Department of pharmaceutics, Rasiklal.M. Dhariwal Institute of pharmaceutical education and research,Chinchwad,Pune.
Keratosis pilaris often manifests in small, hard bumps on the legs and arms. A common treatment method for many acne conditions, such as keratosis pilaris, in such cases, mostly acids are used for the treatment, which have shown a promising effect in recent years. This review examines the use and success of multiple types of acids, steroids, and kinase inhibitors in clinical and non-clinical settings to treat and understand keratosis pilaris. In the treatment of keratosis pilaris, acid primarily works by breaking down the dead skin cells that clog the hair follicles. Some types of steroids have anti-inflammatory properties that have proven useful in minimizing the appearance of acne. Kinase inhibitors control important skin cell functions, such as cell signaling, metabolism, division, and survival, which undoubtedly affect the appearance of skin as a whole. The known impact of acid, steroids, and kinase inhibitors on keratosis pilaris is underestimated and should be given more attention by healthcare industry leaders.Further research is needed to better recognize the pathophysiology of Kertosis Pilaris and to discover more effective therapeutic interventions. Treatment options include topical exfoliants, moisturizers, and keratolytics, although Keratosis Pilaris typically resolves on its own over time. The condition is often mistaken for other dermatological issues, highlighting the need for accurate diagnosis and management.
Keratosis pilaris is a benign but frequent follicular eruption characterized by small, rough, keratotic papules in a folliculocentric distribution. [1] It tends to occur commonly on the extensor surfaces of thighs, arms & buttocks but can also occur on cheeks, face, and trunk. The lesions may be associated with some degree of erythema, leading to the characteristic "chicken skin" description of their pebbly surface. Ketratosis Pilaris is usually asymptomatic and not medically important, but most find it cosmetically displeasing. This self-perceived view is strongly impactful on psychological well-being and quality of life, such that patients present to dermatological care for treatment despite the benign nature of the condition.[2] Epidemiological evidence shows that Keratosis Pilaris is the most frequent follicular skin disease of childhood & it has been estimated that 40% of all adults globally may be affected by it. Surprisingly little has been written about Keratosis Pilaris compared to other papuludedmatoses like atopic dermatitis or acne vulgaris, as a result of its extremely usual occurrence. Pathogenesis, outcome of treatment, and measurement of Keratosis Pilaris remain ill-characterized in the literature, and no accepted standardized measure of disease severity is applied. Such an instrument would be extremely useful both in the research and clinical settings, as it would allow objective measure of response to treatment and inform therapeutic decisions.
The review will attempt to collate and summarise the existing knowledge base regarding Keratosis Pilaris, including its clinical presentation, epidemiology, subtypes, co-morbidities, psychological morbidity, and management options. Primary focus will be given to the requirement for a validated and standardised measurement tool for the disease, a domain of anecdotal lack in current evidence. Identification of knowledge gaps serves to highlight probable future directions for research.
More research is required to clarify the pathophysiology of Keratosis Pilaris and to develop improved therapies. Treatment involves topical exfoliants, emollients, and keratolytics, yet most cases of Keratosis Pilaris disappear spontaneously over time. Keratosis Pilaris is most frequently confused with other dermatoses and therefore diagnosis and treatment are critical.
Clinically, Keratosis Pilaris is generally asymptomatic but can be mildly pruritic or irritating in some patients. Clinical examination is reserved for the diagnosis, and a biopsy is not required in most instances. Treatment is aimed at suppressing symptoms & may involve topical exfoliants (e.g., salicylic acid, alpha-hydroxy acids or urea), moisturizers & keratolytics to minimize keratin accumulation. Treatments can enhance the look of the skin but will continue and will dissolve naturally with time. [3]

Fig 1.1, Fig 1.2: Visual representation of Keratosis Pilaris
EPIDEMIOLOGY AND ETIOLOGY:
Keratosis pilaris is the most frequent follicular disease in children, and it often continues into adulthood. The condition typically develops in early childhood, typically from age 2 to 10, and continues to become more evident in adolescence.[4] Pubertal hormonal fluctuations, combined with heightened sebaceous activity, may aggravate the follicular plugging that defines Keratosis pilaris. Some patients will improve or even completely resolve the lesions after adulthood, but others will continue to have lesions on a lifelong basis.
