1,3Rungta Institute of Pharmaceutical Sciences, Bhilai
2,4School of Pharmacy, Anjaneya University, Raipur
2Rungta College of Pharmaceutical Sciences & Research, Bhilai
Diabetes mellitus remains a global public-health challenge, driven by rising prevalence, complex pathophysiology, and the limitations of conventional therapeutic regimens. Novel drug delivery systems (NDDS) are transforming diabetes management by improving pharmacokinetic control, enhancing patient adherence, reducing adverse effects, and enabling targeted or stimuli-responsive therapy. This review-style abstract summarizes current trends and future perspectives in NDDS for diabetes. Recent advances include sustained-release implants and depot formulations that provide prolonged glycaemic control; nanoparticle-based carriers and liposomes that enhance oral bioavailability and protect insulin from enzymatic degradation; transdermal and microneedle platforms that enable minimally invasive insulin and peptide delivery; inhalable formulations that offer rapid systemic uptake; and glucose-responsive “smart” systems that release therapeutics in response to hyperglycaemia. Integration of biosensors, closed-loop delivery, and wearable devices is converging toward automated glycaemic regulation. Challenges remain in scaling manufacturing, ensuring long-term biocompatibility, achieving precise glucose-triggered responsiveness, and meeting regulatory and cost constraints—particularly for low-resource settings. Emerging directions include gene and cell-based delivery, multi-modal platforms combining incretin mimetics and insulin, and personalized therapeutics guided by digital health analytics. With continued interdisciplinary research bridging materials science, bioengineering, and clinical medicine, NDDS hold substantial promise to shift diabetes care from symptom control toward safer, more physiological, and patient-centered glycaemic management.
Diabetes mellitus is a chronic metabolic disease that develops either when the pancreas fails to produce sufficient insulin or when the body cannot effectively utilize the insulin it produce. Insulin, a key hormone in glucose regulation, maintains normal blood sugar levels, and its deficiency or impaired action results in persistent hyperglycemia. Uncontrolled hyperglycemia progressively damages multiple organ systems, especially the nerves and blood vessels, and leads to serious complications over time. Diabetes is primarily characterized by defects in insulin secretion, reduced insulin sensitivity, or both, and is further complicated by a variety of pathophysiological disturbances including chronic inflammation, dysregulated lipid metabolism, oxidative stress, immune dysfunction, and gut microbiota imbalance. Collectively, these abnormalities accelerate disease progression, contribute to both microvascular and macrovascular complications, and significantly impair patients’ quality of life while increasing the risk of premature death. (1) Long-standing hyperglycemia in diabetes progressively damages multiple organs and systems. Common complications include microvascular disorders such as diabetic retinopathy, nephropathy, and neuropathy, along with macrovascular complications like cardiovascular disease, stroke, and peripheral arterial disease. In severe cases, acute metabolic crises such as diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) may occur, both of which are life-threatening without prompt treatment. These chronic and acute complications collectively impose a heavy burden on patient health, quality of life, and Survival. (2) The disease is broadly classified into Type 1 diabetes mellitus (T1DM), an autoimmune condition marked by β-cell destruction and absolute insulin deficiency; Type 2 diabetes mellitus(T2DM), which arises primarily from insulin resistance and progressive β-cell dysfunction; and other specific forms including gestational diabetes mellitus (GDM) and secondary diabetes due to genetic, endocrine, or drug-related causes. T1DM is primarily an autoimmune disease, where autoreactive T-cells attack pancreatic β-cells, leading to absolute insulin deficiency. Genetic susceptibility, viral infections, and immune dysregulation contribute to β-cell destruction, resulting in the failure of insulin production. (3)
T2DM is characterized by a dual defect: insulin resistance in peripheral tissues (such as muscle, liver, and adipose tissue) combined with progressive β-cell dysfunction. Initially, pancreatic β-cells increase insulin secretion to compensate for insulin resistance, but over time, this compensation fails, leading to chronic hyperglycemia. Factors such as obesity, sedentary lifestyle, oxidative stress, and chronic inflammation play a central role in T2DM progression. Overall, the persistent hyperglycemia and metabolic imbalance in diabetes mellitus trigger a cascade of biochemical and molecular changes, including oxidative stress, advanced glycation end-product (AGE) accumulation, endothelial dysfunction, and chronic low-grade inflammation. These processes drive the onset of both microvascular and macrovascular complications, which represent the most devastating consequences of the disease. (4) Diabetes mellitus continues to represent a major global health concern with a steadily increasing prevalence. According to the International Diabetes Federation (IDF) Diabetes Atlas,10th Edition (2021), an estimated 537 million adults aged 20–79 years were living with diabetes, accounting for approximately 10.5% of the global adult population. This number is projected to rise sharply to 643 million by 2030 and nearly 783 million by 2045. The latest IDF Diabetes Atlas,11th Edition (2025) further highlights the escalating burden, reporting that approximately 589million adults worldwide—nearly one in nine—are currently affected, with around 252 million individuals remaining undiagnosed. Moreover, diabetes-related mortality is responsible for over3.4 million deaths annually, and the associated healthcare expenditure has surpassed US $1trillion per year. These alarming figures underline the urgent need for more effective therapeutic and patient-friendly management approaches, including innovative drug delivery systems, to address the growing global burden of diabetes. In recent years, novel drug delivery systems (NDDS) such as nanoparticles, microneedles, transdermal patches, pulmonary inhalation systems, and glucose-responsive smart formulations have emerged as promising alternatives to traditional therapies. These advanced technologies aim to enhance insulin stability, improve bioavailability, reduce dosing frequency, and ultimately achieve better glycemic control with improved patient adherence.
