School of Pharmacy, Sharda University, Greater Noida, Uttar Pradesh.
Medicine-related problems (MRPs) impose tremendous challenges on healthcare systems around the world, affecting patient outcomes from childhood to advanced old age. This cross-sectional survey assesses the prevalence, types, and risk factors of MRPs among paediatric, adult, and geriatric populations, with emphasis on differences in physiological, psychological, and socio-economic factors that affect medication use and management within each age group. Some of the issues studied include inappropriate prescribing, medication adherence, drug interactions, and adverse drug reactions. Beyond that, it points out gaps in current practice and strategies to reduce these MRPs, including education and patient education, interventions from a pharmacist, and policy reforms. By delineating age-specific challenges and solutions, this survey aims to provide actionable insights to ensure medication safety and optimize therapeutic outcomes throughout people's lives. This survey-based cross-sectional study was conducted across three distinct age groups: paediatric (0–18 years), adult (19–64 years), and elderly (65+ years). Data were collected using a structured questionnaire administered to patients and caregivers in outpatient and inpatient settings of a tertiary care hospital. Key variables included demographic data, medical history, medication use, adherence patterns, and the occurrence of MRPs. The survey included healthcare provider inputs for the identification of systemic issues responsible for causing MRPs. Descriptive statistics were used to analyse the prevalence and type of MRPs, and inferential statistics were applied to assess age-group differences and predictors of MRPs. A total of 100 participants were surveyed (33 per age group). The prevalence of MRPs was highest in the elderly, followed by adults and children. Polypharmacy and drug-drug interactions were the significant issues in elderly patients, whereas non-adherence was dominant among children, followed by dosing error. Adults received MRPs mainly due to lifestyle-related non-adherence and incorrect self-medication. Several significant predictors of MRPs were, number of medications taken, comorbid conditions, and the lack of patient education. Healthcare provider-related factors, including inadequate counselling and communication gaps, added to the contributors. MRP levels are different in various age groups with unique problems and risks that correspond with each age group. Aged-specific interventions to these issues should be designed, such as an improved education for children's caregivers, facilitation of medication adherence among the adults, and polypharmacy among the elderly. Improving healthcare provider-patient communication and medication review programs are the most vital measures to reduce MRPs. Therefore, the long-term effect of such interventions on the reduction of MRPs and improvement in health outcomes should be further researched.
Medicine-related problems (MRPs) are the leading problem in health care that threatens the well-being of individuals, the quality of life, and health care systems worldwide. These problems consist of medication errors, adverse drug reactions, nonadherence to prescribed treatments, and improper use of medications. MRPs can be experienced by anyone at any age, although prevalence, nature, and severity often change because of age-related factors such as physiological changes, co-morbid conditions, and cognitive abilities.
With the increased complexity of pharmacological treatments and more therapeutic options, there remains a need to understand the effects of aging on the risks and outcomes of MRPs. For example, dosing in paediatric groups may become challenging due to weight-based calculations commonly used for dosing while requiring availability of suitable age-related formulations. Particular risks in the adolescent age group pertain to medication misuse or non-adherence, which often occurs during a transition towards independent management of health.
Lifestyle, work stress, and comorbid illnesses may impact medication use in adults, whereas the elderly are more vulnerable to MRPs. Physiological changes in the elderly with deteriorating renal and hepatic function, polypharmacy due to associated comorbidity, and increased rates of chronic diseases strengthen the risk factors for poor outcomes. Furthermore, cognitive and sensory decline in older adults may compromise effective medication management.
It seeks to explore drug-associated issues among diverse age groups and identify specific issues in a targeted age group. It attempts to provide insight into prevalence, causes, and possible measures to reduce the challenges. The understanding of specific dynamics of MRPs among various age groups will help health professionals to develop targeted interventions for safe medication practices, ensuring better outcomes for patients.
OBJECTIVE OF THE RESEARCH
Identify the most common medicine-related issues, such as drug reaction, non-adherence, or overdose, occurring in some subset of the population: children, adults, or the elderly.
Examine how changes may be influential in cases of these issues, such as physiological changes, comorbidities, or regimens of treatment and how they differ by age.
