Department of Pharmaceutics, Yashwantrao Bhonsale College of Pharmacy, Sawantwadi, Maharashtra, India.
Periodontitis is a chronic inflammatory disease that affects the supporting structures of the teeth, leading to tissue destruction and tooth loss if left untreated. Conventional treatments for periodontitis, such as scaling and root planing , may be limited in effectiveness, particularly in cases of advanced disease or in the management of infections within deep periodontal pockets. In recent years, in situ gel systems have emerged as a promising novel approach for the local delivery of therapeutic agents directly to the site of infection, offering numerous advantages over traditional methods. These gels are unique in their ability to transition from a liquid to a gel upon contact with the oral cavity, providing a sustained release of antibiotics or anti-inflammatory drugs, thereby enhancing treatment outcomes and minimizing systemic side effects. This review explores the potential of in situ gels in the management of periodontitis, focusing on their composition, mechanism of action, and efficacy in delivering active pharmaceutical ingredients. The review also highlights various biocompatible polymers used in the formulation of in situ gels, and their role in ensuring controlled drug release and therapeutic efficacy. Additionally, challenges related to patient compliance, gel stability, and scalability for clinical application are discussed. Overall, in situ gels represent a promising therapeutic strategy in the localized treatment of periodontitis, offering a targeted, effective, and minimally invasive alternative to conventional periodontal therapies. The characterisation of oral in situ gels, encompassing several evaluations including drug content study, pH & viscosity determination, texture analysis, spreadibility, gel strength, gelling time, sterility testing, in-vitro drug release study, stability study, etc., is finally summarized in this review. Experimental data indicates that in situ gel forming systems may be helpful in treating a number of common oral cavity illnesses, according to the reviewed literature. Clinical studies should be the main focus of future research if the in situ gel is to significantly reduce periodontitis.
The transitional condition between the solid and liquid phases is called gel. The liquid phase is immobilized by the solid component's three-dimensional network of interconnected molecules.[1] After the formulation is administered to the site, a process known as "in situ gelation" occurs, where a gel forms at the site of action. Based on a liquid medication formulation solution, the in situ gel phenomenon transforms into a semi-solid mucoadhesive important depot.[2] Drugs can now be administered to patients in a liquid dose form using in situ gel forming formulations, which provide a sustained release of the medication for the intended amount of time. Various polymer-based delivery systems have been developed that can extend the formulation's residence time at the drug's absorption site.[3] In the buccal cavity, its mucoadhesive quality also keeps saliva from washing it away. Water-soluble polymers with gel-forming properties that can be applied to a delivery location have garnered more attention recently. Water-soluble polymers with gel-forming properties that can be applied to a delivery location have garnered more attention recently. Unlike very strong gels, these so-called in situ gelling polymers are simply delivered in liquid form to the site of drug absorption, which makes them a particularly favourable alternative to other polymers. They swell at the drag absorption site to create a robust gel that can extend the active ingredient's residence duration. Because of their excellent biocompatibility, solute permeability, and adjustable release properties, gels three-dimensional networks of polymeric materials have drawn a lot of interest in the biomedical domain as drug, protein, and cell transporters.[4] The feature that compromises the surrounding tissues and promotes good biocompatibility is their capacity to hold a significant quantity of water within their structures, which results in a high water content and soft-surface qualities.[5-7] A group of issues known as periodontal disease occur in the sulcus, the space between the gums and teeth. Actinobacillus and actinomy cetemcomitans are common pathogens that cause juvenile periodontitis, while staphylococci subspecies epidermidis and aureus are responsible for adult periodontal disease.[8] Three potential benefits of site-specific therapy for periodontitis include lower medication dosages, higher drug concentration at the infection site, and fewer systemic side effects such gastrointestinal upset.[9] The goal of treating periodontal illnesses with a localized drug delivery system is to minimize the negative effects of systemic medication administration while simultaneously providing the therapeutic agent at a level that is adequate inside the periodontal pocket. Consequently, it improves patient compliance.[10]
Periodontitis
Etiology of periodontitis[11-13]
Periodontal disease is caused by the proliferation of bacteria and spirochetes, among other pathogens. Tooth loss occurs in periodontal disease. The clinical indicators used to gauge the effectiveness of the illness include the plaque index (PI), gingival index (GI), probing pocket depth (PPD), and clinical attachment level (CAL). The primary source of microbial feeding is the probing pocket depth (PPD).

