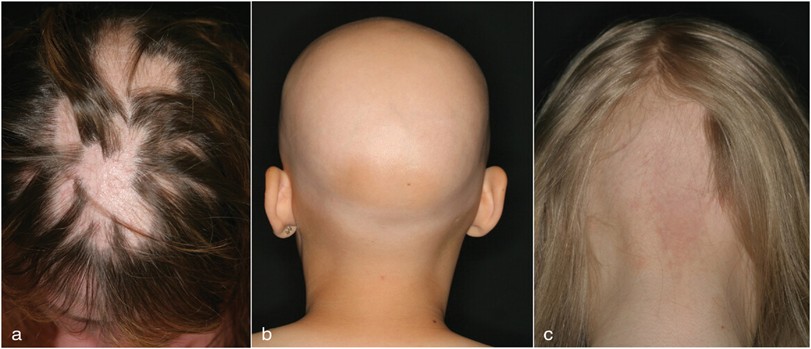
Fig.No:2
The opposite disorder, known as sisaipho or inverse-ophiasis type, is characterised by central hair loss that resembles androgenetic alopecia. One uncommon, Non-localized variant of Alopecia Areata that is frequently Incorrectly diagnosed or has a noticeably delayed diagnosis is diffuse alopecia areata (DAA), also known as alopecia areata incognita (AAI). Women aged 20 to 40 are more likely to suffer from diffuse AA, which is typified by diffuse hair loss [13,14]
EPIDEMIOLOGY :
The second most common reason of hair loss after androgenetic A is AA [15] , affecting 2% of people worldwide, and its frequency is rising. [16] Ophiasis type, alopecia totalis , and alopecia universalis are less common than severe Alopecia Areta symptoms and specific Medical subtypes, with respective prevalences of 0.02%, 0.08 percent, and 0.03%. Both sexes seem to be equally affected by alopecia areata, which can happen to anyone of any age or origin. Compared to adults, young people are more likely to have AA. Additionally, AA is more prevalent among African or African American communities than in Asian and Asian groups, according to recent studies.(17)
Epidemiology : based on sex
The two population studies did not find any discernible variation the occurrence of alopecia areata in both genders [18,19] According to reports, male patients had been identified with AA earlier than female patients.[20] 4 Certain research indicates that there are not statistically reliable variations in duration, or years of AA onset by sex or race.[21]
Epidemiology : based on age
Generally younger age groups have been more likely to be members of AA. The age group that presented for care the most frequently was twenty one–fourty years old, followed by one–twenty years old, fourty one–sixty years old, and 61–80years old.Similarly, the age groups of 31–35 and 30–59 have been found to have the highest rates of AA visits. In 82.6% to 88% of cases, AA patients initially develop the disease by the age of 40, and in 40.2% of cases, it occurs by the age of 20. Table No. shows that the average age at which onset occurs has been found between twenty five. five and thirty six. Three years .Different reports have indicated that the age of onset for females is lower (24.2 vs 26.7 years),the same for males (20),and higher(36.2 vs 31.5 years ).It has been found that the mean year of onset in youngsters is between the years of 5 &10 .[22]
EPIDEMIOLOGY :based on body part
The head is the mainly affected area, either alone or in conjunction with other body parts (such the beard, eyelashes, and eyebrows).[23] In particular, the occipital area was the most frequently affected site, occurring in 33.4% of females and 38.4% of males.[24] 58% of adult patients reported patchy hair loss on initial presentation, affecting less than half of the scalp.[25]
PROGNOSIS :