Measure awareness and knowledge of a patient appropriateness among the caregivers of different age groups.
Short-term and long effects of any medicine-related problems in general health, quality of life, and healthcare expenditure of different age groups.
Identify the gaps in current medication practices and present suggestions for designing age-specific, focused interventions, guidelines, or educational programs.
Assess how providers and pharmacists can help prevent medication-related risk issues across the age groups.
LITERATURE REVIEW
Medicine-related problems (MRPs) can occur in various forms at all ages because of the resultant variation in physiological, psychological, and social determinants that characterise each age group. Treatment for MRPs requires an understanding of age-related vulnerabilities like adherence-related challenges, pharmacokinetics, and comorbidity patterns. This article comprehensively summarizes studies done on the profile of MRPs in children, adults, and the elderly.
MRPs in Paediatric Populations:
The developmental differences of drug metabolism and the difficulty of the accuracy of dosing make children very vulnerable to MRPs. It has been identified that dose miscalculations, mostly due to weight-based prescribing errors, are one of the common causes of ADRs in paediatric patients. Nonadherence is also found to be highly prevalent in chronic diseases, such as asthma or diabetes, often due to parental administration and the palatability of the drugs. Furthermore, off-label use also poses a risk when dealing with paediatric patients, and, thus, increases the likelihood of undesirable outcomes.
Medicines-Related Problems in Adults:
Adults are more prone to medicines-related problems, especially in complex treatments for complicated diseases, such as diabetes, hypertension, or cardiovascular diseases. The studies establish that lifestyle-related nonadherence and economic costs of medication are among the major reasons associated with treatment failures. The presence of multiple comorbid conditions, which are treated using overlapping pharmacotherapies, had increased the alarm of drug-drug interactions among the adults. Also, the self-medication practice and the misuse of over-the-counter drugs upsurge the risks of MRPs among middle-aged adults.
Medicine-Related Problems in Aged Individuals:
Elderly are highly exposed to MRPs because of physiological changes associated with aging, including decreased renal and hepatic functions. These alter the metabolism and elimination pathways of drugs in the body. Contributing significantly to MRPs is polypharmacy-the hallmark of elderly care-an increase of 40% for drug-drug or drug-disease interactions among elderly patients. Cognitive impairment and physical limitations also complicate medication adherence. The Beers Criteria and similar guidelines emphasize the risks of PIMs that commonly are prescribed for elderly patients. Some of the most common ADRs reported in this population include falls, confusion, and gastrointestinal symptoms.
Age-Specific Interventions and Gaps:
Patient counselling, pharmacist-led medication reviews, and therapeutically nondrug interventions should be performed to decrease MRPs. Educating the paediatric patient will involve educational interventions targeted towards caregivers and innovative formulations of the medications. Adults would require synchronization of medications, but also digital reminders to improve adherence. The aged 65 years and above should have completed medication reviews with adequate deprescribing initiative. Nevertheless, there is a gap regarding demographic consideration in the long-term effects of these interventions. Furthermore, few studies investigate the psychosocial determinants of MRPs in pluralistic populations-for instance, health literacy and disparities.
|
Sr. No. |
Title of paper |
Author details |
Literature findings |
|
1. |
Medication use problems and factors affecting older adults in primary healthcare |
Christina Malini Christopher, Ali Qais Blebil, Bhuvan K.C, Deepa Alex, Mohamed Izham Mohamed Ibrahim, Norhasimah Ismail, Mark Cheong Wing Loong |
The results of the current study determine that about 50% of the elderly population in Penang struggle with medication use. These issues predominantly arise from medication administration, adherence, accessibility, polypharmacy, and a lack of information about medication. Qualitative analysis also identified some factors that lead to such medication-related problems. Against the aging population of ASEAN, there is an imperative for effective solutions and strategies to be found in dealing with medication use problems among elderly populations. |
|
2. |
Factors Associated with Multiple Medication Use in Different Age Groups |
Janne Moen, Karolina Antonov, Charlotte A Larsson, Ulf Lindblad, J Lars G Nilsson, Lennart Råstam, and Lena Ring |
The study concludes that among all age groups, multiple medicine use has been associated with morbidity and poor self-rated health. The vast majority of multiple drug users are taking a unique combination of medications. |
|
3. |
Age-Related Medicine
|
John Wahlich, Mine Orlu, Alpana Mair, Sven Stegemann, Diana van Riet-Nales |
This study concludes that lack of efficacy or side effects may not relate to the medicine itself, but rather to the dosage form, formulation/strength and/or the selected trademark, as patients may be unable to use certain products as intended. |
RESEARCH METHODOLOGY
1. Research Design: This study will be descriptive and cross-sectional in research design to identify and analyse medicine-related problems across all age groups. The survey will gather data based on the frequency, types, and severity of medicine-related issues, followed by various age categories: children, adults, and the elderly.