This review provides a comprehensive overview of the recent advances in NDDS for diabetes management, with particular focus on oral, transdermal, pulmonary, nanotechnology-based, and smart delivery approaches. In addition, the review highlights current challenges, clinical translation barriers, and future perspectives for the successful integration of these systems into routine diabetes care. (5)
2. TYPE AND ETIOLOGY OF DIABETES MELLITUS: -
Diabetes Mellitus (DM) is a heterogeneous group of metabolic disorders characterized by chronic hyperglycemia due to defects in insulin secretion, insulin action, or both. The condition manifests in several distinct forms, each with unique etiological factors and pathophysiological mechanisms.
A clear understanding of the classification and underlying causes of DM is essential for effective diagnosis, treatment, and research into novel therapeutic approaches.
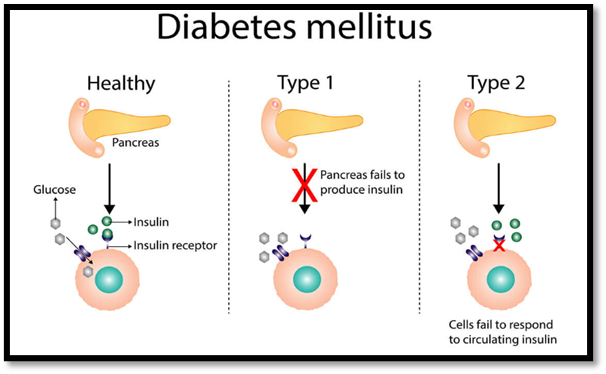
Figure no. 1: Diagram illustrating normal glucose–insulin regulation compared with the pathophysiology of Type 1 diabetes (absence of insulin production) and Type 2 diabetes (insulin resistance at the cellular level).
2.1. Type 1 Diabetes Mellitus (T1DM)
Type 1 diabetes mellitus is a chronic autoimmune metabolic disorder characterized by the destruction of insulin-producing β-cells of the pancreas. This leads to an absolute deficiency of insulin, resulting in hyperglycemia and disturbances in the metabolism of carbohydrates, fats, and proteins. It most commonly develops in children and young adults but can occur at any age.The exact cause of T1DM is multifactorial, involving genetic predisposition, environmental triggers, and autoimmune mechanisms. Genes within the human leukocyte antigen (HLA) complex, particularly HLA-DR3 and HLA-DR4, are strongly associated with disease susceptibility.Environmental factors such as viral infections (e.g., coxsackievirus, mumps), dietary components, and early exposure to cow’s milk proteins may trigger autoimmune destruction of pancreatic β-cells in genetically susceptible individuals.(6)
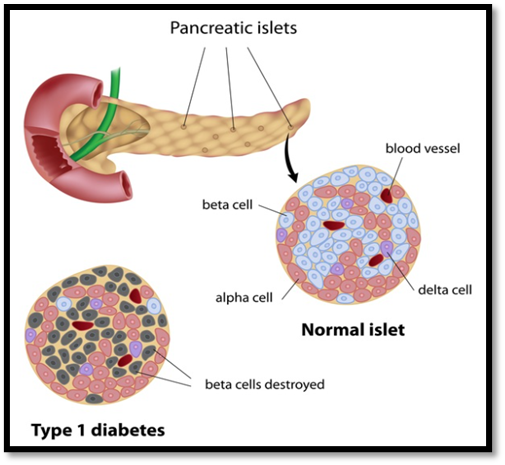
Figure no 2: Structural comparison of normal pancreatic islets and Type 1 diabetes, showing selective destruction of insulin-producing beta cells within the islets of Langerhans.
Pathophysiologically, the immune-mediated destruction of β-cells leads to a marked reduction in insulin secretion. As insulin is the key hormone responsible for glucose uptake and utilization, its absence causes elevated blood glucose levels, glucosuria, and ketosis. Over time, this leads to complications such as diabetic ketoacidosis (DKA), microvascular (retinopathy, nephropathy, neuropathy) and macrovascular (cardiovascular disease) complications. The management of Type 1 diabetes primarily relies on exogenous insulin therapy to maintain euglycemia. Conventional insulin regimens include multiple daily injections or continuous subcutaneous insulin infusion through pumps. However, maintaining optimal glycemic control remains challenging due to fluctuations in insulin requirements, variability in absorption, and the risk of hypoglycemia. (7)Recent advances focus on closed-loop insulin delivery systems (artificial pancreas), pancreatic islet cell transplantation, and immunotherapy aimed at preserving residual β-cell function.Additionally, novel drug delivery systems (NDDS) such as oral, transdermal, and smart glucose-responsive formulations are being developed to reduce injection frequency and improve patient compliance.