The illness has an uncertain prognosis. Thirty four% to fifty % of patients recoverd in a year, according to current data, while 14% to 25% of patients advance to AT or AU, where they hardly ever totally recover. Twelve of the seventy patients with AT/AU (17.1%) who had their charts reviewed retrospectively over a ten-year period showed full hair regrowth. Out of seventy patients with alopecia areata, 17 (24.2%) recorded getting at least ninety percent of their hair back. Five patients with AT (20.8%) and thirty with AU (65.2%) did not exhibit any improvement in their hair growth. Patients may experience multiple Period of hair fall followed by regrowth over the activity of their lifetimes. The following factors are linked to bad prognosis: a history of atopy, early year at onset, Nail disorder ,significant hair fall, Occipital–temporal alopecia pattern or the presence of other autoimmune illnesses. [26]
DIAGNOSIS :
The disorder is generally recognized by clinically, and findings like a +ve trichoscopy or Performing a pull test could aid. Active illness is identified on trichoscopy by breaked hairs, "exclamation mark" or thinning hair, dark spots, and yellow spots. Another sign of AA is vellus hair in lesions, which could be an indication of inactive or late illness. A biopsy may be performed in circumstances that are unclear.[27]
HISTOPATHOPHYSIOLOGY :
The disease's histology will change depending on its stage. A peribulbar lymphocytic infiltration in the acute and subacute phases is characterised by a "swarm of bees" pattern of CD4+ and CD8+ T-cells surrounding a growing hair follicle Furthermore, follicle miniaturisation occurs as the hair development stage transitions from the catagen to the telogen (resting) phase. The hair follicles may be surrounded by macrophases, foreign body giant cells, oedema, microvesiculation and apoptosis. In the chronic stage, pigmentary incontinence occurs, the amount of catagen or telogen hair grows, and the inflammation may or may not go away .[28]
PATHOPHYSIOLOGY :
At this time, the precise diseases condition of the illness is unspecified. But there is evidence that Alopecia Areta is brought on by autoimmune response to hair follicles that results from a combination of environmental and hereditary causes.[29]
A unique type of microorgan, the hair follicular (HF) undergoes a continuous, lifelong process of reproduction. The lower part of the good analog HF (the bulk and column) protects the follicle that produces hair from infection and promotes immunity due to its relative immune privilege (IP).[30]
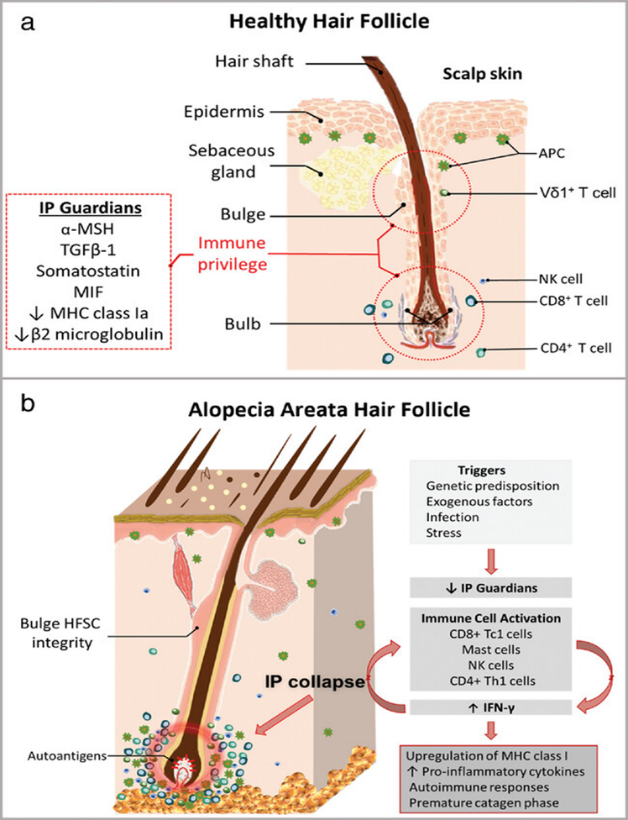
Fig. No.3 : a. Healthy Hair Follicle
b. Alopecia Areata Hair Follicle
REMIDIES
Hair development is promoted by coconut oil, which improves the health of the scalp and hair. There are other nutrients that can help in growth. The oil that is derived from dried coconuts is called coconut oil. It has a white butter-like appearance at room temperature and melts when heated. Hair care, cosmetics, cooking, and food preparation all make great use of this natural oil. Several medical studies have shown the profit of coconut oil for the skin, hair, & body. Some people apply coconut oil to their scalp and hair because they believe it accelerates hair growth. We'll see whether we can accomplish this.
Research on the connection between hair growth and coconut oil is nonexistent. However, coconut oil is beneficial the hair & scalp. As a result, the hair will grow faster.[31,32]