Fig No: 1 Normal tooth and periodontitis
Teeth with periodontitis eventually lose their ability to function or suffer damage as a result of the disease's on going progression. The etiology of periodontal disease is known to be influenced by the bacterial flora found in the gingival crevice. When gingival and teeth are in good health, there is a 2 mm gap between them. The sulcus depth is typically greater than 5 mm when periodontitis and other bacterial collagenase enzymes are present. The condition of infectious disease at the location of nuclear cell polymorphisms caused by the anti-inflammatory reaction. and may aid in halting tooth loss. There is intriguing data from a recent study regarding a number of significant systemic disorders and periodontal infections. Theoretically, systemic health impacts from periodontal disease may be predicted using one or more of numerous approaches. Infection spreads directly to the periodontium from deep and nearby tissue (brain, sinus infection, facial, or aircraft). The work is impacted by circulating inflammatory mediators in the periodontium passage from distant places (atherosclerosis). Oral bacteria can penetrate infections through distant areas in the systemic circulation, such as endocarditis and thrombosis/atherosclerosis. Conditions like gastrointestinal or pulmonary infections encourage or contribute to oral bacteria's dissemination of their products or host products to distant mucosal locations. The teeth are surrounded by a 1 mm broad gingival border and a tight collar of healthy gingival tissue. The gingival margin creates the sulcus, or external wall crevice. A little crevice emerges between the tooth and the gingiva. The gingival sulcus is never totally devoid of microorganisms, and there is a small amount of microflora that is primarily composed of aerobic bacteria that are both analogous to tissue and work in harmony with the host's defense system. Periodontal pathogens grow only and only when environmental and nourishes and their requirements, 3.5 mL/day or more in diseased condition. Firstly a rise in the number of gingival aerobic bacteria, then a shift in the composition of the micro flora is observed with the development of periodontal disease.
Mechanism Of Periodontitis-Induced Tooth Loss
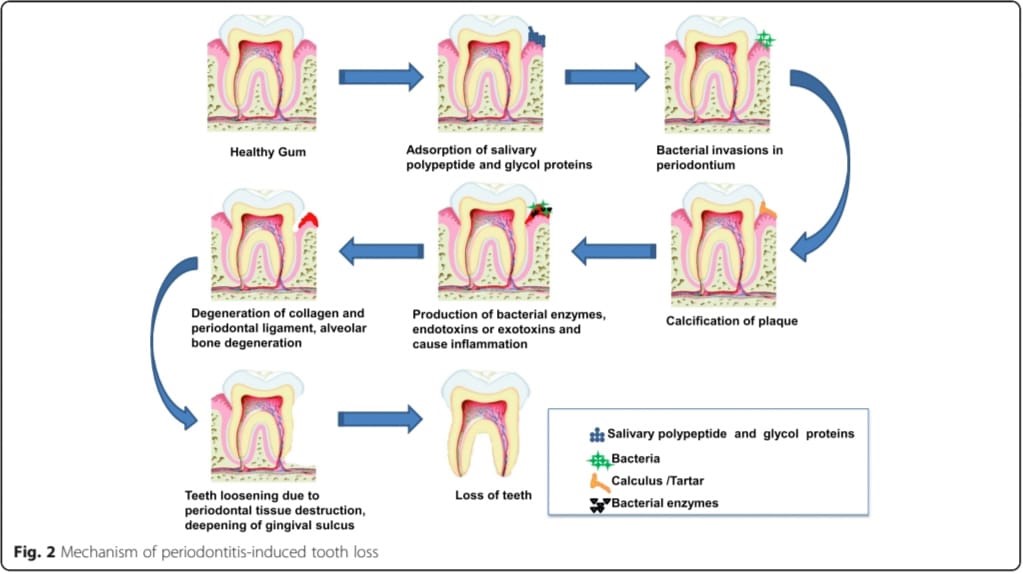
Fig No: 2 Mechanism of periodontitis-induced tooth loss
Periodontal Infection [14,15]
When bacteria and other pathogens infiltrate the pocket, proliferate there under ideal conditions, and reduce the clinical attachment level (CAL), probing pocket depth (PPD), and other parameters, periodontal diseases result.