2.2. Type 2 Diabetes Mellitus (T2DM)
T2DM is the most prevalent form of diabetes, accounting for more than 90% of global cases. It is characterized by insulin resistance in peripheral tissues combined with progressive β-cell dysfunction. The etiology is multifactorial, involving genetic susceptibility, obesity (particularly visceral adiposity), sedentary lifestyle, and unhealthy dietary habits. It often coexists with metabolic syndrome features such as hypertension and dyslipidemia.The development of T2DM is multifactorial, involving a complex interplay of genetic predisposition, obesity (particularly visceral adiposity), physical inactivity, and unhealthy dietary patterns.Environmental and behavioral factors such as stress, aging, and poor sleep also contribute to insulin resistance. The disease frequently coexists with components of the metabolic syndrome, including hypertension, dyslipidemia, and central obesity, which further heighten cardiovascular risk.(8)
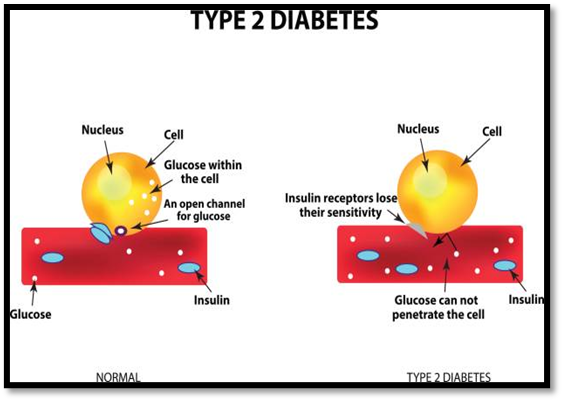
Figure no. 3: Illustration depicting insulin resistance in Type 2 diabetes, where reduced insulin receptor sensitivity prevents glucose uptake into cells despite the presence of insulin.
From a pathophysiological standpoint, insulin resistance causes impaired glucose uptake in muscles and adipose tissue, while excessive hepatic gluconeogenesis maintains elevated fasting glucose levels. Over time, the pancreatic β-cells undergo functional exhaustion and apoptosis, leading to relative insulin deficiency and worsening glycemic control. Clinically, T2DM progresses gradually and may remain asymptomatic for years before diagnosis. Persistent hyperglycemia leads to both microvascular complications (retinopathy, nephropathy, neuropathy) and macrovascular complications (coronary artery disease, stroke, peripheral vascular disease). Management of T2DM involves a stepwise approach, beginning with lifestyle modification (dietary control, regular exercise, and weight reduction), followed by oral antidiabetic agents such as metformin, sulfonylureas, DPP-4 inhibitors, SGLT-2 inhibitors, and thiazolidinediones. In advanced stages or when β-cell function declines significantly, insulin therapy becomes necessary. Despite several pharmacological options, maintaining optimal glycemic control remains challenging due to patient non-compliance, adverse drug effects, and progressive disease nature.(9)Recent research emphasizes combination therapy and novel drug delivery systems (NDDS) aimed at improving drug bioavailability, minimizing dosing frequency, and enhancing patient adherence.
2.3. Gestational Diabetes Mellitus (GDM)
GDM refers to glucose intolerance first recognized during pregnancy. It arises primarily due to pregnancy-related hormonal changes (e.g., human placental lactogen, progesterone, and cortisol),which increase insulin resistance. Women with GDM are at higher risk of obstetric complications and have a greater likelihood of developing T2DM later in life.Women with genetic predisposition, obesity, advanced maternal age, or a family history of diabetes are at higher risk of developing GDM. The prevalence of GDM has been increasing globally, paralleling the rise in obesity and sedentary lifestyle among women of childbearing age.

Figure no 4: Schematic representation of insulin resistance showing desensitized insulin receptors and impaired GLUT4 translocation, resulting in reduced cellular glucose uptake.
If not properly managed, GDM can lead to serious maternal and fetal complications, including preeclampsia, macrosomia (large birth weight), neonatal hypoglycemia, and increased risk of cesarean delivery. Furthermore, women with a history of GDM have a significantly higher risk of developing type 2 diabetes and cardiovascular diseases later in life.(10) Early detection through oral glucose tolerance testing (OGTT) and proper management with dietary modification, physical activity, and insulin therapy when needed are essential to reduce complications. New research is exploring predictive biomarkers and personalized therapeutic approaches to improve maternal-fetal outcomes in GDM.
