Dr. Shivajirao Kadam College of Pharmacy, Kasabe Digraj, Sangli (MS), India. 416305
A chronic, progressive neurodegenerative illness, Parkinson's disease (PD) is characterized by the destruction of dopaminergic neurons in the substantia nigra pars compacta. This degeneration causes motor symptoms such bradykinesia, stiffness, tremors, and postural instability. As a multisystem condition, Parkinson's disease (PD) is becoming more well acknowledged for its substantial non-motor symptoms, which include mood swings, autonomic dysfunction, sleep issues, cognitive impairment, and sensory abnormalities. Its intricate pathophysiology includes oxidative stress, Lewy body formation, alpha-synuclein aggregation, mitochondrial dysfunction, and neuroinflammation, all of which are impacted by environmental and genetic variables (such as SNCA, LRRK2, and PARKIN mutations). Though familial types do exist, the majority of cases are idiopathic. Although research into biomarkers and neuroimaging is still ongoing, the diagnosis is still mostly clinical. Levodopa, dopamine agonists, and MAO-B inhibitors are used in current treatment to alleviate symptoms, in addition to non-pharmacological methods including physical therapy and deep brain stimulation. There are currently no cures or treatments that alter the condition, despite a great deal of study. In order to enhance patient outcomes, this study emphasizes the necessity of early diagnostic instruments and neuroprotective techniques.
Parkinson's disease (PD) is the second most common neurodegenerative ailment (after Alzheimer's), affecting roughly 10 million people worldwide. However, many instances may go untreated. As the population ages, the prevalence of Parkinson's disease is expected to roughly double in the next 25 years, posing a significant societal and economic burden for long-term treatment and care. [1]Until recently, the greatest reported prevalence rate was around 4%, indicating an increase with age. [2, 3] In 2006, WHO emphasized the global health burden of neurological disorders, estimating that they accounted for 6.3% of total DALYs? This was based on the Global Burden of Disease Study 2000, but it did not fully represent global epidemiology. Since then, older populations and better therapies have increased the prevalence and impact of many diseases. Vilariño-Güell et al. (2014) found that DNAJC13 mutations can lead to Parkinson's disease. [4] Parkinson's disease causes significant morbidity in the elderly, with DA neuron loss in the SNpc and basal ganglia degeneration being key features. Nonmotor symptoms often appear early, linked to olfactory and hindbrain changes, progressing to cortical areas in later stages. [5].Neuropsychiatric symptoms, particularly well-formed, non-threatening visual hallucinations, are a key clinical hallmark of DLB, although hallucinations are also common in Parkinson's disease, especially following l-DOPA treatment. Other common clinical features of DLB include delusions, violent or aggressive behavior, and increased sensitivity to neuroleptic medicines [6].Other common consequences include psychosis, delirium, and compulsive/impulsive spectrum disorders include impulse control disorders (ICDs), dopamine dysfunction sickness (DDS), and punding [9]
Parkinson's disease is characterized by cell loss in the substantia nigra, particularly in the ventral pars compacta. At the time of death, this region of the brain has lost 50-70% of its neurons relative to unaffected individuals. The earliest recognized pathogenic alterations in PD3H [7] Polymeropoulos et al. discovered a mutation in the SNCA gene that causes autosomal dominant Parkinson's disease back in 1997. This identified alpha-synuclein as a major component of Lewy bodies in sporadic occurrences. Gene duplications and triplications suggest its function in Parkinson's disease pathogenesis. [8] Mutations in the PARKIN and PINK1 genes cause early-onset recessive Parkinson's disease by affecting mitophagy, resulting in the buildup of damaged mitochondria. PARKIN affects PGC-1α, an important regulator of mitochondrial biogenesis and antioxidant defense. Reduced PGC-1α in sporadic PD implies mitochondrial abnormalities exist beyond rare hereditary instances.
Alpha-Synuclein Antibodies Used for Detecting Neuropathology
Braak and colleagues' staging of Parkinson's disease (PD) has been frequently utilized to follow the progression of Lewy pathology (LP) from the olfactory bulb or brainstem to the brain. The DLB consortium extended this by incorporating semiquantitative LP density grading. A unified staging method for Lewy body diseases (LBDs) takes into account motor, cognitive, and nigrostriatal abnormalities across ten brain areas. Alpha-synuclein (α-Syn) antibodies are important diagnostic indicators, with different epitopes targeting various LP types. Antibody selection is challenging, as some only detect α-Syn after specific pretreatments. Α-Syn aggregates affect cellular structures, including mitochondria, lysosomes, and nuclei, and may differ between diseases and brain regions.[10]
Α-Synuclein fibrils spread by attaching to neuronal surfaces and entering the cytoplasm. This process may require specialized receptors or protein changes. Researchers used Alexa-488 labelling to visualize fibril adhesion and internalization in primary hippocampus neurons. Trypan blue treatment identified intracellular fibrils short fibrils, anc Quantification revealed variable and oligomers, offering insight into the species most associated with Parkinson's pathology.

Figure 1: α-Synuclein fibrils adhere to the whole surface of neurons.