Numerous factors, such as the introduction of pathogens or an imbalance in the native flora, can result in dental infections. The elevated levels of pro-inflammatory substances and cytokines demonstrate that the systems controlling these genes are broken in periodontitis.
Infections are caused by organisms that are antibacterial and antiprotozoal. Numerous causes, including the invasion of pathogens, the alteration of the balance of native flora, and the invasion of germs by various ways, are accountable for periodontal infections.
People with Down syndrome, Chediak-Higashi syndrome, and Papillon-Lefevre syndrome are more susceptible to severe periodontitis. Periodontal disease, which also affects humoral immunity and cell-mediated immunity, is caused by a change in humoral immunity. In children with Chediak-Higiashi syndrome, the periodontal disease presents as early-onset periodontitis. The hallmark of Down syndrome is widespread, severe periodontitis. Early tooth loss is a Papillon-Lefevre symptom of periodontitis
Types Of Periodontitis [16-17]
i. Mild periodontitis
Teeth with gingivitis have a spongy, glossy, mushy, red, and enlarged surface. The bacteria in plaque produce toxins that irritate the gums. A patient with gingivitis will have a 3 mm pocket depth.
ii. Moderate periodontitis
More bone and tissue are lost, and deeper pockets occur as a result. probing pocket depth (PPD) of this kind is 5 mm, and bacteria or other pathogens cause tissue injury.
iii. Advances periodontitis
Up to 6 mm is the probing pocket depth (PPD) for this primary form of periodontitis. Additional tooth damage could cause them to be destroyed.
iv. Refractory periodontitis
Permanent tooth loss and damage occur in cases of periodontitis.
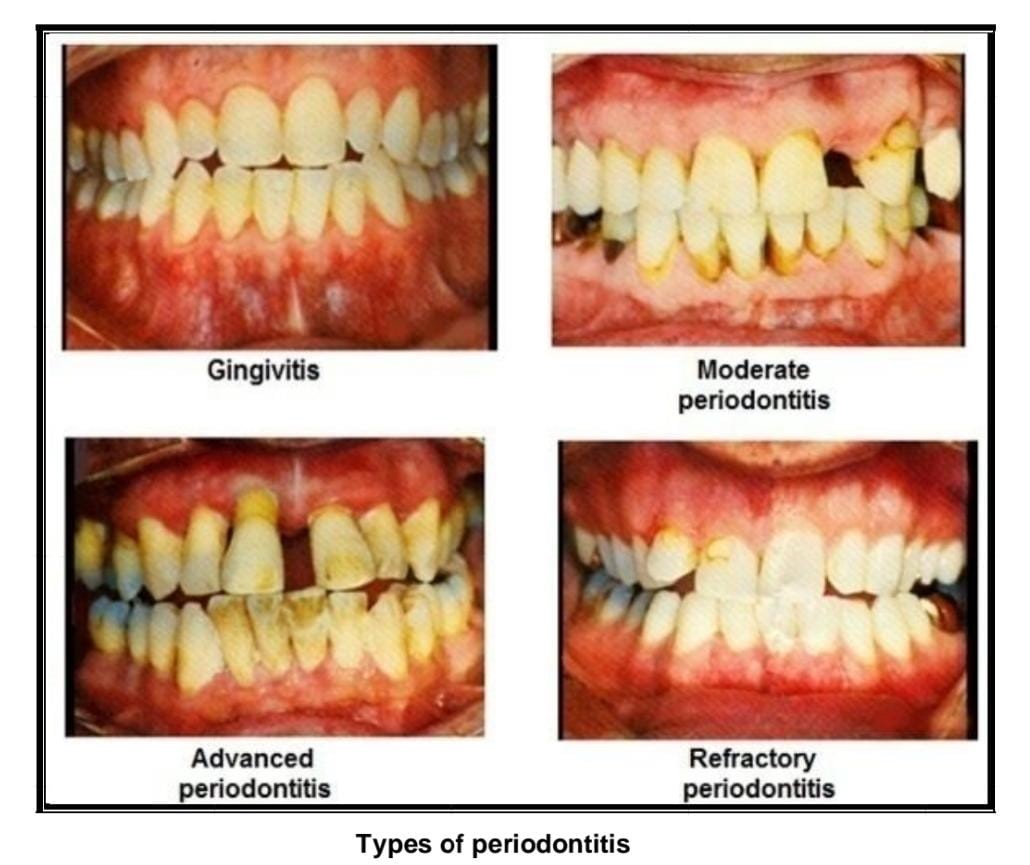
Fig No: 3 Types of periodontitis
Treatment
It's also crucial to remember that systemic antibiotic therapy has been shown to be clinically effective in treating superimposed infections, patient non-compliance, etc. Because periodontitis is the source of local pharmacological treatments, elevated levels of the toxic side effects of systemic administration of high dosages to the condition are considered a localized disease. [18,19] Because the drug's distribution in the periodontal pocket is typically not particularly obvious and the gingival sulcus flow swiftly removes the drug from the site of action, treating periodontitis is extremely difficult. For example, 40 times an hour, material may be replenished in a periodontal pocket that is 5 mm deep.