2.4. Other Specific Types of Diabetes
Apart from type 1, type 2, and gestational diabetes, several less common forms of diabetes exist, collectively referred to as “other specific types.” These forms arise due to genetic defects, diseases of the pancreas, hormonal disorders, or medication use.(11)
a. Monogenic Diabetes
This category includes Maturity-Onset Diabetes of the Young (MODY) and neonatal diabetesmellitus (NDM), both caused by single gene mutations that affect β-cell function or insulin secretion. MODY typically appears in adolescence or early adulthood and is often misdiagnosed as T1DM or T2DM.
b. Secondary Diabetes:
Certain pancreatic diseases (e.g., pancreatitis, cystic fibrosis, pancreatic carcinoma) or endocrine disorders (such as Cushing’s syndrome, acromegaly, and hyperthyroidism) can lead to diabetes due to impaired insulin secretion or increased insulin resistance. Additionally, long-term use of glucocorticoids, thiazide diuretics, antipsychotics, or immunosuppressants may also induce secondary diabetes.(12)
c. Genetic Syndromes Associated with Diabetes:
Some chromosomal abnormalities and genetic syndromes such as Down’s syndrome, Turner’s syndrome, and Klinefelter’s syndrome are associated with an increased risk of developing diabetes.
Overview of Diabetes Management
Diabetes mellitus is a chronic metabolic disorder that requires continuous medical care, lifestyle regulation, and patient education to prevent acute complications and reduce the risk of long-term organ damage. Management strategies primarily aim to maintain normal blood glucose levels and improve quality of life. As each type of diabetes presents unique pathophysiological features, treatment approaches must be individualized. Conventional management relies on lifestyle modification, oral antidiabetic drugs, and insulin therapy.(13)
However, these approaches often face challenges such as variable drug response, frequent dosing, and poor patient compliance, leading to exploration of newer therapeutic and drug delivery approaches.
3. Conventional Therapies for Diabetes Mellitus: -
Diabetes mellitus is primarily managed through both pharmacological and non-pharmacological interventions aimed at achieving normoglycemia and minimizing the risk of chronic complications. Conventional therapeutic strategies include the use of oral antidiabetic agents, insulin therapy, and adjunctive injectable therapies, along with essential lifestyle and dietary modifications. These approaches collectively aim to enhance glycemic control and improve patients’ quality of life.
3.1 Oral Antidiabetic Agents (OADs)
These are mainly used in Type 2 Diabetes Mellitus (T2DM), either as monotherapy or in combination. The major classes include:
3.2 Insulin therapy
Insulin therapy is the cornerstone of treatment for Type 1 Diabetes Mellitus (T1DM) and is also indicated in patients with Type 2 Diabetes Mellitus (T2DM) when oral agents fail to maintain adequate glycemic control. The primary goal of insulin therapy is to mimic normal physiological insulin secretion — maintaining fasting and postprandial glucose levels within the normal range while minimizing the risk of hypoglycemia.(15)
Different formulations of insulin are available, classified according to their onset, peak, and duration of action.
Various regimens such as basal–bolus therapy, split-mix, or continuous subcutaneous insulin infusion (CSII) using insulin pumps are used to optimize glycemic control. Advancements like insulin analogs and smart insulin delivery systems have significantly improved flexibility, reduced glycemic variability, and minimized adverse effects. Despite these improvements, challenges such as injection-site discomfort, strict dosing schedules, and risk of hypoglycemia remain — emphasizing the need for more patient-friendly delivery approaches.(16)
3.3 Other Injectable Therapies in Diabetes Management
In addition to conventional subcutaneous insulin, several other injectable therapies have emerged for diabetes management, particularly for type 2 diabetes. GLP-1 receptor agonists (e.g., exenatide, liraglutide) are peptides that enhance glucose-dependent insulin secretion, suppress glucagon release, slow gastric emptying, and promote satiety, contributing to weight loss and improved glycemic control. Amylin analogs, such as pramlintide, complement insulin therapy by regulating postprandial glucose levels through delayed gastric emptying and reduced glucagon secretion.Long-acting insulin analogs and co-formulations with GLP-1 agonists provide more physiological insulin profiles, reduce injection frequency, and lower the risk of hypoglycemia. These injectable therapies, often delivered via pens or pumps, represent significant advances in personalized diabetes care, offering better efficacy, convenience, and patient adherence compared to traditional insulin injections.
3.4 Lifestyle and Dietary Interventions
Lifestyle and dietary modifications form an integral component of diabetes management and can significantly improve treatment outcomes when combined with pharmacotherapy. Adopting balanced diet, engaging in regular physical activity, and maintaining a healthy body weight are key strategies for optimizing insulin sensitivity and glycemic control.(17)Dietary interventions focus on calorie regulation, macronutrient balance, and low-glycemic-index foods to prevent sharp rises in blood glucose. Patients are encouraged to consume high-fiber meals, limit refined sugars, and practice portion control. Regular exercise enhances glucose uptake by skeletal muscles, improves cardiovascular health, and assists in weight reduction —all of which contribute to better metabolic stability. Lifestyle interventions also include smoking cessation, stress management, and adequate sleep, as these factors influence insulin resistance and overall metabolic health. Continuous patient education, regular monitoring, and counseling play vital roles in sustaining these lifestyle changes. Thus, lifestyle management remains a foundational pillar in both Type 1 and Type 2diabetes care, complementing drug therapy to achieve long-term glycemic stability and prevent complications
4.Limitations of Conventional Diabetes Therapy
Although conventional pharmacological approaches, including oral antidiabetic drugs and insulin injections, remain the mainstay of diabetes management, they are associated with several important limitations.(18)
4.1. Variability in Insulin Requirements:
Insulin needs vary widely among patients and even within the same individual under different physiological or lifestyle conditions. This variability makes dose optimization complex and often leads to episodes of inadequate glycemic control.