In α-synucleinopathy brains, certain neuronal types—like dopaminergic, noradrenergic, cholinergic, and glutamatergic neurons—show substantial α-synuclein aggregation, while GABAergic neurons remain essentially unaffected. Higher levels of α-synuclein may increase susceptibility at glutamatergic presynaptic terminals. However, sensitivity is not simply determined by neurotransmitter type; for example, SNc dopaminergic neurons are more vulnerable than those in the VTA. Limited stereological investigations reveal neuron loss even in the VTA, implying wider degeneration. [11]
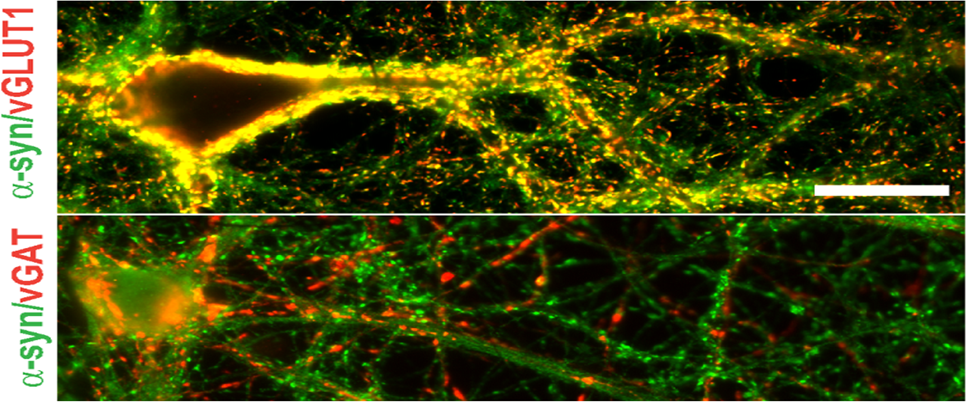
Figure 2: Colocalization of α-Synuclein with Excitatory and Inhibitory Synaptic Markers in Neuronal Cultures
Distribution of disease-
Parkinson's disease incidence ranges from 5 to more than 35 per 100,000 people each year, with rates increasing significantly with age. The prevalence rises from less than 1% between the ages of 45 and 54 to 4% in males and 2% in women beyond the age of 85. [12] Parkinson's disease mortality climbs after the first decade after diagnosis, and its frequency is anticipated to quadruple over the next 20 years, raising societal and economic consequences. . [12
Determinants of disease-
Most Parkinson's disease cases are the consequence of a combination of hereditary and environmental factors. While 5-10% are associated with specific gene mutations, frequent variants have incomplete penetrance, implying that additional factors play a role. Twin studies estimate heredity at only 30%, indicating a greater influence for environmental and lifestyle factors. [12]
Toxicant chemical exposure-
Pesticide exposure, farm work, and rural living have all been related to an increased risk of Parkinson's disease, with substances such as paraquat and rotenone connected to experimental parkinsonism. Genetic vulnerabilities in toxin processing may exacerbate this risk, indicating a gene-environment connection. Chlorinated solvents and PCBs, which are employed in numerous industries, have also been related to Parkinson's disease in human and animal research. . [12]
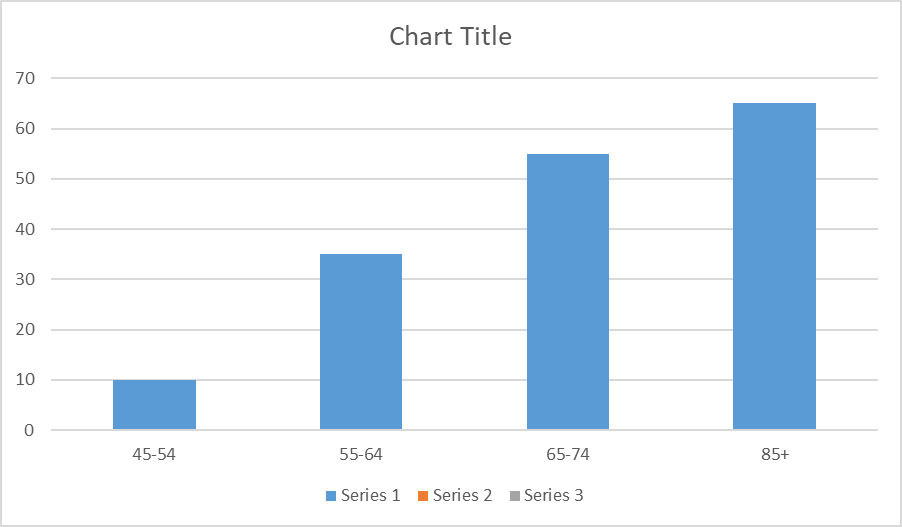
Figure 3: Annual incidence of Parkinson's disease ranges
Age
Although musculoskeletal pain may be expected in elderly Parkinson's patients, studies indicate inconsistent findings. Goetz et al. and Defazio et al. discovered that PD-related pain, particularly dystonia-related discomfort, frequently occurs in younger individuals, implying that it may not be entirely age-related. [13].