2. Study Population: Target population will include individuals from diverse age groups: below 18 years of age are categorized as follows
The sample will be appropriately stratified in such a manner that equal representation would be given to adults and older adults of diverse socio-economic status to ensure that the generalizability of findings of this study would be correctly ensured.
3. Sampling Method
This is mainly because a stratified random sampling technique will ensure that the age groups are well represented. Under this technique, individuals are randomly selected from the strata after having divided the population into strata according to age groups.
4. Sample Size: From the set criteria below, the sample size will be determined.
5. Data Collection Method: The structured questionnaire will be used to collect the data. For different requirements of different age groups, it will be available both online and offline. The questionnaire will be both the closed-ended and open-ended type. The questionnaire will comprise:
6. Data Analysis: The data will be analysed using either SPSS or R. This will be done in the following steps:
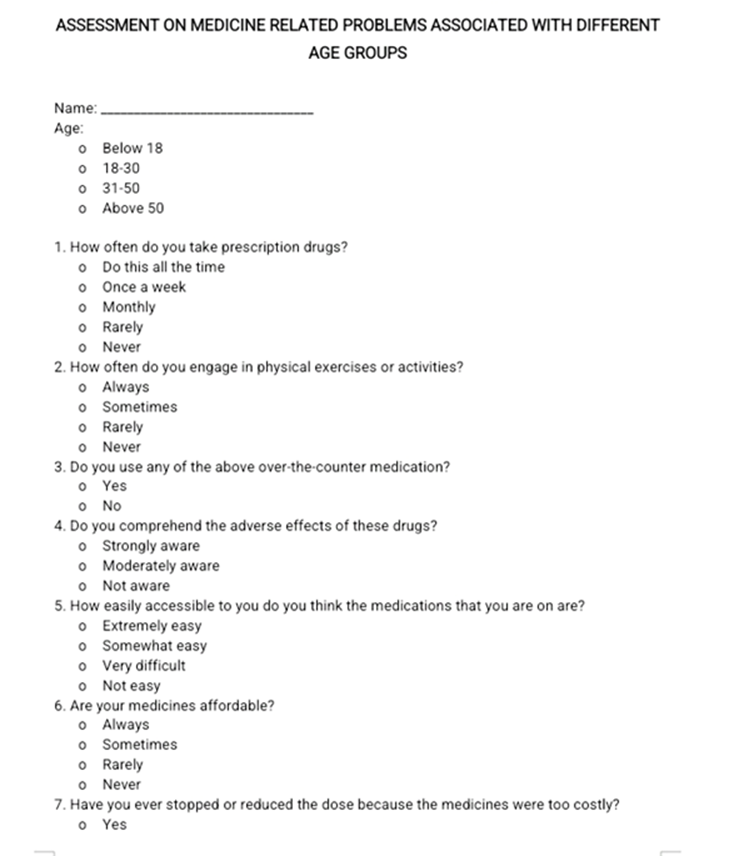
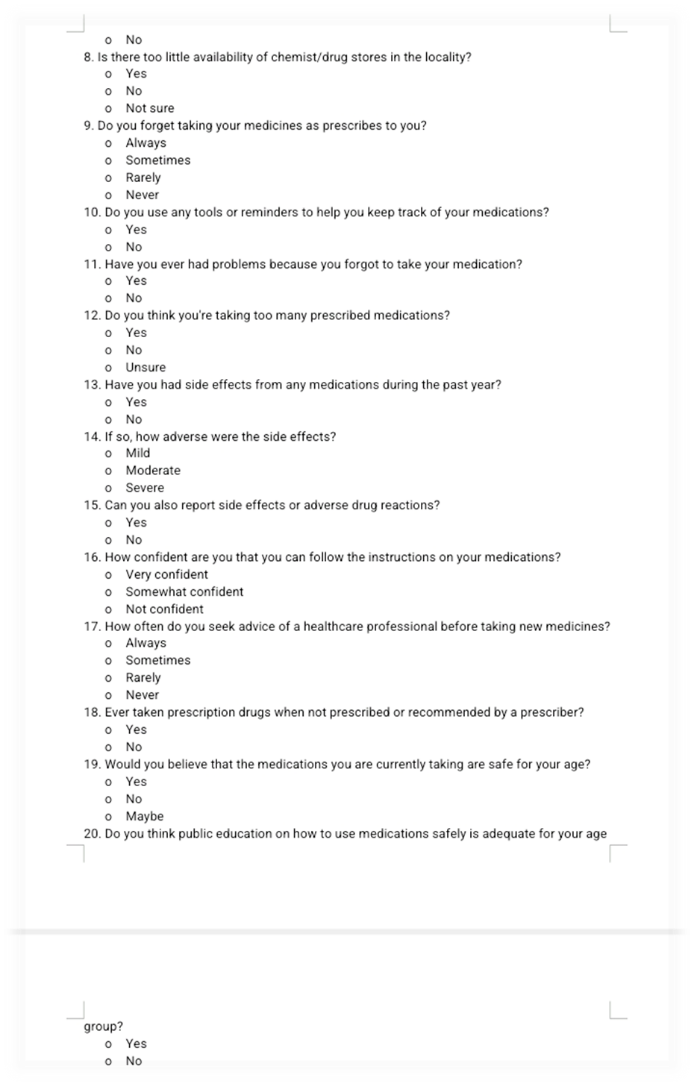
QUESTIONNAIRE
DATA COLLECTION



DATA DESCRIPTION
Primary Data: Primary data refers to the original data collected directly from the respondents through the survey process. In this survey, primary data is gathered through structured questionnaires, face-to-face interviews, or online surveys, targeting individuals from different age groups. The focus is on gathering firsthand information about medicine - related problems faced by these groups.
Primary Data Components:
Secondary Data: Secondary data refers to data that has already been collected, analysed, and published by other sources, such as healthcare reports, research studies, or official statistics. In this context, secondary data provides a background for understanding the broader patterns and trends related to medicine-related problems across various age groups.
Secondary Data Components:
FINDINGS
Number of participants: 100
|
Age Group |
No. of participants |
|
Below 18 |
22 |
|
18-30 |
38 |
|
31-50 |
24 |
|
Above 50 |
16 |
% of participants who have ever stopped or reduced the dose because the medicines were too costly: -

This pie chart depicts that among 100 responses, results showed that 60.5% (shown in red) of the patients did not cite costs as a reason to non-adhere to their medications. On the other side, 39.5% (as shown in blue) responded "Yes," which is a daunting concern to nearly 40% of respondents, indicating affordability problems with respect to the medicines themselves.
Whereas a high percentage adheres to their dose regimen, the significant percentage that faces challenges due to costs requires targeted interventions, such as financial assistance programs or policy changes to address issues of medication affordability and ensure better health outcomes.