Epidemiologic studies have shown that Keratosis pilaris occurs in 50–80% of adolescents and in around 40% of adults. It is frequent in the context of dermatology clinic settings, but its real prevalence is probably greater since numerous patients are not seen because the condition is asymptomatic and benign and therefore do not seek medical evaluation.
In children, Keratosis pilaris usually appears as coarse, small bumps on the cheeks, upper arms, and thighs. In adults, the pattern is more localized to the upper arms, thighs, and buttocks. Involvement of the face diminishes with increasing age. Notably, most adults view their Keratosis pilaris as merely "dry skin," and thus under-estimate the condition. [5]
The severity of Keratosis pilaris demonstrates obvious seasonal variability. The condition generally worsens in colder months when decreased ambient humidity worsens skin dryness and barrier dysfunction. On the other hand, warm and humid conditions potentially soften keratotic papules and improve skin hydration, reducing roughness.
Geographically, Keratosis pilaris has been reported globally but is best described in lighter skin phototypes (Fitzpatrick I–III). This can be in part due to a diagnostic bias since erythematous papules are more easily seen on fair skin. Darker skin types could possibly present as hyperpigmented papules and thus may be less easily recognized. Notwithstanding these comments, there are no strong global prevalence studies and regional differences remain poorly documented.
Keratosis pilaris has been noted in both men and women, although a number of studies indicate a slightly greater frequency in females. This may be caused by hormonal factors, genetic variation, or merely greater cosmetic concern and health-seeking behavior in female patients. In children, no gender predilection exists. [6]
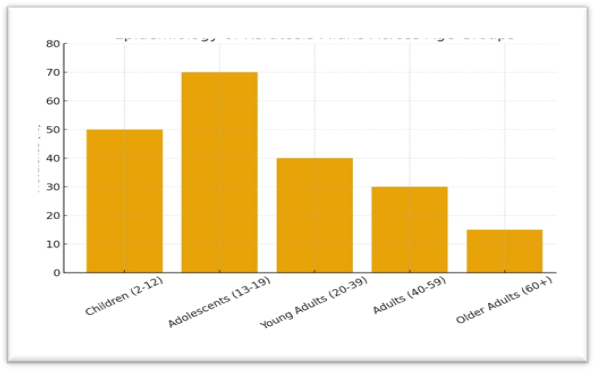
Fig 1.3: Epidemiology
Here’s a bar graph showing the approximate prevalence of Keratosis pilaris (Keratosis pilaris) across different age groups.
The etiology of Keratosis pilaris is not clear, but it is believed that the condition results from follicular keratinization abnormalities. The hyperkeratinisation causes blocking of the follicular orifice with keratin and leads to the papules. Perifollicular erythema and inflammation, which sometimes occur, cause the redness and coarsening.
Keratosis pilaris represents a papulosquamous disease, a heterogeneous group of illnesses presenting with scaly papules and plaques, with an indeterminate etiology. Keratosis pilaris is expected to be congenital in an autosomal leading fashion with adjustable penetrance. The pathophysiology of Keratosis pilaris is unclear and several hypotheses for its etiology have been proposed. The most popular hypothesis is that keratotic infundibular plug in Keratosis pilaris is due to abnormal follicular epithelial keratinization. Thomas et al. suggest that Keratosis pilaris is not an intrinsic keratinocytic abnormality but a hair shaft disease. Keratosis pilaris is a condition where hair shafts that are coiled break the follicular epithelium, triggering inflammation & abnormal follicular keratinisation. This was first discovered when hair shafts from Keratosis pilaris patients removed by a needle still maintained their looped appearance even when they had been removed from the follicle. [9] But this study was on a limited sample of 25 patients and more work would be needed to confirm this. In addition, Gruber et al. have hypothesised that hair shaft defect and aberrant keratinisation can be clarified by the lack of sebaceous glands at an initial stage of Keratosis pilaris pathogenesis.[7]
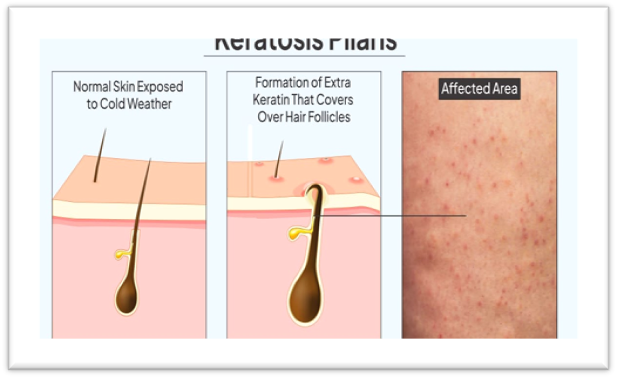
Fig 1.4: Mechanism of Keratosis Pilaris
CLINICAL FATURES:
Keratosis pilaris presents as small, rough, follicular papules, typically skin-coloured, red, or brown depending on skin type. They are commonly described as “goose-bump like” in texture. Distribution is usually symmetrical, affecting:
1. Overall Appearance of Lesions:
The characteristic of keratosis pilaris is the formation of small, rough, keratotic papules. The papules are secondary to keratin plugging of the hair follicles. In contrast to acne, these lesions are not inflamed pustules but separate, hard, and sometimes minimally elevated bumps.
