Department of Pharmacy Practice, Shivlingeshwar College of Pharmacy, Almala, dist. Latur, Maharashtra.
This review examines hepatorenal syndrome (HRS) in viral hepatitis, outlining its evolution into a complex clinical challenge. It summarizes the etiology, epidemiology, and dual classification of HRS into rapidly progressive type 1 (HRS-AKI) and slower type 2 forms, noting the diagnostic challenges in differentiating HRS from other acute kidney injuries. The review discusses the pathophysiological mechanisms—namely systemic vasodilation and compensatory renal vasoconstriction—and current treatment strategies, including early intervention with albumin and vasoconstrictors (terlipressin, norepinephrine, midodrine/octreotide), renal replacement therapy, and liver transplantation. It also highlights emerging treatments such as TIPS and artificial liver support systems, underscoring the need for prompt, multidisciplinary management to improve outcomes.
The liver and kidneys are two of the many organs affected by hepatorenal syndrome (HRS). People with acute or chronic liver disease may experience acute kidney injury as a result of it. In the late 1800s, the first correlation between cirrhosis and renal failure was noted. Subsequent studies conducted in the mid to late 1900s demonstrated that renal failure in liver cirrhosis was functional. This was shown in hepatorenal syndrome patients who did not have proteinuria and had normal kidney histology. Clinical examples of this included the improvement of renal function in patients with liver cirrhosis who received a liver transplant and the transplantation of kidneys from patients with HRS into those with chronic kidney disease. The link between renal vasoconstriction and HRS was established by additional research examining renal clearance.[1]
Etiology:
In developing nations, viral hepatitis is the most frequent cause of hepatorenal syndrome, or liver failure. Hepatitis B or, less frequently, Hepatitis C are the most common causes. Acetaminophen, chronic alcoholism, or any medication that causes cytochrome p450 to be triggered, and non-alcoholic steatohepatitis (NASH) are the most common causes in the developed world. Less frequently, viruses like CMV, HHV6, and Parvovirus B19 cause liver failure that results in HRS. Alternatively, metabolic causes like nonalcoholic fatty liver disease and vascular phenomena like hepatic/portal vein thrombosis.[2]
Epidemiology:
About 4% of patients with decompensated liver disease will develop hepatorenal syndrome. The majority of these patients suffer from portal hypertension as a result of cirrhosis, alcoholic hepatitis, or metastatic cancers. In patients with decompensated liver disease, the cumulative risk of developing HRS is 18% at 1 year and 39% at 5 years. Patients with high plasma renin activity and hyponatremia were at the highest risk. HRS can develop in one-third of patients with spontaneous bacterial perititis. [3]
Classification:
People who have liver cirrhosis or, less frequently, fulminant liver failure are susceptible to hepatorenal syndrome, a specific and prevalent form of kidney failure.[3] The syndrome is characterized by dilatation of the splanchnic circulation, which supplies the intestines, and constriction of the kidneys' blood vessels. [4] Hepatorenal syndrome is classified into two types of kidney failure, known as type 1 and type 2 HRS, which both affect people who have cirrhosis or fulminant liver failure. Either a higher blood creatinine level or a lower urine creatinine clearance rate are used to measure the decline in kidney function in both groups.[5]
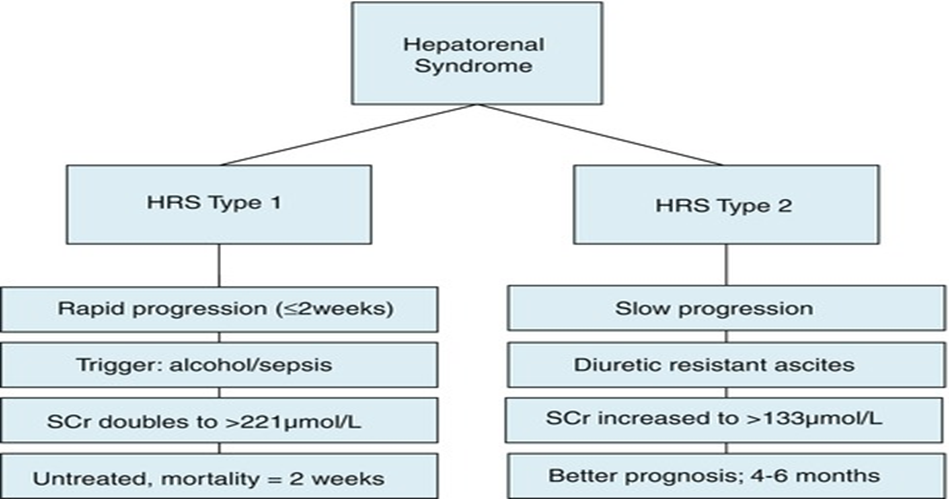
Fig 01: HRS Types [12]
Type 1 hepatorenal syndrome:
A doubling of serum creatinine to more than 221 μmol/L (2.5 mg/dL) or a halving of creatinine clearance to less than 20 mL/min in less than two weeks are signs of type 1 HRS, which is characterized by rapidly progressing kidney failure. People with type 1 HRS have an especially poor prognosis; after one month, the mortality rate is more than 50%. [6] Individuals with type 1 HRS are typically sick, may have low blood pressure, and may need medication to maintain blood pressure (vasopressors) or to strengthen the contraction of the heart muscle (inotropes). [7] In contrast to type II, kidney failure in type I hepatorenal syndrome stabilizes and gets better with treatment.The cornerstones of treatment are volume expanders and vasoconstrictors.[8] Due to new research, the International Club of Ascites revised their definition of HRS Type 1 in 2015. Known as HRS-AKI, it can be identified even if the serum creatinine level is less than 2.5 mg/dl (221 umol/L) because there is no minimum creatinine value required.[9]
Type 2 hepatorenal syndrome:
On the other hand, type 2 HRS does not have an inciting event and develops and progresses more slowly. Serum creatinine levels rising to >133 μmol/L (1.5 mg/dL) or creatinine clearance below 40 mL/min, along with urine sodium levels below 10 μmol/L, are indicators of this condition. [10] It also has a poor prognosis; unless the affected person has a liver transplant, the median survival is about six months. It is believed that type 2 HRS is a component of a group of diseases linked to elevated portal vein circulation pressures, which start with the formation of abdominal fluid (ascites). Diuretic-resistant ascites is another condition on the spectrum, in which the kidneys cannot eliminate enough sodium to remove the fluid, even when diuretic drugs are taken. Before their kidney function deteriorates, the majority of people with type 2 HRS have diuretic-resistant ascites. [11] Like the revised HRS-AKI, HRS-NAKI refers to functional kidney injury in cirrhosis patients who do not fit the HRS-AKI criteria. It can be separated into two groups: HRS-AKD, which is defined as having an eGFR of less than 60 ml/min/1.72 for less than three months, and HRS-CKD, which is defined as having an eGFR of more than three months. [9]
Pathophysiology:
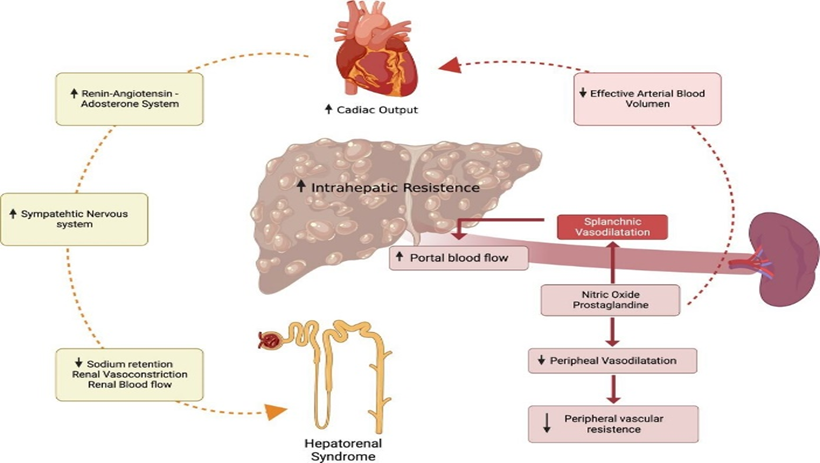
Fig 02: Pathophysiology HRS [13]
The neurohormonal cascade that causes HRS can be set off by cirrhosis and portal hypertension. Vasodilators and cytokines such as prostaglandins and nitric oxide are then produced and released, leading to both systemic and splanchnic vasodilation. Three distinct compensatory mechanisms are activated by the carotid and aortic arch baroreceptors in response to a systemic decrease in circulating pressure. These include the release of vasopressin, the sympathetic nervous system (SNS) being activated, and the renin-angiotensin-aldosterone system. Further renal vasoconstriction is induced by the decline in cardiac output and systemic vascular resistance brought on by the progression of cirrhosis. [3] Renal vasoconstriction exacerbates the subsequent renal hypoperfusion, which ultimately results in renal failure. Gastrointestinal bleeding, large volume paracentesis of ascites without plasma expansion, and spontaneous bacterial peritonitis are the most frequent causes of HRS.[15]
Diagnosis:
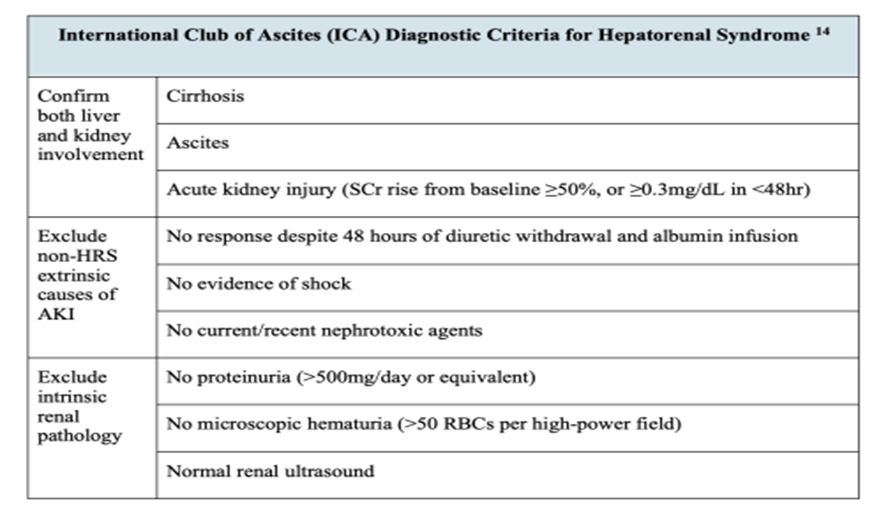
Both liver function and end-organ dysfunction should be assessed in any patient exhibiting signs and symptoms of progressive liver failure. In addition to the hepatic panel of bilirubin, protein, albumin, and transaminases, laboratory tests should include a complete blood count, metabolic panel, blood gas, lactate, ammonia, and coagulation studies.[16] Urinalysis, urine osmolality, and the computation of fractional sodium excretion (FENa) and fractional urea excretion (FEUrea) should all be part of the urine evaluation process.[18] How can these labs be useful? Recognizing acute kidney injury (AKI) is the first step in diagnosing HRS in a patient with liver failure. Serum creatinine (sCr) fluctuates with severe hepatic dysfunction in addition to age, sex, and body mass index. Such dysfunction reduces muscle mass for creatine supply in the first place and hinders the conversion of creatine to creatinine.[17] According to the International Club of Ascites guidelines, if the sCr increases by 50% from baseline or by 0.3 mg/dL from the initial sCr within 48 hours of admission, AKI is diagnosed in these patients.