% of participants to which there is too little availability of chemist/drug stores in the locality: -
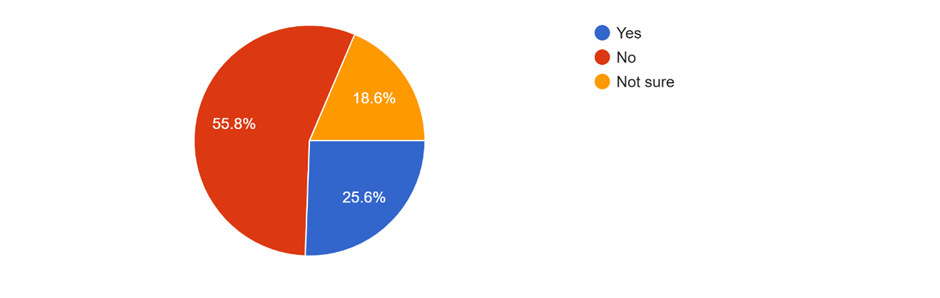
This pie chart depicts that 55.8% (Red section) said 'No,' meaning most of the respondents do not think there is a shortage of availability of chemist/drug stores in their area. 25.6% (Blue section) responded in the affirmative, meaning that one-quarter of respondents believe there is a drugstore shortage in their locality. 18.6% (Yellow section) answered "Not sure," indicating that some people are not sure whether the business is available.
This would indicate that although many are happy with the supply of chemist/drug stores, a large proportion feel there is a lack or are unaware of their existence-a concern for localized shortages or ignorance about available facilities.
% of participants who had side effects from any medications during the past year: -
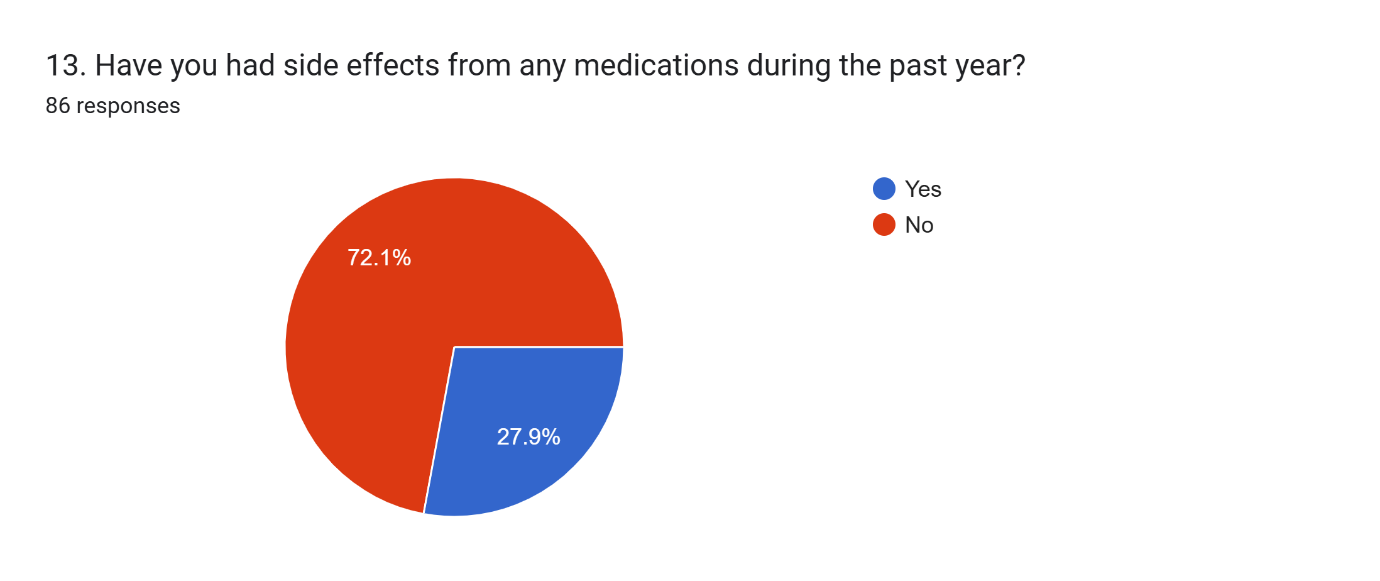
This pie chart depicts that 72.1% (Red section) responded in the negative, which means that most of the respondents did not get side effects from drugs in the previous year.27.9% (Blue area) answered "Yes", indicating that a smaller but not trivial proportion of respondents experienced side effects.
This means that whereas a good majority of respondents reported having no side effects, a third reported having side effects, which still necessitates further monitoring of drug safety and efficacy, as well as proactive health provider communication that would caution or prevent possible side effects.