Size: The papules are usually 1–2 mm in diameter.
Shape: Dome-shaped, round, or conical.
Consistency: Coarse and hard on palpation, sometimes described as being "goosefleshed" or "sandpaper-like."
Surface: Papules can be covered with a white fine scale or possess a central keratin plug.
Plugging is in some instances so prominent that a curled hair becomes trapped beneath the surface, causing irritation or superficial erythema.
2. Distribution of Lesions:
Keratosis pilaris possesses an extremely characteristic distribution pattern, by which it can be distinguished from other follicular dermatoses.
Extensor surfaces of upper arms
Thighs (particularly outer surfaces)
Buttocks
Cheeks & occasionally the jawline (especially in children and adolescents)
Forearms, Back, Lower legs: The lesions are generally bilateral and symmetrical in their distribution, which is a helpful diagnostic point. For instance, both of the upper arms are affected to an equal extent and not one side more than the other.
3. Skin Texture:
One of the most notable characteristics of Keratosis pilaris is the surface roughness of skin. The skin is coarse & pebbly to palpation, like:
Sandpaper, Chicken skin, Plucked gooseflesh.
The texture is also usually more obvious than visible appearance. Patients complaines about the skin not being smooth, particularly when rubbed or touched, even if bumps are unobtrusive to the eye.
4. Changes in Color:
Color of keratosis pilaris lesions also varies based on a host of factors such as skin type, degree of inflammation, and chronicity.
The papules could be flesh-colored, white, or pale pink.
Some of the lesions have border erythema, giving them a red "pinpoint" appearance.
The papules could be dark brown, grayish, or hyperpigmented.
Post Inflammatory Hyperpigmentation is more prevalent.
In either case, coloration is usually mild and does not indicate significant inflammation, unlike acne or folliculitis.
5. Symmetry and Pattern:
A typical feature of Keratosis pilaris is symmetrical and bilateral distribution. Both thighs, or both cheeks, and both arms are usually involved equally. This distinguishing feature separates it from folliculitis, where lesions may occur more randomly or asymmetrically.
Distribution is folliculocentric—one papule per hair follicle orifice. Follicular involvement is one of the main diagnostic features.
6. Symptoms and Patient Complaints:
Keratosis pilaris is usually asymptomatic but, at times, produces minimal discomfort. Some of the symptoms are:
Surprisingly, Keratosis pilaris is not painful and does not generate systemic symptoms.
7. Seasonal Changes:
Severity of keratosis pilaris tends to vary seasonally:
8. Age of Onset and Natural Course:
9. Associated Conditions:
Keratosis pilaris also presents in association with other dermatologic conditions, most notably those of abnormal keratinization or dryness.
These are not diagnostic, but give extra clinical information.
10. Variations of Keratosis Pilaris:
Although the classic one is most prevalent, there are variations with slightly different clinical presentations:
Keratosis pilaris atrophicans: Uncommon variant of scarring follicular atrophy. Encompasses conditions like ulerythema ophryogenes (eyebrow involvement).