[20] Currently, scaling and root planning the mechanical removal of bacteria are the mainstays of conventional nonsurgical periodontal therapy. Even though the patient's pocket geometry may not be conducive to total excision, it nevertheless causes discomfort for the patient, and in some situations, infections return to cavities following treatment. It has been suggested that using various antimicrobial treatments in conjunction with root planning can reduce the likelihood of pathogenic germs reoccurring.[21] The correct delivery of this medication is a significant difficulty in its therapy. Multiple dosages cause bacterial resistance, and systemic delivery exposes medications to the entire organ, resulting in unwanted side effects. Mouthwash prevents periodontal pockets from receiving adequate medication concentrations. The most effective strategy at the moment is thought to be local drug delivery systems, which release the active ingredient at the site of action at a regulated pace over a predefined amount of time. Easy delivery, adequate retention at the administration site, and ideally controlled drug release are all characteristics of the perfect drug delivery system.[22]
Symptoms [23]
In comparison to early gum disease, periodontitis is a more advanced stage of periodontal disease and might present with more severe symptoms. These are a few common signs:
i. Deepening Gum Pockets
A dentist can identify this during an examination: a deeper gap between your teeth and gums.
ii. Gum Recession
More gum recession, revealing more of the tooth's surface or perhaps the root.
iii. Loose Teeth
Teeth that seem unsteady or loose because the gums and supporting bone have been lost.
iv. Persistent Bad Breath
Increased severity and persistence of foul breath that is unabated by good mouth hygiene.
v. Pain While Chewing
Gum disease can make chewing painful or uncomfortable.
vi. Gum Pockets
Infection may develop in the pockets or gaps that develop between the teeth and gums.
vii. Change in Bite
Noticeable alterations in your teeth's bite fit, frequently brought on by teeth shifting.
viii. Gum Pain or Sensitivity
Increased pain or sensitivity in the gums, which can become more intense as the condition progresses.
ix. Pus Between Teeth and Gums
An infection is indicated by the presence of pus or an unpleasant taste emanating from the pockets surrounding the teeth.