Gender
While current beliefs claim that there are no gender differences in Parkinson's pain, certain studies reveal that women are more likely to experience pain. Scott et al. discovered that women have more neck and low back pain, while Vela et al. discovered that women have lower pressure pain thresholds. This shows that women may have greater mechanical sensitivity in relation to musculoskeletal discomfort. [13]
Severity and duration of the disease
The effect of Parkinson's disease severity and duration on pain is debatable. Some studies associate pain with longer illness and greater severity, while others find no such link. [13]
Depression
Depression symptoms in Parkinson's disease patients range from minor to severe, with chronic pain raising depression risk in the elderly. Given the age and comorbidities of Parkinson's disease patients, a substantial relationship between pain and sadness is expected. Goetz et al. discovered that, while depression rates are comparable between patients with and without pain, those with pain have more severe depression symptoms. [13]
Systemic disease and pre-existing disturbances
Patients with pre-existing discomfort from illnesses such as diabetes or osteoporosis frequently continue to feel it after a Parkinson's diagnosis, with PD symptoms such as rigidity and cramping exacerbating the problem. Beiske and Defazio discovered that age-matched controls experience joint and neuropathic pain, implying that some pain may be caused by aging rather than Parkinson's disease. Additionally, some people reported pain prior to their Parkinson's diagnosis. [13]
Clinical spectrum
Parkinson's disease is characterized by different motor and non-motor symptoms such as cognitive impairment, sadness, and pain, all of which have a substantial influence on sufferers. Early diagnosis is difficult, frequently taking up to ten years, because first symptoms such as constipation, REM sleep behavior disorder, or hyposmia are nonspecific. Delays are more prevalent in individuals who do not have a tremor, have leg symptoms, or are younger, and general practitioners should not be held responsible for early missed diagnoses.
Diagnostic Criteria
The UK Parkinson's Disease Society Brain Bank (UKPDSBB) criteria diagnose Parkinson's disease in three steps: first, confirm parkinsonian syndrome with bradykinesia plus rigidity, rest tremor, or postural instability; second, rule out secondary causes such as stroke or medication side effects; and third, identify supportive features such as unilateral onset, levodopa responsiveness, and symptom progression. Bradykinesia is the central feature, which includes genuine slowness of movement, decreased movement amplitude (hypokinesia), and lack of movement (akinesia). These criteria establish an organized approach to accurate clinical diagnosis. [14] Autopsy confirms Parkinson's disease in 75-95% of clinically diagnosed cases, as complete assurance cannot be reached during life. Longer disease duration, professional experience, and breakthroughs in understanding Parkinson's disease all contribute to increased diagnostic accuracy. [15]After diagnosing Parkinsonism, the MDS-PD criteria will be used to determine if Parkinson's disease is the underlying cause.
To diagnose clinically established Parkinson's disease, the following are required:
Clinically plausible Parkinson's disease can be diagnosed as follows:
For example, if one red flag is present, at least one supportive criterion is required. If two red flags are present, at least two supportive criteria are needed. If more than two red flags are present, clinically probable Parkinson's disease cannot be identified. [15]
Early Medical Therapy
The American Academy of Neurology advocates beginning Parkinson's medication at the first signs of functional impairment, with options including levodopa, non-ergot dopamine agonists, and MAO-B inhibitors. Sinemet, which combines carbidopa and levodopa, is the most effective for motor symptoms, although it might cause dyskinesias if administered prematurely. Non-ergot dopamine agonists, such as Mirapex and Requip, cause less dyskinesias but have lower potency. Ergot-derived agonists are not first-line treatments due to the dangers of fibrosis and heart issues, which necessitate continuous cardiac monitoring if given. [16]
Late Medical Therapy
As Parkinson's disease worsens, initial therapies become less effective, resulting in motor problems such as dyskinesias and fluctuations. Patients have less "on time" while medicine manages symptoms and more "off time" when symptoms return. To lessen fluctuations, levodopa is coupled with non-ergot dopamine agonists (pramipexole, ropinirole) and apomorphine, which shorten off time. Monoamine oxidase-B and catechol O-methyltransferase inhibitors are also effective, however amantadine has only a moderate, short-term effect on dyskinesias. [16]
Tremor, stiffness, bradykinesia, and postural problems are all signs of Parkinson's disease. Resting tremor is the primary reason for consultation. It is of the distal and asymmetrical form, affecting one limb more intensively than the other and potentially compromising all four limbs. It is regular and has a low frequency (4–6 cycles per second). It is referred to clinically as "pill-rolling tremor," "adduction-abduction movement" of the fingers in the axis of the middle finger, "prono-supination movement" of the hands, or a combination of the three. [17]
Table 1: Classification of Motor and Non-Motor Symptoms in Parkinson’s disease
|
Motor symptoms |
Non motor symptoms |
|
Tremor, bradykinesia, stiffness, and postural instability. |
Cognitive dysfunction, bradyphrenia, and tip-of-the-tongue (word seeking) phenomena. |
|
Hypomimia, arthritis, dysphagia, and sialorrhea. |
Depression, fatigue, tiredness, and other behavioral and psychological issues |
|
Reduced arm swing, shuffling walk, festination, difficulties rising from chair, and turning in bed |
Sensory symptoms include anosmia, ageusia, discomfort (shoulder, back), and sensations. |
|
Micrographia, cutting food, feeding, hygiene, and slow daily tasks. |
The condition (orthostatic hypotension, constipation, urinary and sexual dysfunction, abnormal sweating, seborrhea), and weight loss. |
|
Glabellar reflex, blepharospasm, dystonia, striatal deformity, scoliosis, or camptocormia |