Identification of these variants assists clinicians in distinguishing between subtle presentations.
11. Psychosocial Impact:
Although Keratosis pilaris is not medically significant, its effect on quality of life can be huge. Patients can feel:
Self-consciousness due to visible lesions on the arms, cheeks, or legs. Low self-esteem, particularly during adolescence. Anxiety due to the false assumption that Keratosis pilaris is an infectious or hygienic illness. Reassurance and counseling are a crucial component of clinical management.
ASSOCIATIONS WITH OTHER CONDITIONS:
Keratosis pilaris is a benign dermatologic condition cutaneous presents with numerous small, rough papules most classically scattered over the extensor surfaces of arms, thighs, buttocks & occasionally the cheeks. While it is oftentimes simply considered an unproblematic cosmetic issue, studies have determined that Keratosis pilaris is most often not an independent event. Rather, it may occur in association with a wide range of dermatologic & systemic diseases. These relationships are of interest to researchers and clinicians alike in the context that they provide information on possible common mechanisms, genetic overlaps, as well as clinical correlations. Discussion below also considers the most suitable relationships of Keratosis pilaris with special emphasis on atopic dermatitis, ichthyosis vulgaris, obesity and metabolic syndrome, and other follicular diseases.
1. Relationship with Atopic Dermatitis (AD):
Shared Pathophysiological Mechanisms:
The link between Keratosis pilaris and AD can be attributed to a shared disruption in immune regulation and epidermal barrier function. Both diseases share disturbances in keratinization along with disruption of the epidermal barrier resulting in inflammation and dryness.
Clinical Implications:
AD patients are predisposed to Keratosis pilaris development during the adolescent years, with subsequent erythematous or more inflamed papules.
Erythematous or more inflamed papules are followed by atopic Keratosis pilaris, which can cause pruritus, cosmetic distress, and lower quality of life, although Keratosis pilaris is asymptomatic in non-atopic subjects.
This association is significant because treatment of Keratosis pilaris in AD patients can involve intensive moisturization, barrier repair therapy, and sometimes anti-inflammatory treatment. [12]
2. Association with Obesity and Metabolic Disorders:
In the obese, Keratosis pilaris is more widespread and symptomatic. The association invites one to think of Keratosis pilaris not only in its cosmetic but also as a possible cutaneous marker of hidden metabolic risk. Promoting weight reduction and maintenance of metabolic health may indirectly enhance Keratosis pilaris.
PSYCHOSOCIAL IMPACT:
Keratosis pilaris is a very prevalent skin condition of small, rough papules that normally reside on the upper arms, thighs, buttocks, and occasionally face. From a health point of view, Keratosis pilaris is benign: it is not a source of much or even any physical pain, it is not a symptom of systemic illness, and it is not infectious. But beyond the surface level of its clinical appearance is a true but all too frequently overlooked factor — its psychosocial impact. The condition, while not physically incapacitating, will have a profound impact upon self-esteem and interpersonal relationship. Physical manifestation of Keratosis pilaris is a strong factor that influences self-esteem, social role, and quality of life in most patients, especially adolescents and young adult. [20]
1. The Problem of Cosmetic Noticeability:
Compared to cutaneous chronic inflammatory dermatoses like psoriasis or atopic dermatitis, Keratosis pilaris is a rare cause of burning, tenderness, or pruritus. Its most debilitating failure is not pain but cosmetic visibility. The miniature, thick, red papules render the skin sandpapery hard to the touch, an erroneous assumption that it is "acne," "rash," or "poor hygiene." It is embarrassing and socially stigmatizing.
Keratosis pilaris is also most commonly found in childhood and adolescence - years of increased self-concept, body image, and peer acceptance susceptibility. Keratosis pilaris is most commonly found in teenagers who say they feel "different" or "not perfect" from others, particularly when the papules are visible on cheeks, forearms, or legs. Social comparison, especially in today's age of social media and photoshopped ideals of beauty, increases self-consciousness.
• Avoidance of short-sleeved shirts, swimming, or activity with use of involved areas is described in the majority of adolescents.
• Avoidance of physical education class or athletics on the basis of concern over embarrassment is described in others.