% of participants who are confident that they can follow the instructions on their medications: -
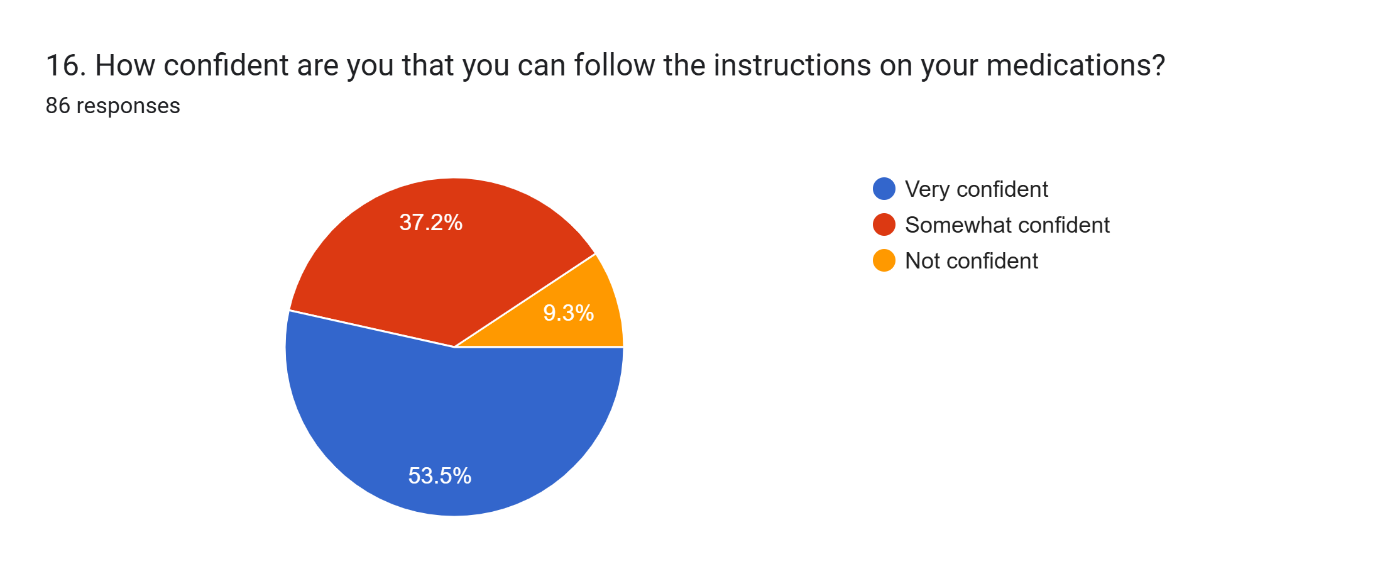
This pie chart depicts that 53.5% (Blue section) are "Very confident" in their ability to follow medication instructions, showing that the majority is highly confident in understanding and adhering to their regimen for medications that is 37.2% who are "Somewhat confident," that is, moderately confident but can still experience occasional difficulties or uncertainties.
Yellow section: "Not confident." 9.3% There is this much smaller group that has problems following directions. Maybe, just maybe, a little more support or clarification.