In-Situ Gelling System
The ability to provide precise and repeatable amounts in contrast to gel that has already formed is of utmost importance. Easy administration and lower administration frequency are two benefits of the in-situ forming polymeric delivery method that enhance patient comfort and compliance. The usage of gel systems that are injected locally can help overcome the poor bioavailability and therapeutic response that conventional dosage forms demonstrate because of the drug's quick metabolism and excretion.[24] In situ medication delivery devices present an intriguing opportunity to get over this significant barrier. Easily injected into the periodontal pocket, these liquid preparations solidify to create a gel with a specific geometry after the solvent is replaced.[25] Under non physiological circumstances, the gel in situ stays in the form of a solution; under physiological conditions, it transforms into a gel in response to stimuli like pH, temperature, ions, and the solvent that is present in the mouth cavity.[26,27] In situ gel lowers side effects and increases patient compliance by delivering the drug release at a regulated pace straight to the target spot.[28] It seems that in situ forming gel is a promising option for satisfying the needs of both high adhesiveness and low viscosity. Injectable One especially efficient medication delivery method is in situ gel. The in situ forming system is a sol before administration, and it turns into a gel or solid depot as it is gradually supplied. Because it can sustain high drug concentrations in the gingival crevicular fluid for extended periods of time in order to achieve the intended clinical advantages, in situ gel is one of the most promising local drug delivery technologies. The success of using in situ gels to treat periodontitis depends on the phase transition from the fluid to the gel. The in-situ gel gelling technology has a number of benefits, such as simple dosage form applications, less frequent administration, and even drug protection against environmental changes. In-situ gel formation is a process that can be used to ocular, transdermal, buccal, intraperitoneal, parenteral, injectable, rectal, and vaginal routes for a variety of natural and synthetic polymers.[29,30] There are three approaches: ion-activated systems, pH-triggered systems, and thermally-triggered systems. To improve product retention in the periodontal pocket, use polymers such as mucoadhesive polymers to make the solution more viscous. The ability of the mucoadhesive polymer to interact with the gingival crevicular fluid found on the tooth's surface is essential.[31]
Advantages Of In Situ Gel [32,33]
Disadvantages Of In Situ Gel
Limitation Of In Situ Gel [34]
Ideal Characteristics of a Suitable Drug Candidate [35]
Ideal Properties Of Polymers For In-Situ Gels [35]
Various Mechanisms For In Situ Gel
i. Stimuli responsive in situ gel [36,37]
In this mechanisms solution covert to gel like structure after physiological condition is change like temperature, pH and ion. This type of gel is called stimuli responsive in situ gel.
These systems are injectable liquids that can be administered minimally invasively to the body and then solidify in the organ, tissue, or bodily cavity of choice . The idea pertains to the creation of mucoadhesive formulations that include a temperature-activated gel transition polymer solution at temperatures between 25 and 37 °C. At body temperature, the polymers that have a low critical solution temperature of about 32 °C go through a phase change.[38]
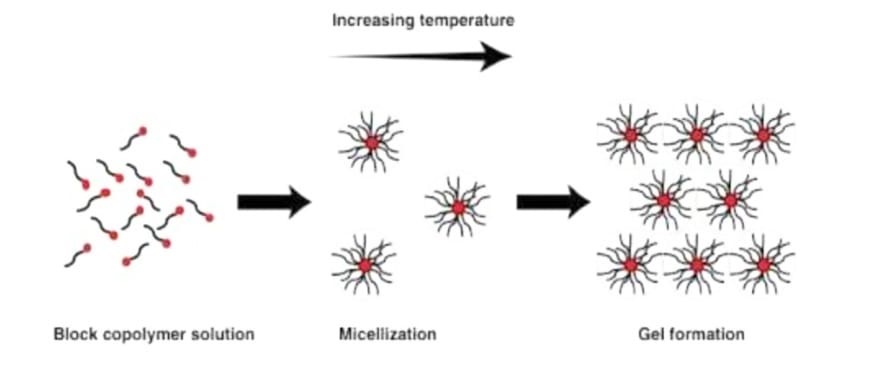
Fig. 4: Mechanism of Temperature induced in situ gel systems.
pH triggered in situ gelling systems
The class of pH-sensitive polymers includes any polymer with an acid or basic group. These polymers undergo polymerization as a result of proton acceptance or release when exposed to varying physiological and ambient pH levels. A shift in physiological pH causes the solution-gel transition, which results in in situ gel.[39]

Fig 4 : pH triggered system.