4.2. Inability to Mimic Physiological Insulin Secretion:
Currently available insulin formulations fail to replicate the rapid and continuous insulin secretion of the pancreas, resulting in fluctuating blood glucose levels and frequent episodes of hyperglycemia or hypoglycemia.
4.3. Invasiveness and Patient Discomfort:
The subcutaneous route of insulin delivery is invasive and often associated with pain, local irritation, and the risk of infection. These factors can reduce patient compliance, especially in long-term therapy.
4.4. Adverse Effects of Oral Agents:
Many oral antidiabetic drugs are associated with side effects such as gastrointestinal disturbances, weight gain, hypoglycemia, and cardiovascular risks, which may further limit their use in certain populations.
4.5. Complex Dosing Regimens and Poor Compliance:
The need for multiple daily dosing, careful meal-time coordination, and frequent glucose monitoring imposes a psychological and physical burden on patients, leading to decreased adherence and poor long-term outcomes.
4.6 needs of novel Drug delivery system
The limitations of conventional diabetes therapies have prompted significant research interesting the development of Novel Drug Delivery Systems (NDDS). These advanced systems aim to improve the pharmacological and therapeutic outcomes of existing drugs by enhancing their bioavailability, stability, and patient compliance.(19) Conventional oral and injectable formulations often fail to provide precise control of blood glucose levels due to poor absorption, enzymatic degradation, or fluctuating plasma drug concentrations. NDDS technologies offer an opportunity to overcome these challenges by delivering drugs in a more controlled, targeted, and sustained manner. One of the primary goals of NDDS in diabetes management is to mimic physiological insulin secretion and maintain steady plasma glucose levels without frequent dosing or invasive administration. Systems such as transdermal patches, nanoparticles, liposomes, microspheres, and oral insulin formulations have shown promise in providing prolonged and regulated drug release. Additionally, NDDS can minimize systemic side effects and improve the therapeutic index ofantidiabetic drugs by ensuring their site-specific delivery, reducing the required dosage, and improving patient adherence. In the case of insulin, novel delivery systems such as inhalable insulin, mucoadhesive formulations, and glucose-responsive nanoparticles are being extensively explored to eliminate the pain and inconvenience associated with multiple daily injections.Although conventional therapies remain the cornerstone of diabetes management, their long-term effectiveness is limited by several drawbacks, including frequent dosing, invasive administration routes, variable absorption, and poor patient adherence. These challenges highlight the urgent requirement for alternative strategies that can provide sustained glycemic control with minimal side effects.(20) Novel drug delivery systems (NDDS) have been developed to overcome these limitations by improving drug stability, enhancing bioavailability, and offering patient-friendly, non-invasive routes of administration. Furthermore, NDDS aim to mimic physiological insulin secretion more closely, thereby reducing the risk of hypoglycemia and improving overall quality of life. Overall, the Integration of NDDS into diabetes therapy represents a Major step toward personalized and patient- Centric treatment, enhancing not only Efficacy but also the quality of life of Diabetic patients
5. CURRENT TREND IN NOVEL DRUG DELIVERY SYSTEM (NDDS) FOR DIABETES MELLITUS: -
Recent advancements in pharmaceutical technology have led to the development of innovative NDDS approaches designed to overcome the drawbacks of conventional diabetes therapies. These systems focus on controlled, sustained, and targeted drug delivery, thereby improving glycemic control, minimizing adverse effects, and enhancing patient compliance.
5.1 Oral Insulin Delivery Systems
Oral insulin delivery represents a major advancement in diabetes management, offering a non-invasive alternative to subcutaneous injections. Conventional insulin is poorly absorbed in the gastrointestinal tract due to enzymatic degradation and low permeability across the intestinal epithelium. Novel drug delivery strategies have been developed to overcome these barriers, including nanoparticle-based carriers, liposomes, polymeric micelles, and mucoadhesive systems. (21)

Figure no. 5: Overview of advanced oral insulin drug delivery systems, including liposomal, polymeric, metallic, hydrogel-based carriers, microparticles, and modified insulin formulations to enhance oral bioavailability.
These systems protect insulin from enzymatic degradation, enhance intestinal absorption, and provide controlled release, thereby improving bioavailability. Additionally, some oral insulin formulations are being engineered to respond to glucose levels, enabling a more physiological regulation of blood glucose. Although still largely in the experimental or early clinical trial stage, oral insulin delivery systems hold immense promise for improving patient adherence, reducing injection-related discomfort, and revolutionizing diabetes therapy.