• Avoidance diminishes access to social integration and threatens physical health through reduced levels of activity.
2. Comparative Insights: Keratosis pilaris and Other Dermatological Conditions:
Keratosis pilaris vs Acne:
Acne vulgaris is the most studied dermatological condition in the area of psychological morbidity. Like Keratosis pilaris, acne typically arises in adolescence and is physically apparent. Although while acne is typically marked by pain, inflammation, and scarring ability, Keratosis pilaris is not. But whereas Keratosis pilaris patients' pain is of roughly the same magnitude as that of mildly acnes patients, it is for the same reason working in both cases: physical visibility and subjective difference from normal-skin appearance.
Keratosis pilaris vs Psoriasis and Atopic Dermatitis
In contrast to psoriasis & atopic dermatitis, Keratosis pilaris is not associated with systemic inflammation or severe itching. Embarrassment and lifestyle restriction do occur, nonetheless. This difference reminds us that psychosocial morbidity of skin disease is separated from medical severity. Mild illness can have enormous emotional weight when visible skin surfaces are altered.
3. Quality of Life Studies: [19]
The psychosocial impact of Keratosis pilaris is shown by current quality of life (QOL) studies
CURRENT TREATMENT OPTIONS:
Keratosis pilaris (Keratosis pilaris) is still one of the most frequent but frustrating dermatologic complaints seen in the clinic. Benign but frequently asymptomatic, its cosmetic presentation- follicular papules, erythema, and textural alteration-provides intense cosmetic morbidity, most typically in adolescents and young adults. Thus, they come to the clinician or the over-the-counter sector with a desire to enhance the cosmetic appearance of the skin. Even though treatment of Keratosis pilaris is normally rational, since no cure exists and relapse is an easy job once therapy has stopped. Therapeutic modalities are thus more or less symptomatic in nature and try to enhance evenness of the skin, alleviate erythema, and maximize cosmetic results.
7.1 Emollients:
Liberal moisturizing is the foundation of Keratosis pilaris treatment. Keratosis pilaris is causally linked with dryness, roughness, and barrier defect, and hence emollients play a central role in softening papules & lessening tactile roughness.
Mechanism of action: Emollients hydrate the stratum corneum, diminish transepidermal water loss & enhance skin barrier function. Mild keratolytics or humectants may be incorporated in some mixtures that facilitate desquamation of keratin plugs.
Formulations of choice: Urea creams (10–20%): Both moisturize and have keratolytic effect by disrupting hydrogen bonds in keratin. Lactic acid lotions (5–12%): Less irritable exfoliants with humectant properties, providing smoother texture. Ceramide moisturizers: Repair barrier lipids and potentially offer long-term hydration.
Clinical effects: Emollients do not eradicate lesions in most instances but obviously enhance skin feel and appearance with sustained therapy. But this must be repeated daily, because relapse is quick when it is discontinued. [21]
7.2 Topical Retinoids:
Topical retinoids such as tretinoin, adapalene, and tazarotene are reserved for resistant cases.
Mechanism of action: Retinoids re-establish differentiation of keratinocytes, decrease hyperkeratinization, and perhaps remove plugged follicles. They also improve epidermal turnover, firmness and color.
Efficacy: There have been many small trials which demonstrate improvement of roughness and pigmentation with retinoid treatment. Less irritating adapalene can be used where there is sensitive skin. [22] , [23]
7.3 Laser and Light Treatment:
In cases with an excess of cosmetic morbidity, laser and light therapy constitute a new choice. They are used mainly for the treatment of erythema and papules that are refractory to treatment.
Treats vascular elements of erythematous Keratosis pilaris. Decreases redness and inflammation, particularly beneficial in keratosis pilaris rubra.
Mechanism of action: The Pulsed Dye Laser emits an intense beam of light at a specific wavelength (commonly 585–595 nm) that targets oxyhemoglobin - the red pigment in blood vessels. This process is based on the principle of Selective Photothermolysis, which means: The laser selectively heats and destroys the target (blood vessels causing redness or inflammation) while sparing surrounding skin tissues.
More penetrating & can treat papules and pigmentation.