Sleep disturbances (REM behavior disorder, bright dreams, daytime sleepiness, sleep fragmentation, restless legs syndrome) |
Bradykinesia
Bradykinesia, or sluggish movement, is a feature of Parkinson's disease (PD) and a diagnostic clinical symptom. It includes difficulty in planning, initiating, and executing motions, as well as performing sequential and concurrent tasks. Barbeau (1981) coined the words bradykinesia, hypokinesia, and akinesia to describe different levels of motor dysfunction. Gibb and Lees (1988) described bradykinesia as a slow initiation of voluntary movement with a gradual reduction in the speed and amplitude of repetitive motions. [19]
Physiology of Bradyk1nesia
The Peter Bent Brigham Hospital Human Studies Committee authorized a study in which 19 Parkinson's patients (12 men, 7 women; ages 47-82) and 11 healthy individuals (6 men, 5 women; ages 30-83) gave their informed consent. Patients had varied levels of disability and therapies, whereas controls experienced common illnesses such as back pain. Rapid elbow flexion of the dominant arm was investigated in both groups. [20]
Tremor
Tremor is one of the main motor symptoms of Parkinson's disease (PD), occurring in around 75% of patients and is commonly present at illness onset. Tremor in Parkinson's disease is generally seen in rest with a frequency of 4-6 Hz and typically affects the upper limb but may also occur in other body parts such as the lower limb, chin, mouth, or tongue. Tremor is a highly heterogeneous symptom: it may range from mild to severe manifestations, is highly sensitive to stress.[21]Patients often report worsening tremors during stressful situations .This can lead to stigma and embarrassment, creating a cycle of negative behavior. Tremor also spontaneously ‘waxes and wanes’. Making it a symptom that both patients and clinicians cannot predict. Uncertainty surrounds the brain processes that underlie both the spontaneous fluctuations in tremor and its amplification during stress. In order to address this problem, we investigate whether acute cognitive stress affects how levodopa affects resting tremor. [22]Second, some Parkinson's disease patients experience postural/kinetic tremors and rest tremors of different frequencies; the postural/kinetic tremor has a higher frequency (41.5 Hz) and is not harmonically connected to the resting tremor. 510% of Parkinson's disease patients have this type. [23]
Pathology of parkinsonian tremor-
The loss of dopaminergic cells in the substantia nigra and the ensuing dopamine depletion of the striatum are the pathologic hallmarks of Parkinson's disease. The question of whether tremor-dominant PD and akinesia/rigidity-dominant PD have different pathologies emerges. In the tremor-dominant form, dopaminergic cell degeneration mostly affects the medial sub-stantia nigra, particularly the retrorubral area A8, while the lateral substantia nigra (A9) is more extensively damaged in the akinetic stiff variant. [24]
This suggests that tremor is connected with cell death in the retrorubral substantia nigra.
However, other nuclei, such as the locus coeruleus, are more affected in the akinetic stiff variantLouis and colleagues discovered pathologic abnormalities in autopsied brains of patients with clinically diagnosed essential tremor, contradicting Rajput et al.'s observations .ET(essential tremor) patients' brains exhibit pathological abnormalities such as reduced Purkinje cells (PCs), increased axonal swellings (torpedoes), and other alterations.[25]
Tremor, the first movement disorder documented, has been addressed in medical literature with varying nomenclature since Hippocrates' writings (1). The term "tromos" comes from the Proto-IndoEuropean root *ter-, which means "to shake" and "to fear." It retained its dual meaning in Sanskrit and ancient Greek after undergoing a syllabic metamorphism: =lfr (trasat), sqE~lx (TR~emo, to tremble or shake), and sq?lo1 (tromos, shaking caused by great fear). In Latin, the *ter- root was maintained to denote dread (terreo), but the *tre- metathesis referred to the involuntary movement of tremors. [26]
Postural Instability-
Background
In Parkinson's disease, balance impairment and postural instability significantly impact quality of life.Physiotherapy may reduce impairment by treating balance dysfunction and postural instability.This comprehensive review and meta-analysis evaluated the effectiveness of traditional physiotherapy therapies in treating balance dysfunction and postural instability in individuals with idiopathic Parkinson's disease. [28]
Definition
Parkinson's disease (PD) frequently causes postural instability (PI), which becomes a clinical concern in the latter stages of the disease. [29]Postural instability is common in Parkinson's disease, with demonstrated changes in postural control methods during standing tasks. [30]
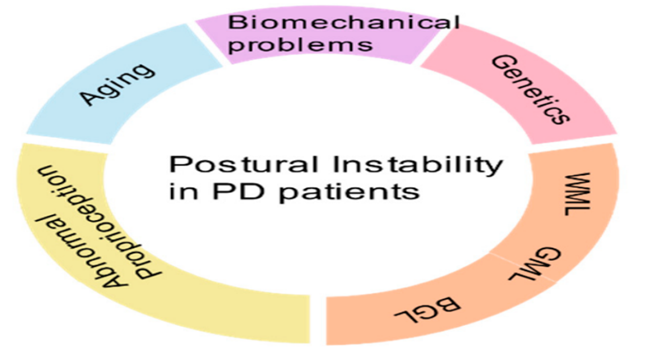
Figure 4: Factors Affecting of Postural Instability
Factors Affecting Postural Instabillity
The majority of PI signs and symptoms are nonspecific. As a result, delays in diagnosis and misdiagnosis occur, which can be avoided by more aggressive and early investigations.Identifying PI-specific risk factors will aid in effective diagnosis and distinguishing modifiable from nonmodifiable ones, hence promoting prevention. While age, genetic mutations, and race cannot be changed, environmental influences, lifestyle modifications, chemical exposures, and stress can.Measuring the components may aid in the successful screening and tracking of illness changes. [27]
Aging is a complex process that involves gradual physiological deterioration, increasing susceptibility to sickness and death. It varies among species, people, and even tissues, according to Miller (1999), Takubo et al. (2002), and de Magalhaes & Costa (2009). Aging is explained by two primary theories: damage-based (accumulated tissue damage) and programmable (genetic regulation). According to the multifactor hypothesis, aging is caused by a long-term imbalance between cellular damage and repair. [31]Decreased sensory motor function in the elderly might lead to greater anxiety and frequency of falls, reducing independence.Falls in elderly is a major cause of morbidity and mortillity [32] the control of the posture is maintained by a complex central sensorimotor system which integrates information from the vestibular, visual, and somatosensory systems. [33]