5.2 Transdermal Drug Delivery System in Diabetes Mellitus
Transdermal drug delivery systems (TDDS) have emerged as one of the most promising and patient-friendly approaches for the management of diabetes mellitus. These systems deliver drugs through the skin directly into the systemic circulation, thereby bypassing hepatic first-pass metabolism and avoiding gastrointestinal degradation. This route provides several advantages over conventional subcutaneous insulin injections, such as improved patient compliance, painless administration, controlled release, and steady plasma drug concentrations. The skin, however, poses significant barrier due to the presence of the stratum corneum, which restricts the permeation of large biomolecules like insulin. To overcome this limitation, various advanced transdermal techniques have been developed, including microneedles, iontophoresis, electroporation, and ultrasound-mediated delivery.(22)
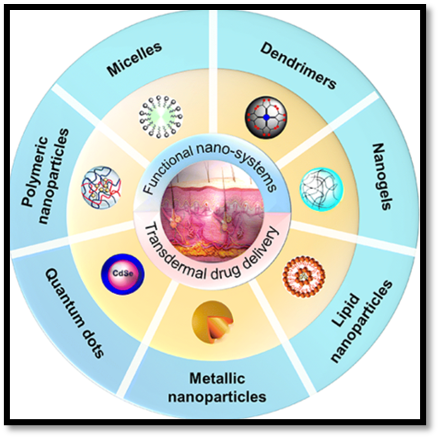
Figure no.6: Classification of functional nanosystems—such as micelles, dendrimers, nanogels, lipid, polymeric, metallic nanoparticles, and quantum dots—used in transdermal drug delivery applications.
Among these, microneedle-based patches have gained special attention for diabetes therapy. These microneedles are made of biodegradable or dissolving polymers that painlessly penetrate the stratum corneum and release insulin into the dermal layer, where it is absorbed into systemic circulation. Recent innovations have led to the development of glucose-responsive microneedle patches that can sense elevated blood glucose levels and release insulin accordingly. Such systems utilize glucose oxidase or phenylboronic acid-based sensing mechanisms to regulate insulin release automatically, minimizing the risk of hypoglycemia.(23) Additionally, wearable smart insulin patches integrated with continuous glucose monitoring (CGM) sensors and feedback-controlled pumps are under development to provide real-time insulin regulation similar to an artificial pancreas.Another promising approach involves the use of lipid-based vesicular carriers, such as transferosomes and ectosomes, in transdermal formulations. These ultra deformable vesicles enhance drug penetration through the skin by altering lipid packing and increasing membrane fluidity.Studies have shown that such carriers can significantly improve the transdermal permeability and bioavailability of insulin and other antidiabetic drugs. Furthermore, polymeric films, gels, and nanocarriers incorporated into transdermal systems allow sustained and stable release profiles, reducing dosing frequency and improving long-term glycemic control.(24)
Overall, transdermal insulin delivery represents a non-invasive, patient-convenient, and technologically advanced approach in diabetes management. Although challenges such as limited permeability for macromolecules, formulation stability, and large-scale manufacturing remain, continuous research and development in microneedle technology, nanocarriers, and smart responsive systems hold immense potential to make transdermal insulin delivery a practical and reliable alternative to injections in the near future.
5.3 Liposomal and Vesicular Drug Delivery Systems in Diabetes Mellitus
Liposomal and other vesicular drug delivery systems have gained significant attention in the management of diabetes mellitus due to their biocompatibility, ability to encapsulate both hydrophilic and lipophilic drugs, and protection of sensitive molecules such as insulin from enzymatic degradation. Liposomes are microscopic vesicles composed ofphospholipid bilayers that can entrap insulin or other antidiabetic agents within their aqueous core or lipid membrane. By modifying their composition and surface charge, liposomes can enhance drug stability, prolong circulation time, and achieve controlled or targeted release. These carriers are especially advantageous for peptide-based drugs like insulin, which are unstable in the gastrointestinal tract and easily degraded by enzymes. (25) In addition to liposomes, several other vesicular systems such azotosomes, transferosomes, and ectosomes have been developed to improve the permeability and bioavailability of antidiabetic drugs. Niosomes, composed of non-ionic surfactants, are more stable and cost-effective than liposomes and have been shown to enhance the transdermal and oral absorption of insulin. Transferosomes, or ultra deformable liposomes, possess high elasticity and can penetrate deep into the skin layers, making them suitable for transdermal insulin delivery. Similarly, ectosomes, which contain high ethanol concentrations, increase the fluidity of skin lipids and facilitate deeper permeation of the drug. These vesicular systems not only offer sustained release but also help maintain steady plasma insulin levels, reducing dosing frequency and minimizing hypoglycemia risk.(26) Recent studies have also explored surface-modified liposomes conjugated with ligands or antibodies that target specific tissues such as the liver or pancreatic β-cells, enabling site-specific drug delivery. Moreover, hybrid nanocarrier systems that combine liposomes with polymers or nanoparticles are being developed to further improve stability and insulin encapsulation efficiency. Overall, liposomal and vesicular carriers represent versatile, biocompatible, and efficient strategy for the controlled delivery of antidiabetic drugs, offering a promising alternative to conventional injection-based insulin therapy and paving the way for more patient-friendly treatment options.