Ionic stimulation causes these in-situ gelling systems to convert from solution to gel. It comprises an ion-sensitive polymer that gels in the body's natural setting. The most often utilized ion-sensitive gelling agents for in-situ gelling systems are gellan gum, alginate, and pectin. They cause cationic complexation and the creation of a three-dimensional network structure by interacting with cations found in the physiological fluid, such as Na+, K+, Ca++, Mg++, etc. Because the periodontal pocket is rich in cations like Ca++, cationic complexation and polymeric interaction occur when formulations containing these kinds of polymers are present, leading to a solution to gel transition.[40-42]
ii. In situ gel formation due to solvent exchange [43]
Because of the solvent exchange with the surrounding aqueous environment, the gel solidifies.
One of the key processes for creating in situ gel is the substance's absorption of water from the surrounding environment, which causes the material to expand to fill the required space.
In situ gel formation, which is based on the diffusion method, precipitates the polymer matrix because solvent diffuses from the polymer to surrounding tissue. Diffusion is a more accurate and dependable mechanism of drug release from the system than erosion. Diffusion is the movement of atoms, ions, and molecules from a region of higher concentration to a region of lower concentration and is driven by a concentration gradient. The porosity of the polymer matrix, which ultimately depends on the pore formation process during the diffusion process, reverse phase. The diffusion of the medication takes place during the coagulation of the polymeric solution.
iii. Chemically induced in situ gel [44]
In this type of method ionic strength is responsible for converting in to gel like structure.
Also in situ gel structure depend up on enzymatic activity like glucoseoxidase. In this method enzymes are catalysed in to the body and convert into gel like structure.
In this method radiation, UV rays, X rays, are also responsible for convert in to solution in to gel like structure.
Polymers Commonly Used For Periodontal In-Situ Gelling Systems
Carbopol
Carbopol is a polymer comprising acrylic acid and cross-linked poly alkyl esters of sugars or polyalcohols, according to the European Pharmacopoeia. The carboxyl (-COOH) groups in this polymer range from 56.0% to 68.0%, depending on the dried material. During hydration and neutralization, carbomers swell and produce colloidal dispersions that appear viscous despite not being soluble in deionized water. [45] It is well-known pH-dependent polymer, carbopol remains in solution at acidic pH values but gels with low viscosity at alkaline pH values. HPMC and carbopol are combined to give the carbopol solution viscosity while lowering the solution's acidity. The group of water-soluble polymers known as pH-induced in-situ precipitating polymeric systems includes the carbopol system-hydroxy propylmethyl cellulose system and the poly (ethylene glycol)-poly (methacrylic acid).[46]
Hydroxypropyl methylcellulose (HPMC)
HPMC is a member of the class of cellulose ethers that have had one or more hydroxyl groups in the cellulose ring swapped out for hydroxyl groups. Deionized water dissolves HPMC, a hydrophilic polymer. It has numerous uses in medication delivery and is also biodegradable and biocompatible. HPMC is a white, yellowish-white, or greyish-white powder or granule. After drying, it might take in moisture from the surrounding air. Acetone, anhydrous ethanol, toluene, and hot deionized water do not dissolve HPMC. Nevertheless, it can form a colloidal solution when dissolved in cold deionized water.[47]
Methylcellulose (MC)
MC is a methyl ester of cellulose that has between 27.5 and 31.5% methoxy groups. The aqueous solution of MC has thermal gelation capabilities and is soluble in deionized water.[48]
Pectin
Pectins are a family of polysaccharides that mostly consist of ?-(1-4)-Dgalacturonic acid residues in their polymer backbone. In aqueous solution, low methoxypectins easily gel when free calcium ions are present. This crosslinking of the galacturonic acid chains is explained by the egg-box concept. In order to create gels that are appropriate for drug delivery, calcium ions are typically needed, even though pectin will gel when H + ions, a source of divalent ions, are present. Pectin's water solubility eliminates the need for organic solvents in these formulations, which is its primary benefit. When taken orally, divalent cations in the stomach facilitate the conversion of pectin to a gel form.[49,50]