Mechanism of action: An Nd: YAG laser works by using Nd: YAG as the active medium to produce a high-intensity beam of light, primarily at a wavelength of 1.064um. A flash lamp pumps energy into the neodymium ions, exciting them to higher energy levels. These eager ions then come back to a lower energy state, releasing photons in a process called stimulated emission, which are amplified between two mirrors to create a laser beam.
Potentially improves skin texture and colour but experience is not common.
Mechanism of action: A fractional CO2 laser works by creating microscopic columns of heat and micro-ablations in the skin, which promotes the body's natural healing mechanism to generate new, healthier tissue. The laser's infrared light is absorbed by water in the skin, vaporizing the outer layers and stimulating collagen production for a firmer, smoother, and tighter appearance. The "fractional" aspect leaves healthy skin between the micro-injuries, allowing for faster healing than traditional, fully ablative lasers.
Treats vessels and pigment with non-coherent light energy.
Mechanism of action: IPL, or Intense Pulsed Light, targets certain pigments (chromophores) in the skin, such as hemoglobin or melanin, using broad-spectrum light. The light is absorbed, converting to heat which destroys the target cells, leading to hair removal, reduction of pigmented or vascular lesions, or collagen stimulation.
7.4 Other Modalities:
A number of other or adjuvant therapy have been used for Keratosis pilaris, but most are weakly supported by robust clinical evidence.
Is a physical abrasion utilized to buff the skin surface. Will result in temporary change but effects are fleeting. Is a minimally invasive cosmetic technique that uses a instrument to softly exfoliate top layer of skin to extract dead skin cell and enhance texture. It is nonsurgical treatment that is performed by professional and is used to treat problems like uneven acne, skin tone, scars, fine lines, and sun damage.
Peels with a number of agents including glycolic acid, salicylic acid & trichloroacetic acid have been tried. May cause deeper exfoliation but is accompanied by a higher risk of irritation and post-inflammatory hyperpigmentation.
Several vitamin D analogues, anti-inflammatory agents, and peptides have been described recently. Evidence is preliminary and pending confirmation.
Used very infrequently, other than syndromic or refractory Keratosis pilaris. Oral retinoids are documented in individual case reports but should not be used because of their side effect profiles.
More objective monitoring of treatment, increasing trust in therapies. Validation of problems, as their cosmetic and psychosocial problems are addressed in a formal context. Potential for access to more specific treatments as new treatments become established.
A systematic critique of current literature in turn illustrates several key gaps that are constraining improvement in clinical care, as well as scientific understanding of Keratosis pilaris. Fulfillment of the gaps is essential to promote patient outcomes, guide evidence-based practice, and drive future research.
Small patient numbers, typically fewer than 50. Brief follow-up periods, so safety and efficacy over the long term cannot be determined. Heterogeneous outcome measures, making studies incomparable.
CLINICAL PRESENTATION AND DIAGNOSIS:
Keratosis pilaris is a benign, chronic, & prevalent keratinization disorder presenting as small, coarse, folliculocentric papules. Benign though it is, the process frequently leads to cosmetic distress and at times to discomfort, pruritus, or secondary change such as post-inflammatory pigmentation and scarring. The clinical presentation of Keratosis pilaris is according to distribution, morphology, and severity, while diagnosis is primarily clinical but aided with dermoscopy and sometimes with histopathology.
The characteristic presentation of Keratosis pilaris is the formation of spiny, keratotic papules measuring approximately 1mm in diameter. The papules are usually rough to palpate and have been compared to the feeling of "gooseflesh," "chicken skin," or "sandpaper." The papules form because of follicular plugging secondary to hyperproduction of keratin, which ensnares fine, coiled, brittle vellus hair within the follicular orifice. The papules in most cases are only slightly erythematous or skin-colored, but exceptions exist depending on the type of Keratosis pilaris and level of inflammation.
Generally asymptomatic in most cases, some patients do have mild pruritus, but specifically if seen in temperate climates, or as an association with xerosis (dryness). Patients are bothered more by the cosmetic effect of lesions, and so, seek out the dermatologist. [14]
Keratosis pilaris most commonly affects hair-bearing skin surfaces, particularly those over extensor surfaces. The most common sites are:
The condition is rarely seen on glabrous skin (e.g., palms and soles), as the presence of follicles is a pre-requisite for papule formation.