5.4 Pulmonary Drug Delivery System
The pulmonary route has gained significant attention as a non-invasive and efficient method for systemic drug delivery. It utilizes the large surface area of the lungs and the rich blood supply in the alveolar region to enable rapid absorption of drugs into the bloodstream. This route bypasses the hepatic first-pass metabolism, providing higher bioavailability and faster onset of action.(27) In the management of diabetes mellitus, pulmonary delivery of insulin has emerged as a promising alternative to subcutaneous injections. Dry powder inhalers (DPIs) and metered-dose inhalers (MDIs) are the most commonly used devices for this purpose. Insulin particles are engineered to reach the deep lung regions, ensuring efficient deposition and absorption. However, despite its advantages, pulmonary delivery faces challenges such as variability in lung deposition due to breathing patterns, potential irritation of the respiratory tract, and the need for patient training. Moreover, long-term safety concerns regarding repeated administration of macromolecules like insulin through the lungs are still under investigation.(28) Overall, the pulmonary drug delivery system represents a significant advancement in achieving patient-friendly, needle-free administration and improved therapeutic outcomes for chronic diseases like diabetes mellitus.
5.5 Nanoparticle Drug Delivery System
Nanoparticle-based drug delivery systems have revolutionized modern therapeutics by offering targeted, sustained, and controlled drug release.These systems typically consist of particles ranging from 10–1000 nm and are composed of materials such as polymers, lipids, metals, or biodegradable substances. In diabetes mellitus management, nanoparticles are being explored to improve the stability, bioavailability, and pharmacokinetic profile of insulin and other antidiabetic agents.(29)
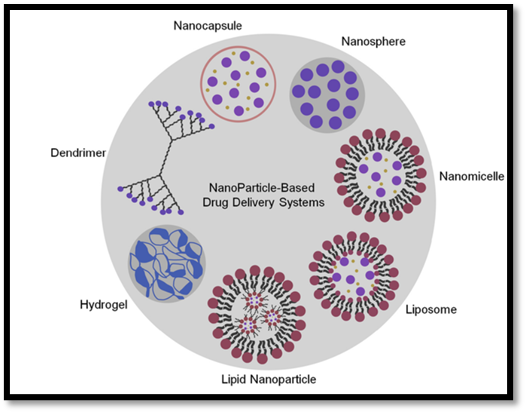
Figure no 7: Schematic representation of various nanoparticle-based drug delivery systems, including nanocapsules, nanospheres, dendrimers, nanomicelles, liposomes, hydrogels, and lipid nanoparticles
.The small size of nanoparticles allows them to penetrate biological barriers efficiently, protecting the encapsulated drug from degradation and facilitating controlled release at the target site. For instance, polymeric nanoparticles such as PLGA (poly lactic-co-glycolic acid) and chitosan-based nanoparticles have been studied for oral insulin delivery to enhance intestinal absorption and prolong therapeutic effect. Similarly, lipid nanoparticles and gold nanoparticles have shown potential for glucose-responsive drug delivery systems that release insulin in response to blood glucose levels. However, some limitations still exist, including potential cytotoxicity, complex manufacturing processes, and challenges in large-scale production. Despite these, the use of nanotechnology in diabetes therapy presents a promising approach to overcome the shortcomings of conventional insulin delivery systems, offering better patient compliance and precise glycemic control.(30)
5.6 Implantable and Smart Drug Delivery Systems
Implantable and smart drug delivery systems represent the next generation of diabetes management strategies designed to provide precise, long-term, and patient-responsive therapy. Implantable systems are miniature devices or biodegradable depots placed under the skin or within body tissues that continuously release insulin or other antidiabetic agents over extended periods. These systems help maintain consistent plasma glucose levels while reducing the frequency of injections and improving patient adherence.
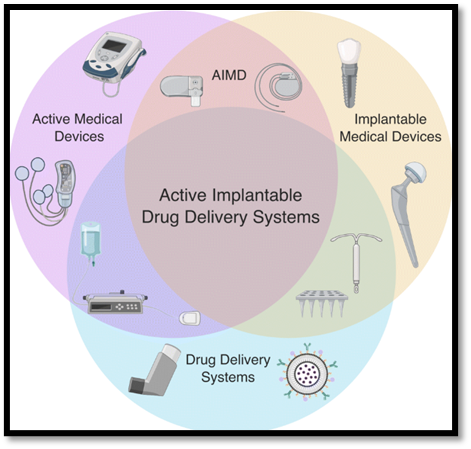
Figure no. 8: Conceptual overlap of active medical devices, implantable medical devices, and drug delivery systems illustrating the integrated framework of active implantable drug delivery systems (AIMDs).