The development of sporadic Parkinson's disease is likely caused by a complex combination of hereditary and environment-related factors.[34] Reduced Parkinson's disease (PD) risk among cigarette smokers, with strong evidence for inverse dose–response gradients, has been demonstrated consistently.[35]Active smokers have a 50% decreased risk of Parkinson's disease compared to those who never smoked. The risk of Parkinson's disease (PD) reduces with longer smoking duration and increases with time following quitting.[36]various sclerosis has various causes; both hereditary and environmental factors increase the likelihood of developing the condition.[37]The link between smoking and secondary progression is unclear, with some research indicating a greater risk and others showing no effect.[38]Numerous environmental contaminants have been linked to the start of Parkinson's disease, however research is conflicting. According to certain studies, Parkinson's disease incidence may be connected to occupational chemical exposure. [39]A combination of genetic and environmental variables may impact the beginning of human disease by structurally modifying deoxyribonucleic acid (DNA). Caffeine, for example, is an adenosine A2A (ADORA2A gene) receptor antagonist that promotes dopamine neurotransmission, and ADORA2A polymorphisms have been reported to lessen the incidence of Parkinson's disease. [39]
Since the discovery of the first gene for Parkinson's disease (PD) 20 years ago, other genes have been linked to PD or illnesses with Parkinsonism. Genetic testing for young-onset, inherited, or unique Parkinsonian illnesses is already common practice in healthcare settings. [40]
Approximately 1% to 2% of those over 65 suffer with Parkinson's disease (PD). Parkinsonism that resembles idiopathic Parkinson's disease (PD) can be caused by mutations in five different genes: SNCA (α-synuclein), PARK2 (parkin), PARK7 (DJ-1), PINK1, and LRRK2.Leucine-rich repeat kinase (LRRK2) is a 51-exon, multidomain protein that is encoded by LRRK2. Mutations in LRRK2 result in autosomal dominant Parkinson's disease (PD), which often manifests as α-synuclein-type neuropathology in most cases.[41]Numerous other genes have been proposed as monogenic origins of Parkinson's disease (PD) or illnesses with Parkinsonism as a more or less prominent clinical feature since the initial gene for PD was discovered 20 years ago.[42]The LRRK2 G2019S mutation and GBA mutations are two of the most prevalent genetic changes linked to an elevated risk of Parkinson's disease (PD).These mutations are especially prevalent among the Ashkenazi-Jewish population . Mutations in the GBA gene, which encodes the lysosomal enzyme β-glucocerebrosidase, can result in type I, II, or III. Gaucher's disease. [43]Gaucher's illness is the most common glycolipid storage condition. [44]LRRK2 gene mutations are a prevalent cause of late-onset, autosomal dominant familial Parkinson's disease (PD; PARK8, OMIM #607060), with a clinical and neurochemical pattern that is virtually indistinguishable from idiopathic disease. [45]
Nutrients that may be associated with increased risk or progression of Parkinson's disease:
Dairy Products-
Milk and dairy consumption may raise the incidence of Parkinson's disease (PD), notably in men, regardless of calcium intake (Hellenbrand et al., 1996b; Chen et al., 2002, 2007a). Dairy consumption has also been linked to a higher incidence of Parkinson's disease in women (Saaksjarvi et al., 2013). Higher dairy consumption is linked to decrease blood uric acid levels, which are negatively connected to PD risk and development (Weisskopf et al., 2007; Shen et al., 2013). Urate's neuroprotective impact appears to be more significant in men, with less evidence in women (GAO Et Al., 2008; O'Reilly et al., 2010). [46]Diary consumption is linked to insulin resistance. Research suggests that Parkinson's disease and other neurodegenerative disorders represent a type of "type III diabetes". [47]Vitamin D's active form, 1, 25-dihydroxyvitamin D3 (1, 25(OH) 2D3), is a pluripotent steroid with physiological activities beyond calcium homeostasis and bone metabolism (Jones et al., 1998). [48]Supplementing with vitamin D and calcium can lower the incidence of hip fractures and other nonvertebral fractures among the elderly. [49]
Nutrients that may be Associated with a Decreased Risk or Progression of PD:
Phytochemicals
Polyphenols, terpenoids, flavonoids, ascorbic acid, alpha-tocopherol, catechins, and beta-carotene may provide neuroprotection and slow the progression of Parkinson's disease, according to recent studies.[50]The brain has a high oxidative capacity but limited ability to combat oxidative damage.Oxidative stress is linked to neuronal cell injury in numerous brain pathologies, including vitamin E, beta-carotene, and supplements. Although the mechanism of action is unclear and clinical trials are limited, AOX have shown promise in slowing the progression of neurodegenerative disorders like Alzheimer's, Parkinson's, Huntington's, amyotrophic lateral sclerosis, and ischaemic stroke. [51]
Caffeine
It is unknown whether caffeine can lessen the risk of Parkinson's disease and stop its progression. In large-scale cohort studies, caffeine use was inconsistently associated with a low risk of Parkinson's disease during the follow-up.[52]Our study demonstrated a slight negative correlation between coffee consumption and the probability of Parkinson's disease. A study indicated that those who drank at least 10 cups of coffee per day had a considerably decreased risk of Parkinson's disease compared to non-drinkers.[53].Even after controlling for confounding factors, the results remained consistent. We created internal RT-m/z libraries for HILpos and C18neg modes, which included caffeine and its principal metabolites. To expand coverage, we used in silico cheminformatic analysis to annotate all probable metabolites implicated in caffeine metabolism. [54]
Omega-3 (DHA)
Global life expectancy is growing , and the prevalence of age- and lifestyle-related noncommunicable diseases (NCDs), such as cancer, heart disease, lung disease, type 2 diabetes, obesity, chronic kidney disease, and dementia, is rising.