% of participants who believe that the medications they are currently taking are safe for their age: -
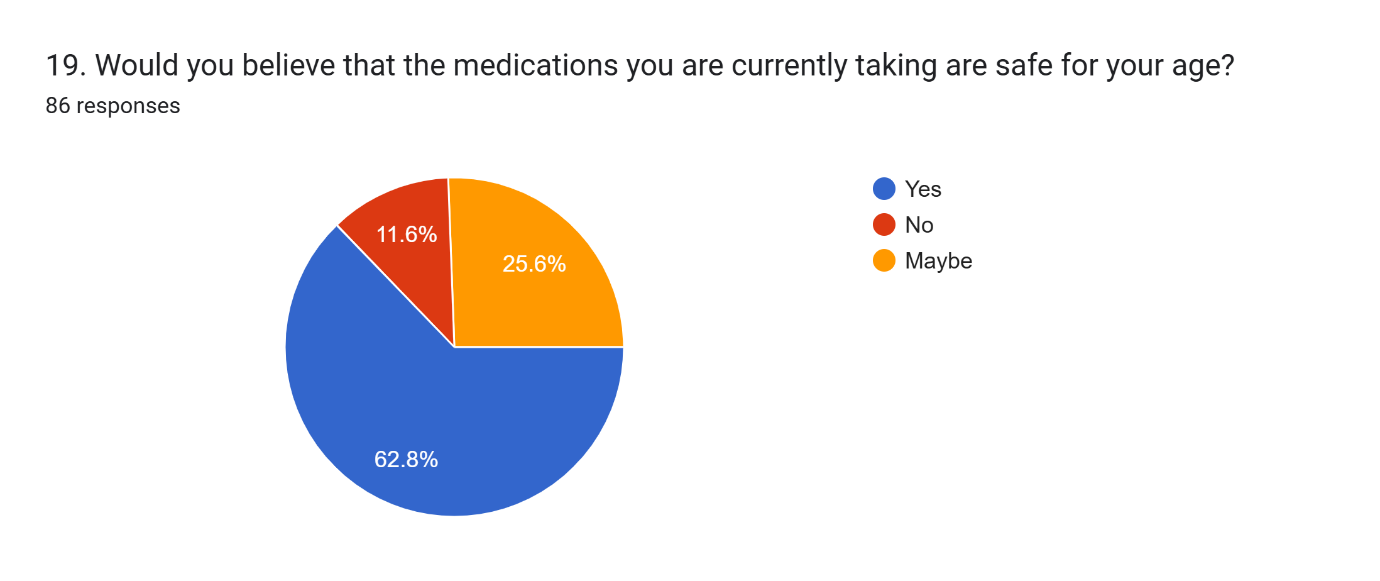
This pie chart depicts that majority of the respondent’s rate that the medications they are currently taking are safe for them:62.8% (Blue section) said "Yes," which indicated that they were confident of the safety of their medications.
25.6% (Orange segment) answered "Maybe," indicating that the medicine they consume is not safe. In the red section, 11.6% answers, "No," which suggests that they do not believe their medications are safe.
This suggests that although many consumers believe in their drugs, the percentage of those who do not or are unsure and concerned is high enough to warrant attention and perhaps better education or consultation regarding the medications they are taking.
DISCUSSION
Medicine-related problems vary quite significantly across age groups because of physiological, metabolic, and lifestyle differences. For infants and children, dosing is more frequently problematic because of the low body weights-thereby requiring precise weight-based calculations-and immature liver and kidney function-affecting metabolism and excretion of drugs and thereby increasing the likelihood of toxicity.
Issues involving medicine intake might also result among adolescents in chronic diseases such as asthma or diabetes due to their fight for independence and influence from friends. In adults, multiple medicines that may be prescribed for more than one condition might lead to drug interactions, side effects, or inefficacy. Older adults face more risks because of changes that occur with age, such as renal and hepatic decline, reduced clearance of drugs, and increased sensitivity to certain drugs.
In addition, impaired cognitive function can sometimes cause elderly people to make medication errors or commit non-adherence from unconscious reasons. Known age-specific challenges require adaptation of medical care to obtain the best results with minimal risk.
CONCLUSION
A survey across various age groups on the issues of medicine exposed serious challenges in the use of medications by age. These findings can be summarized as follows:
Elderly Population (50+ years):
Middle-Aged Adults (30–50 years):
Young Adults and Adolescents (18–29 years):
Children (0–17 years):
Recommendations:
For the Elderly: Implement medication reconciliation programs, simplify regimens, and provide clear, accessible instructions.
For Middle-Aged Adults: Patient education and lifestyle interventions to facilitate adherence without becoming overly dependent on medications.
For Young Adults: Targeted campaigns and school-based programs to raise awareness about the safe use of medication.
For Children: Train their caregivers in proper dosing techniques. Improve the palatability of pediatric formulations.
REFERENCES



Swati Sharma, Shivanshu Sharma, Rishabh Gupta, Dil Prasad Subba, Medicine Related Problems Associated with Different Age Groups, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1973-1984. https://doi.org/10.5281/zenodo.16903911
 10.5281/zenodo.16903911
10.5281/zenodo.16903911