Fig. No. 4: Coconut oil
Hair loss is a major problem among numerous younger girls and women. The hair problem is not brand-new, but it has evolved over the past few years. Fast-paced lifestyles, increased stress levels, and pollution have made hair loss more of a problem. Every day, we hear women and girls talking about hair difficulties in casual conversations and on social media. Thanks to natural medicine, we can be saved! Do you remember your grandmother talking about how her mother used herbs to heal a range of illnesses? Or did your parent tell you about the hair remedies and treatments she tride when she was younger ? Natural hair treatments are always dependable because they have been proven to be easy , efficient , and successful .when use it with the appropriate hair treatment product , you won’t be concerned about hair loss anymore ! Over the year ,individuals have tride , tested , and verified the efficacy of numerous cures , such as dairy products, aloe vera ,and lemon. Because of its benefits and uses ,fenugreek stands out from other hair care products. [33]

Fig. No. 5: Fenugreek seed (Methi)
baldness is a major issue, and practically all women grow weary of keeping track of how much hair they lose each day. Dandruff, balding, thinning hair, and grey hair are just a few of the issues that accompany hair. Naturally, pollution is to blame for this, and regardless of our actions, we are constantly in contact with it. Use heat-resistant cosmetics or wrap our hair in a scarf to protect it. Hair loss is a major issue, and nearly all women grow weary of keeping track of how much hair they lose each day. Dandruff, balding, thinning hair, and grey hair are just a few of the issues that accompany hair.
Naturally, pollution is to fault for this, because we are constantly exposed to it regardless of our actions. Wrap our hair with a headscarf or use heat-resistant cosmetics to protect it.[34,35]

Fig.No. 6 :Onion Oil
4.Amla (Indian Gross Berry)
Five uses for amla in hair treatment :
Reducing Hair Loss with Amla: Consuming amla on a daily basis can make your hair seem amazing. Amla juice is also delicious.
Drinking is recommended for people who experience significant hair loss.
One glass of amla juice on without food each day.[36]
Amlicanemblica Juice Promotes Hair Growth: The straightforward yet potent amla tonic is for you if you're looking for thicker, stronger hair. Gently massage the scalp after applying freshly extracted amla juice. Rinse your hair well with a gentle shampoo after 50 to 60 minutes.[37]
Nourish with Lemon and Amla: It is thought that amla and lemon restore hair from its insides out. A mixture of freshly cut fruit juice and lemon juice makes a pleasant tonic. Put this remedy on your scalp. Let it sit for 30 minutes. To rinse your hair, use warm water.[38]
Use Alma water to wash your hair. Add a couple of freshly crushed amla in a water dish. Let the water come to a boil. Give the water at least thirty to forty minutes to cool and drain. Dried gooseberry slices can be soaked in water for a whole night.
For optimum results, clean your hair with such water every day.[39]
Use Shiitake and Amla for Strong Hair: It's well known that shiitake and amla mushrooms support healthy hair. Make a hair mask with powdered shiitake mushrooms and amla. Add water and carefully stir. Use the mask and keep it on for 30 minutes if you have lengthy hair. Rinse your hair well with cold water. Use this combination to help control hair loss .[40]

Fig . No.7: Indian Gross Berry (Amla)
5. Aloevera Hair Mask
Aloe Vera Hair Mask Benefits: Aloe Vera's anti-inflammatory properties reduce skin inflammation. The fatty acids and enzymes in aloe vera help to reduce inflammation. Its moisturising qualities are beneficial to dull, dry hair. In addition, aloe vera contains vitamin C, folate, and choline to support good hair. It is known as an organic hair cleanser since it eliminates dead tissue, excess filth, sebum, and dirt from the scalp and hair. Aloe vera keeps the scalp clear and helps prevent dandruff. Aloe vera hair mask's many antibacterial, antifungal, and antiviral properties help to eliminate microbial illnesses in the hair.
It also protects the hair by fortifying the hair roots. Additionally, aloe vera has components that encourage hair development. Your scalp's pH balance is restored by using an aloe vera hair mask. Your mane will appear glossy if you use an aloevera hair mask for curly hair.
Aloe vera hair masks and shampoos have a variety of uses. Among the possibilities that can be prepared at home are egg and aloe hair masks and coconut and aloe hair treatments.[41,42]

Fig.No.8; Aloevera Hair Mask

Fig .NO.9: Aloevera Hair Mask
CONCLUSION:
The immune-mediated, multifactorial condition known as alopecia areata still poses serious therapeutic and psychological difficulties. Its unpredictable course, fluctuating diagnosis, and frequent relapses necessitate a personalised and all-encompassing management approach, even though it is non-scarring and frequently reversible. Results and standards of life can be enhanced by timely diagnosis and suitable intervention. New treatments like as JAK inhibition, PRP medications, and immune-modulating agents have had encouraging outcomes in resistant cases, but corticosteroids continue to be the cornerstone of care. By enhancing scalp health and fortifying hair follicles, natural therapies like oil of coconut, fenugreek seed, onions oil, amla, and aloe vera may offer additional benefits in addition to medical care. However, additional clinical verification through controlled trials is needed to confirm their effectiveness.
REFERENCE


Aishwarya Mane, Dr. Sanjay Bais, The Review on Alopecia Areata : A Comprehensive Review of Pathogenesis, Diagnosis, Clinical Pattern and Remedies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3743-3753. https://doi.org/10.5281/zenodo.18063502
 10.5281/zenodo.18063502
10.5281/zenodo.18063502