The Relevance of Mechanisms of Action of DHA-DHA and EPA appear to act via overlapping, but unique, mechanisms of action, affecting cellular function to promote overall health and wellbeing, as well as to lessen the risk and severity of disease; these mechanisms are described in depth elsewhere. [55] Omega-3 long-chain polyunsaturated fatty acids (n-3 FAs) promote brain growth and may protect against neurodegenerative illnesses such as Parkinson's and Alzheimer's. EPA and DHA, which are found in fatty fish such as salmon, mackerel, and tuna, have been shown to protect against mood disorders. ALA, another n-3 fatty acid, is found in vegetable oils and green vegetables such as kale and spinach.[56]Omega-3 LCPUFAs and Cognitive Decline and Dementia-Although DHA plays a structural role as a key component of neuronal membrane fatty acids, it is endogenously converted in the nervous system into an endocannabinoid-like metabolite known as N-Docosahexaenoylethanolamine (synaptamide). Synaptamide enhances neurogenesis, neurite outgrowth, and synaptogenesis in developing neurons primarily via the G-protein coupled receptor GPR110.GPR110 stimulates cAMP synthesis and phosphorylation of protein kinase A (PKA) and the cAMP response element binding protein (CREB).[57]Omega-3 fatty acids are vital nutrients. Docosahexaenoic acid (DHA, 22:6n-3) is an omega-3 fatty acid found in the brain and plays a substantial role in brain development, cognitive function, and memory function (2-5). However, the molecular processes behind this positive effect are not fully known. [58]
Soy (Genistein)
Soy is one of the eight major dietary allergens, with proteins including glycinin and β-conglycinin known to cause allergic reactions. Other ingredients, such as protease inhibitors and whey fractions, may potentially contribute to soy allergies. Breeding and genetic engineering may help lower soy allergens for safer consumption...[59]Soybean (Glycine max L. Merrill) originated in China and is an economical legume utilized globally as a key source of vegetable protein and oil.[60]
Tea
Research on the protective effects of coffee and tea on Parkinson's disease is limited, compared to cigarette smoking. Several writers suggest various mechanisms for the protective effect. Caffeine has been shown to reduce the loss of striatal dopamine and dopamine transporter binding sites caused by MPTP in mice, supporting a direct cause-effect relationship. [61]
Alcohol
Another age-related prevalent neurodegenerative disease, Parkinson's disease (PD), is defined by a constellation of clinical signs, which include slowness of movement, rest tremor, rigidity, and postural instability.[62]In our patient cohort (mean age at diagnosis, 66.9 years; average disease duration at enrollment, 2.1 years; and 5.3 years of follow-up), we found that prediagnosis consumption of caffeinated coffee, tea, and moderate alcohol, as well as physical activity, protect against disease progression.[63]
White matter hyperintensities (WMH) on FLAIR MRI are predominantly associated with small-vessel disease in the brain's subcortical areas and increase with age and cerebrovascular risk factors. WMH has been linked to a higher incidence of cognitive decline and dementia in the elderly (Debette and Markus, 2010).[64] White matter hyperintensities (WMH) on T2-weighted and FLAIR MRI have been linked to cognitive deficits in the elderly, including memory and executive function.[65]The Leukoaraiosis and Disability (LaDis) study discovered that the presence of wMLs in nondisabled senior persons was associated with a history of falls, as well as mobility impairments such as lower walking speed, balance, and physical activity levels.[66]WMHs have a high correlation with age, hypertension, and diabetes, suggesting a vascular etiology.[67]Cognitive impairment is typical in Parkinson's disease, ranging from moderate cognitive impairment to dementia. Dementia is a late-stage condition, whereas MCI is prevalent in the early stages. [68]. Structural MRI in idiopathic Parkinson's disease (PD) typically seems normal, but it is utilized to rule out secondary causes such as vascular lesions and identify atypical parkinsonisms, such as the hot-cross sign found in multiple system atrophy (MSA-C).[69]WMHs may contribute to depressed symptoms in cases where the first occurrence of depression is late in life.[70]
Parkinson's disease (PD) patients are characterized as either tremor dominant (TD) or postural instability gait difficulty (PIGD), with PIGD being associated with more cognitive impairment and gait abnormalities. The neurological cause for these symptom disparities is unknown, however gray matter (GM) atrophy may be a factor. GM atrophy is linked to aging, cognitive decline, and delayed walking. However, due to its low sensitivity, visual assessment of GM alterations may fail to properly identify PD subtypes...[71] Voxel-based morphometry (VBM) is an unbiased whole-brain MR approach that may detect regional changes in brain tissue composition, such as gray matter (GM) and white matter.[72]
Over the last 30 years, there has been a significant advancement in imaging brain anatomy and function. This has led to insights into illness causation, consequences, and healthy basal ganglia function. [73] Dopamine depletion causes functional alterations in the basal gangliacircuitry, contributing to the development of Parkinson's disease [74]
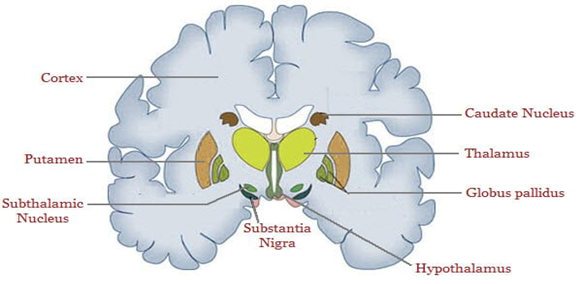
Figure 5: Basal Ganglia
Movement disorders, ranging from hypokinetic Parkinson's to hyperkinetic Huntington's, are caused by anomalies in the basal ganglia-thalamocortical motor circuit. [75]
James Parkinson accurately defined both motor and non-motor symptoms of Parkinson's disease, which resulted in breakthroughs in diagnosis and therapy. According to research, nonmotor symptoms such as sadness and sleep difficulties have a significant impact on quality of life, institutionalization, and healthcare expenses...[76] NMS has a negative impact on patients' quality of life and can lead to institutionalization in advanced disease stages [77] Non-motor symptoms can be more disabling than motor dysfunctions and do not respond to dopaminergic medication. Evidence suggests that Parkinson's disease can affect neurotransmitters other than dopamine, including serotonergic, noradrenergic, and cholinergic systems. [78]