Chitosan
Chitosan is a polycationic, biodegradable, and thermosensitive polymer that is produced by alkaline deacetylation of chitin, a naturally occurring substance found in crab and shrimp shells. As a pH-dependent cationic polymer that is biocompatible, chitosan dissolves in aqueous solutions up to 6.236. When the chitosan aqueous solution is neutralized to a pH higher than 6.2, a hydrated gel-like precipitate forms. The addition of polyol salts with a single anionic head, such as glycerol, sorbitol, fructose, or glucose phosphate salts, to chitosan aqueous solution converts the pH gelling cationic polysaccharides solution into thermally sensitive pH dependent gel forming aqueous solutions without any chemical modification or cross linking.[51,52]
Poloxamer
Poloxamers, which are nonionic triblock copolymers made up of two hydrophilic chains of polyepoxyethane on either side of a core hydrophobic chain of polyepoxypropane, are frequently employed in research on drug delivery systems.[53,54] There are numerous uses for the non-ionic surfactant polxamer 407. BASF Laboratories has registered it under the Pluronic® F127 brand, whereas ICP Laboratories has registered it under the Synperonic PE/F127® trademark. Poloxamer 407 is recognized by the U.S. Food and Drug Administration (FDA) as a "inactive ingredient" in a number of pharmaceutical preparations, including topical, ophthalmic, intravenous (IV), inhalation, suspension, and oral solutions.It is a nonionic surfactant with good solubility, low toxicity, and good drug release properties that is compatible with cells, bodily fluids, and a wide range of substances. '[55] Poloxamer 188, also known as Pluronic F-68 or Flocork, is a nonionic block copolymer that contains segments of polypropylene oxide and polyethelyene oxide organized in an ABA structure. Despite having the same chemical structure, poloxamers differ in the quantity of poly (propylene oxide) and poly (ethylene oxide) units they contain, which causes a variance in their molecular weight. Hypromellose, methyl hydroxypropyl cellulose, propylene glycol ether of methylcellulose, and methylcellulose propylene glycol ether are other names for hydroxypropyl methylcellulose (HPMC).
The formula for this substance is C8H15O6-(C10H18O6)-C8H15O5.[56,57]
Gellangum
An anionic deacetylated exocellular polymer, gellan gum (marketed as Gelrite TM or Kelcogel TM) is secreted by Pseudomonas elodea and contains a tetrasaccharide repeating unit consisting of one ?-L-rhamnose, one ?-D-glucuronic acid, and two ?-D-glucuronic acid residues. It has a propensity to gel, which can be caused by cations or temperature. Following the creation of double helical junction zones, the double helical segments aggregate to create a three-dimensional network through complexation with cations and hydrogen bonding with water. A gellan solution with a calcium chloride and sodium citrate complex made up the composition.[58,59]
Xanthum gum
Xanthomonas campestris is a gram-negative bacterium that ferments to create xanthan gum, a high molecular weight extracellular polymer. A cellulosic backbone (?D-glucose residues) and a trisaccharide side chain of ?-D-mannose-?-D-glucuronic acid-?-D-mannose are connected to the main chain's alternating glucose residues in the fundamental structure of this naturally occurring cellulose derivative. This polymer's anionic nature results from the side chain's existence of both pyruvic and glucuronic acid groups.[60]
Xyloglucan
Tamarind seeds are the source of xyloglucan, a polysaccharide made up of a (1-4)-?-D-glucan backbone chain with (1-6)-?-D xylose branches that are partially replaced by (1-2)-?-D-galactoxylose. The product of ?-galactosidase's partial degradation of xyloglucan shows thermally reversible gelation through the lateral stacking of the rod-like chains. The degree of galactose removal affects the sol-gel transition temperature. When it warms up to body temperature, it creates thermally reversible gels.[61,62]
Alginic acid
The linear block copolymer polysaccharide alginic acid is made up of residues of ?-D-mannuronic acid and ?-L-glucuronic acid connected by 1,4-glycosidic bonds. The algae source affects the percentage of each block and how the blocks are arranged along the molecule. When divalent and trivalent metal ions are added to diluted water solutions of alginates, the alginate chain's ?-L-glucuronic acid blocks' successive glucuronic residues work together to generate solid gels.[63]
Evaluation Of In-Situ Gelling System