Several clinical presentations of Keratosis pilaris have been described, each with distinct characteristics:
Characterized by prominent perifollicular erythema along with characteristic papules. Most commonly seen on cheeks and proximal arms. The erythema is also typically persistent and cosmetically disconcerting, giving the skin a reddish or inflamed appearance. Patients will often mix up this subtype with early rosacea.
Papules are whitish or grayish in color and have little erythema. This subtype is more common in patients with lighter skin. The lesions are less noticeable but can also roughen the skin.
A less common but clinically significant subtype. Includes follicular plugging followed by scarring and atrophy with fading of papules. It occurs with alopecia (particularly of eyebrows and scalp margins) and scarring pitting. Variants of this type include ulerythema ophryogenes (eyebrow involvement) and atrophoderma vermiculatum (honeycomb scarring). This type tends to persist into adulthood and is likely to be more of a cause of psychologic distress due to scarring and hair loss. [16]
Keratosis pilaris with hyperpigmentation – more common in darker phototypes of skin, where there is inflammation leading to post-inflammatory hyperpigmented macules around papules.
Erythromelanosis follicularis facieietcolli – erythema, hyperpigmentation, and follicular papules involving rare variant limited to face and neck.
Although papules are the primary feature, secondary changes may follow:
Keratosis pilaris may masquerade or mimic a number of dermatoses. Clinical inspection is therefore prudent. The appropriate differentials are:
DIAGNOSTIC APPROACH [30]
1. Clinical History:
History-taking will generally be sufficient to render a suggestion of Keratosis pilaris. Consider:
Age of onset: Keratosis pilaris is most commonly seen in childhood or adolescence but is occasionally persistent throughout adult life.
Family history: Familial predisposition is common; several people have affected family members.
Associated conditions: Atopy, ichthyosis vulgaris, and keratoderma are common associations.
Symptoms: Symptomatically asymptomatic in most patients, but in some cause itching, dryness, or cosmetic distress.
Exacerbating factors: Cold temperature, dry climate, and low humidity can potentially aggravate symptoms.
2. Physical Examination:
Visual and palpation inspection of the skin reveal:
Small, folliculocentric papules which can be skin-colored, erythematous, or whitish. Rough texture most evident on extensor arms and thighs. Symmetry of distribution and sparing of non-follicular areas. Secondary changes such as erythema, pigmentation, or scarring according to subtype.
3. Dermoscopy:
Dermoscopy is a useful, non-destructive diagnostic tool which enhances visibility and is able to differentiate Keratosis pilaris from associated disorders. Characteristic dermoscopic findings are:
Follicular plugs of keratin, Coiled or whorled vellus hairs in papules, Perifollicular erythema and scaling, Dermal vascular ectasia, Enlarged follicular orifices, Hyper- or hypopigmentation of follicle environs.
Dermoscopy is also an objective way of recording baseline severity and follow-up treatment response, valuable in both clinical and research settings.
4. Histopathology (Rarely Indicated):
Histopathological diagnosis is rarely required but can be required for atypical or severe lesions. Characteristics are:
Hyperkeratosis and ostia plugging of follicles, Mild perifollicular lymphocytic infiltrate, Sebaceous gland atrophy in some types, Trapped vellus hair shaft in keratin plug.
5. Patient-Reported Outcomes:
Since Keratosis pilaris is normally a cosmetic and not a symptomatic skin condition, the psychosocial impact must be assessed. Some patients are self-conscious, feel lower about themselves, or are withdrawn socially due to observable lesions if the face or the exposed skin surfaces are involved.
No widely accepted standard scoring system for Keratosis pilaris severity currently exists, but physicians typically grade on:
Number of lesions, Distribution of sites involved, Severity of erythema, Roughness of skin (texture), Scarring or pigmentation. Development of severity grading is a dermatological unmet need to have standardized instruments for.
Keratosis pilaris is an innocent condition and typically self-limiting. The lesions can improve over age in a majority of patients and recover spontaneously in adulthood. Persistence into later life does take place, however, particularly in those who present with severe varieties or with coexistent atopic conditions. Dissatisfaction with appearance remains the primary concern in most patients, thus serving to highlight the importance of sensitive clinical management.