Autonomic Dysfunction
Autonomic dysfunction is a significant non-motor characteristic of Parkinson's disease (PD).[80] Synucleinopathies are neurodegenerative illnesses caused by aberrant accumulation of misfolded phosphorylated α-synuclein (αSyn) in neurons, glia, or both resulting in autonomic nervous system dysfunction.
Evidence suggests that aberrant αSyn spreads through cells similarly to prions. Strains refer to different forms of αSyn assemblies with distinct structural features. [79]
Constipation
Constipation, caused by autonomic dysfunction, is one of the most researched prodromal symptoms of Parkinson's disease. [81] Parkinson's disease (PD) patients suffer constipation and defecatory dysfunction at a 2-3 times higher rate than non-PD patients.[82] Chronic constipation patients may have altered relaxation of the striated pelvic floor and anal sphincter musculature, resulting in functional blockage of defecation at the pelvic outlet. Anismus, also known as spastic pelvic floor syndrome, is a condition with unknown underlying causes. [83] PD-related constipation can be caused by Lewy body deposition in the enteric nervous system or the dorsal motor nucleus of the vagus nerve, which are among the first affected sites. [84] Severe constipation can occur at any stage of Parkinson's disease, including before motor symptoms appear, and it is frequently treatment-resistant. It may because difficulties like as megacolon, pseudo-obstruction, or volvulus. A 12-year study found that people who had infrequent bowel movements were up to 4.1 times more likely to acquire Parkinson's disease. [85] Various measures have been validated to assess nonmotor impairment in Parkinson's disease, including questions on autonomic function. [86] PD has been associated with intestinal anomalies, such as megacolon, caused by pseudo blockage. [87]
Urinary Problem
Lower urinary tract symptoms (LUTS) are prevalent in Parkinson's disease (PD), affecting 27-85% of patients. [88] The lower urinary tract consists of the bladder and urethra. The bladder contains muscarinic M2, M3, and adrenergic β3 receptors. It is regulated by parasympathetic (cholinergic) fibers for contraction and sympathetic (noradrenergic) fibers for relaxation. [89]
Urinary dysfunction symptoms include urgency and incontinence, as well as dysuria and prolonged micturition. [90] Bladder regulation involves both the somatic and autonomic neural systems. During filling, sympathetic efferents from the hypogastric nerves increase muscular compliance, bladder distension, and sphincter closure. [91]
Orthostatic Hypotention
In severe Parkinson's disease (PD), non-motor symptoms may be the primary cause of impairment. Orthostatic hypotension (OH) is one of Parkinson's disease's non-motor symptoms. The condition is believed to be caused by degeneration of the peripheral autonomic nerve system during the illness progression. [92] Orthostatic hypotension affects 10% to 30% of older people.[93] Orthostatic hypertension (OH) is more common in children aged and is linked to higher rates of morbidity and death.[94Orthostatic hypotension (OH) occurs when blood pressure drops by at least 20 mm Hg systolic or 10 mm Hg diastolic within three minutes of standing. It is a symptom, not a disease, indicating poor blood pressure regulation. A decline detected at a head-up tilt of ≥60 degrees is a valid alternative diagnostic technique. [95] The term "orthostatic dizziness" describes vertigo or dizziness that happens as one rises from a supine position to a sitting or standing position, or from a sitting position to a standing one. [96]
Sexual Dysfunction
Sexual dysfunction, including erectile and ejaculatory difficulties, is common early in the course of synucleinopathies... [97] Sexual function is crucial for both species survival and human well-being. [98] Dopaminergic mechanisms may contribute to libido and arousal-induced vasodilation of penile erectile structures. Up to 79% of men with Parkinson's disease report impaired sexual function, including erectile dysfunction, ejaculation issues, and difficulty achieving orgasm. [99] Sexual dysfunction (SD) is often overlooked, despite its significant impact on well-being. Despite societal stigma, studies show that SD affects up to 80% of male and 85% of female PD patients, which is much greater than age-matched controls. [100]
Sleep disorders
Sleep issues are a commonly recognized source of disability in Parkinson's disease (PD) sufferers. However, since a report of 'sleep attacks' in patients with Parkinson's disease taking dopaminergic drugs was published,[101] Sleep difficulties are frequent in both the general population and people with Parkinson's disease, with an estimated prevalence of 60-70%. Sleep difficulties in Parkinson's patients can significantly reduce their quality of life due to a variety of factor. [102
Insomnia
Insomnia symptoms are the most common cause of sleep problems in Parkinson's disease patients.[103] Insomnia is the most common sleep disorder in Parkinson's disease patients, accounting for 36.9% of cases and ranging from 27 to 80% [104] Insomnia is defined as nightly symptoms of insufficient sleep or restlessness following a regular sleep pattern.[105]
Dopaminergic therapy
Hornykiewicz introduced dopaminergic treatment in 1970, using L-Dopa, the predecessor of DA. L-Dopa therapy is still the preferred treatment for Parkinson's disease after four decades of widespread use. Its main benefits are its low cost and ability to cross the blood-brain barrier after converting to DA. In the early stages of Parkinson's disease, L-Dopa can alleviate motor symptoms such akinesia, bradykinesia, rigidity, and partial reaction to tremors. This period is also referred to as the L-Dopa "honeymoon".