Biodegradable polymers such as poly (lactic-co-glycolic acid) (PLGA) and polycaprolactone (PCL) are commonly used to fabricate implants capable of releasing insulin in a controlled manner for weeks or months. Some advanced implants are programmable, allowing dose adjustment or on-demand release using external stimuli such as magnetic fields or ultrasound.(31) In parallel, smart drug delivery systems have gained immense interest due to their ability to respond dynamically to physiological changes, particularly glucose fluctuations. These systems utilize stimuli-responsive materials that release insulin automatically when blood glucose levels rise, mimicking the function of pancreatic β-cells. Smart delivery platforms are often based on glucose-sensitive polymers, hydrogels, or nanoparticles incorporating glucose oxidase, phenylboronic acid, or concanavalin A assessing elements. Upon detecting high glucose concentrations, these materials undergo structural changes that trigger insulin release, ensuring precise glycemic control and minimizing hypoglycemia risk. Moreover, the integration of microelectronic sensors and wireless communication technologies has led to the development of closed-loop systems, also known as the artificial pancreas. These intelligent systems continuously monitor blood glucose levels and automatically regulate insulin delivery through feedback control, offering a near-physiological approach to diabetes therapy. Although still in developmental stages, implantable and smart delivery systems hold immense potential to transform diabetes care by providing sustained, responsive, and patient-friendly management options that enhance both therapeutic efficiency and quality of life.(32)
6. Advantages, Future Prospects, and Challenges of NDDS in Diabetes Management
Novel Drug Delivery Systems (NDDS) have shown remarkable potential in enhancing diabetes management by addressing many limitations of conventional therapies. They offer improved bioavailability, targeted drug delivery, and sustained release of antidiabetic agents, which can reduce dosing frequency and minimize adverse effects. Approaches such as transdermal patches, nano-formulations, and implantable devices provide enhanced patient compliance and convenience, especially for individuals requiring long-term insulin or oral hypoglycemic therapy. Looking forward, integration of smart technologies, including glucose-responsive and wearable delivery systems, promises personalized, real-time drug administration tailored to fluctuating blood glucose levels. These innovations could optimize therapeutic outcomes and help reduce complications associated with chronic hyperglycemia.(33)
However, despite these advantages, the widespread application of NDDS in diabetes care faces several challenges. High production costs, complex fabrication processes, and stringent regulatory requirements can limit large-scale manufacturing and commercialization. Concerns regarding long-term stability, potential toxicity of novel carriers, and variable patient responses remain significant. Some advanced delivery systems, like implantable or glucose-responsive devices, may necessitate surgical intervention or specialized monitoring, which can restrict accessibility. Additionally, limited clinical data for emerging NDDS approaches makes it difficult to fully evaluate their safety and efficacy. Overcoming these obstacles through continued research, cost-effective technologies, and comprehensive clinical trials is crucial to realizing the full potential of NDDS in providing effective, patient-friendly, and precise diabetes therapies.(34)
7. Current Clinical Applications of NDDS in Diabetes: -
Several Novel Drug Delivery Systems have already found their place in clinical diabetes management, demonstrating practical benefits for patients. Insulin pumps and continuous subcutaneous insulin infusion (CSII) devices have become standard options for patients with type 1 diabetes, providing precise and adjustable insulin delivery while reducing the risk of hypoglycemia.

Figure no. 9: Various types of nanomaterials used as advanced delivery systems for the treatment and healing of chronic wounds.
Transdermal patches and microneedle-based systems are being explored for both insulin and other antidiabetic drugs, offering painless, convenient alternatives to conventional injections. Oral nanoparticle formulations of insulin and other hypoglycemic agents are also undergoing clinical trials, showing potential to improve bioavailability and patient adherence. These systems not only enhance therapeutic outcomes but also improve quality of life by minimizing injection-related discomfort and allowing better glycemic control. The clinical adoption of NDDS reflects a significant shift towards patient-centric, technologically advanced diabetes care, bridging the gap between research innovations and practical treatment solutions.(35)
CONCLUSION
Novel Drug Delivery Systems (NDDS) represent a significant advancement in the management of diabetes mellitus, addressing many of the limitations associated with conventional drug administration methods. These innovative platforms—such as nanoparticles, liposomes, microneedles, transdermal patches, and smart glucose-responsive systems—offer improved drug stability, controlled release, and enhanced patient compliance. By enabling targeted and sustained delivery, NDDS not only optimize therapeutic outcomes but also minimize side effects and dosing frequency. Despite these benefits, challenges such as large-scale production, regulatory approval, cost-effectiveness, and long-term safety must be overcome before their widespread clinical adoption. Future research focusing on integrating nanotechnology, biosensors, and artificial intelligence could pave the way for personalized and automated diabetes management systems. Overall, NDDS hold great potential to revolutionize diabetes therapy, shifting the focus from routine insulin administration toward more efficient, patient-friendly, and precision-based treatment approaches.
REFERENCES


Prerna Bahekar, Prerana Sahu, Gyanesh Kumar Sahu, Harish Sharma, Novel Drug Delivery System in Diabetes Mellitus: Current Trends and Future Prespective, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3435-3453. https://doi.org/10.5281/zenodo.18722382
 10.5281/zenodo.18722382
10.5281/zenodo.18722382