ROLES OF ACIDS, STEROIDS:
It is a common ingredient of many acne products because it is able to clean out the pores.
Since kinase inhibitors block enzymes known as tyrosine kinases, they have also been shown to have an impact on keratosis pilaris and its related variations. Since tyrosine kinases aid in conveying advanced signals in cells, obstructing them limits cell division & development. The majority of alopecia's negative effects, mostly skin scarring, are caused by the kinase inhibitor nilotinib. Another noteworthy kinase inhibitor is vemurafenib, a BRAF inhibitor utilized to treat metastatic melanoma, a kind of skin cancer when cells that produce color in skin turn cancerous.
Steroids are among the chemicals that affect keratosis pilaris. Topical & systemic steroids immediately treat acne conditions by reducing inflammation. Based on the research included in the current review, some particular examples of steroids affecting acne issues include mometasone furoate, triamcinolone, prednisone, hydrocortisone, testosterone, methylprednisolone & clobetasol propionate.
Keratosis pilaris is a genetic illness; hence, some of the amino acid-producing genes may have an effect on the condition. For example, the fibrinogen alpha chain & guanine nucleotide exchange factor 1 genes encode amino acids that produce proteins that affect acne & hyperpigmentation.
The importance of concentration & dose. Acids, steroids & kinase inhibitors all have an effect on keratosis pilaris, although the kinds differ depending on the quantity and dose. Acid's intended benefits for the skin may not always be realized at low doses. This will mostly impact people with sensitive skin types. Acid concentration is also determined by type of acid employed.
The dosage of steroids & kinase inhibitors. Dosages of steroids are important to consider for medications since too much or too tiny might cause unpleasant side effects. For example, testosterone is directed in doses ranging from 1.1 to 8 nmol. According to the research, the recommended doses for hydrocortisone, triamcinolone, mometasone furoate & clobetasol propionate are 2.5%, 0.1%, and 0.05%. The daily doses of prednisone and methylprednisolone are 20mg & 6mg, respectively.
Kinase inhibitor doses are also crucial. Studies show that individuals are given either 600mg or 800mg of nilotinib.
The concentration of acids, as well as the dosages of kinase inhibitors & steroids, is critical for patients suffering from skin problems since the efficacy of skincare products is dependent on the concentration of acids in skincare routine & how it disturbs various skin types. [28] , [29]
TABLE:
Table no. 1
|
Compound/ class |
Herbal/ natural source |
Uses |
Importance |
|
|
Glycolic acid |
Sugarcane, sugar beets, pineapple |
Used in chemical peels, skin exfoliation, and treatment of acne scars, and hyperpigmentation |
Improves skin texture, stimulates collagen production, and promotes youthful appearance. |

|
|
Lactic acid |
Sour milk (curd, yogurt), fermented foods |
Used in skincare for gentle exfoliation, hydration, and treatment of keratosis pilaris |
Maintain skin pH balance, enhances moisture retention, and improves skin smoothness. |

|
|
Salicylic acid |
Willow bark, wintergreen leaves |
Used in acne treatment, dandruff shampoos, warts, psoriasis, and as a keratolytic agent |
Penetrates oil glands, unclogs pores, reduces inflammation, and prevents breakouts. |

|
|
Kinase inhibitors |
Flavonoids from green tea, genistein |
Used in cancer therapy research, anti-inflammatory activity, and regulating cell signaling. |
Help block abnormal cell regulate metabolic pathway potential use in targeted therapies. |

|
REFERENCES


Sayali Deth, Om Salunke, Khushi Sarnot, Anushka Sawant, Priyanka Shaha, Keratosis Pilaris: A Comprehensive Review of Etiology, Diagnosis, and Management., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1575-1592. https://doi.org/Sayali Deth, Om Salunke, Khushi Sarnot, Anushka Sawant, Priyanka Shaha, Keratosis Pilaris: A Comprehensive Review of Etiology, Diagnosis, and Management., Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1575-1592. https://doi.org/10.5281/zenodo.19044866
 10.5281/zenodo.19044866
10.5281/zenodo.19044866