L-Dopa is the only medicine that has been shown to increase life expectancy. [106] during treatment for Parkinson's disease, non-motor symptoms such hallucinations, cognitive impairment, and orthostatic hypotension may also occur. After 5 years of L-Dopa treatment, roughly 50% of patients experience worsened "wearing off" or "on-off" swings and dyskinesia. L-Dopa has been linked to increased neuronal degeneration through oxidative metabolism but this is still debated. [106]
Monoamine oxidase-B (MAO-B) inhibitors
The University of Minnesota developed Rasagiline, a new MAO-B inhibitor. It is currently being investigation to potentially slow the progression of Parkinson's disease.
It has somewhat different qualities than selegiline and effectively alleviates Parkinson's disease symptoms.
Its potential as a supplement to levodopa therapy is also being studied. Researchers are exploring how Rasagiline might be coupled with functional moieties to create a novel bifunctional molecule. It was proposed to introduce a carbamate cholinesterase (ChE) inhibiting moiety to achieve this. [107]
Figure 6: Chemical structure of melatonin, 3-(2-acetylamino-ethyl)-1H-indol-5- ol anion.
Dopamine agonists
Dopamine agonists (DA) activate DA receptors directly, skipping the presynaptic production of DA. Research indicates that activation of D2 receptors is crucial for the favorable antiparkinsonian effects of DA agonists, but concomitant D1 activation is also necessary.
D2 stimulation is essential to provide the best physiological and behavioral results.Pramipexole has been proven to be a safe and effective medicine when used as monotherapy in the early stages of Parkinson's disease. Ropinirole has been shown to be useful in treating early PD. In Clinical In practice, dosages up to 24 mg may be required for best results. [108]
CONCLUSION
Parkinson's disease (PD) is a complex neurological illness that significantly impairs patients' quality of life and is characterized by both motor and non-motor symptoms. Its pathogenesis, which is impacted by both environmental and hereditary factors, is primarily caused by the formation of alpha-synuclein aggregates and the gradual death of dopaminergic neurons in the substantia nigra. There is presently no cure or disease-modifying treatment, and diagnosis is still mostly based on clinical observation despite tremendous advancements in our knowledge of the disease processes. Dopamine replacement therapy and supporting measures including deep brain stimulation and physical therapy are the mainstays of treatment, which is still symptomatic. There is optimism for future advancements due to research on early indicators, neuroprotective drugs, and the impact of diet and lifestyle. As the prevalence of Parkinson's disease (PD) rises worldwide, comprehensive approaches that combine early diagnosis, focused treatment, and individualized care are desperately needed to control symptoms and enhance patients' long-term results.
ACKNOWLEDGEMENT
We would like to express our heartfelt gratitude to all those who supported and guided us throughout the completion of this article. First and foremost, we sincerely thank Dr. Shivajirao Kadam College of Pharmacy for providing us with the necessary facilities and a conducive academic environment. We are deeply grateful to all the faculty members of the institution for their constant encouragement, valuable suggestions, and continuous support during the preparation of this work. We would also like to extend our special thanks to our mentors and guides for their insightful guidance, motivation, and constructive feedback, which helped us improve the quality of our work. This article is a collaborative effort by the following authors: Vaishanvai Kolekar, Avadhut Khot, Manali Bavadekar, Vedika Shinde, Tejaswini Bhosale, Mayuri Kalokhe, Shraddha Jadhav, Sairaj Kattekari, Yash Kulkarni.Their dedication, teamwork, and commitment to research have been instrumental in the successful completion of this article.
REFERENCES








Vaishanvai Kolekar, Avadhut Khot, Manali Bavadekar, Vedika Shinde, Tejaswini Bhosale, Mayuri Kalokhe, Shraddha Jadhav, Sairaj Kattekari, Yash Kulkarni, Multisystem Neuropathology of Parkinson’s Disease: A Convergence of Synucleinopathy, Neuroinflammation, And Dopaminergic Demise, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1161-1183. https://doi.org/10.5281/zenodo.16801148
 10.5281/zenodo.16801148
10.5281/zenodo.16801148