Clarity
The in situ gel's clarity is usually evaluated visually. To look for particles or cloudiness, the gel is examined under black and white background. In situ gel formulations require clearness testing to ensure quality, efficacy, transparency, purity, and physical stability as well as to confirm the gel's applicability for a range of applications.[64]
pH
Measurement of pH was done by using a digital type pH meter by dipping the electrode completely into the gel so as to cover the electrode.[65]
Viscosity
Various viscometers, such as the Brookfield viscometer, cone, and plate viscometer, can be used to measure the viscosity and rheological characteristics of the polymeric formulations, whether they are in solution or in gel formed with artificial tissue fluid. These formulations' viscosity should be such that patients comply with them.[65]
Gel strength
A rheometer can be used to assess this parameter. A certain amount of gel is made in a beaker from the sol form, depending on the gelling agent's process. A probe is pushed slowly through the gel because the beaker containing the gel rises at a specific rate. The probe's depth of immersion below the gel surface can be used to measure changes in the load on the probe.[66]
Spreadability
One glass plate (10 x 10 cm) was carefully covered with another glass plate after 1 gram of gel had been weighed and placed in the middle. The plate was centered with a 2 kg weight, and caution should be used to prevent the plate from moving. Following 30 minutes, the gel's diameter was measured in centimeters.[66]
Drug content
1 ml of each formulation taken in 10 ml volumetric flask, diluted with distilled water and make up the volume to 10 ml. 1ml solution was taken and diluted to 10 ml with distilled water. Measured the absorbance of final solution using double beam UV visible spectrophotometer. [66]
Sol-gel transition temperature and gelling time
For In-Situ gel forming systems, the sol-gel transition temperature and pH should be determined. Gelling time is the time required for the first detection of gelation of in-situ gelling system. Thermo sensitive in-situ gel should be checked for in-situ gelling at body temperature.[66]
In vitro drug release studies
The in-vitro drug release study of from in-situ gel was determined by using a Franz-diffusion cell. The cellophane membrane was set on the receptor cell. The donor cell was packed with 1 g of in-situ gel formulation. The receptor compartment was filled with simulated salivary fluid pH 6.8 and constantly stirred using magnetic stirrer at a speed of 200-250 rpm throughout the experiments to prove homogeneity. The temperature was maintained at 37± 1°C by circulating hot water through the jacket of Franz-diffusion cell. 1 ml of sample was withdrawn at scheduled time intervals of 1hr and was replaced with same volume of pH 6.8 simulated salivary fluids to maintain the sink condition. Samples were analysed UV-visible spectrophotometer.[66]
Texture analysis
The firmness, consistency and cohesiveness of formulation may be determined using texture analyzer which mainly indicates the syringe ability of sol so the formulation can easily administered in-vivo.[67]
Accelerated stability studies
Formulation is replaced in amber colored vials and sealed with aluminum foil for the short term accelerated stability at 40?±20?C and 75±5% RH as per ICH state guidelines.[67]
CONCLUSION
In conclusion, in situ gel systems represent a highly promising and novel strategy for the management of periodontitis. By combining the benefits of sustained drug release, localized treatment, and improved patient compliance, these gels offer significant advantages over traditional therapeutic approaches. Their ability to deliver drugs directly to the affected periodontal tissues ensures enhanced therapeutic efficacy and minimal systemic side effects. Moreover, the customization of gel formulations for different drugs and periodontal conditions opens new avenues for personalized treatment options. While further clinical trials and research are needed to fine-tune their application, in situ gels stand as a transformative approach in periodontitis therapy, offering potential for better long-term outcomes in periodontal health management.
REFERENCES




Darshad Rane*, Rashmi Mahabal, Namita Bhosale, Vijay Jagtap, In Situ Gel: A Novel Approach for Periodontitis Management, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 3049-3063. https://doi.org/10.5281/zenodo.14551009
 10.5281/zenodo.14551009
10.5281/zenodo.14551009