[19] Since HRS is a diagnosis of exclusion, the AKI still needs to be further differentiated from there.[17] According to a prospective study of 562 cirrhotic patients, spontaneous bacterial peritonitis (SBP, 46%) was the most common cause of renal failure in this population, followed by hypovolemia (32%), and HRS (13%). This means that HRS is by no means the most common cause of kidney injury in cirrhotic patients.[20] Therefore, before a patient with cirrhosis, ascites, and AKI is definitively diagnosed with HRS, other causes of kidney injury must be ruled out through diagnostic and possibly therapeutic interventions. These include treating hypovolemia and any underlying infections, as well as discontinuing any nephrotoxic, vasodilatory, and diuretic medications.[18]
The inability to respond to volume replacement with 1g/kg/day albumin (not more than 100g/day) over two days is another important criterion for diagnosing HRS.[14] Since this cannot be ascertained in the emergency department, the emergency physician should continue to look for alternative causes. For instance, an obstructive uropathy may be indicated by hydronephrosis on renal ultrasonography.[14] White blood cell or granular casts may indicate acute tubular necrosis or interstitial nephritis, respectively, while protein containing red blood cells may indicate glomerulonephritis (particularly in the context of hepatitis).[21] Naturally, these distinctions are often hazy: tubular necrosis, bile cast formation, and subsequent tubular obstruction can result from a significant decrease in renal blood flow in HRS.[22] There are still other factors to rule out before diagnosing HRS, such as prerenal azotemia and abdominal compartment syndrome, even in patients with the expected high urinary osmolality but low FENa and no urine blood or protein.[23,24] A fractional excretion of urea less than 28% was found to be 75% sensitive and 83% specific for HRS in a recent retrospective cohort analysis of cirrhotic patients with ascites and AKI.[25]
Table 01: ICA criteria [14]
Prognosis:
The average survival for Type 1 HRS is less than two weeks, which is a poor prognosis. The median survival for type 2 HRS was 6 to 12 months without treatment, but it is generally more chronic and depends on the severity of the Child-Pugh class of liver disease. [26]
Treatment Strategies:
Since patients with cirrhosis and AKI frequently deteriorate quickly, treatment of AKI in these patients should start as soon as a diagnosis has been made and the cause of AKI has been determined. Following an AKI diagnosis, the standard course of treatment involves stopping all diuretics and administering a fluid challenge of 20–25% IV albumin at 1 g/kg/day for two days (expert opinion, not evidence-based).[27] If required, low volume therapeutic paracentesis with albumin should also be carried out to control ascites.[28,29] This encourages early circulating volume expansion in the setting of decreased EABV in addition to ruling out pre-renal azotemia. Due to their negative inotropic effect, nonselective β-blockers, along with other possible nephrotoxic agents and vasodilators, must also be temporarily stopped during the first phase of treatment.[30,31]
Vasoconstrictors (Terlipressin, Midodrine, Norepinephrine) to improve renal perfusion.
Vasoconstrictors:
The cornerstone of treatment for HRS-AKI is vasoconstrictors. This is because the hemodynamic abnormalities that have caused HRS-AKI can be improved by their mode of action. They should begin as soon as HRS-AKI is diagnosed and are advised to be used in conjunction with albumin[42,43]. Terlipressin, norepinephrine, a combination of midodrine and octreotide, or dopamine with furosemide are among the vasoconstrictors used to treat HRS1. Terlipressin is the most commonly used vasoconstrictor in the world. By decreasing portal inflow, splanchnic vasoconstrictors such as octreotide and terlipressin improve central compartment filling by transferring a portion of the intravascular volume to the systemic circulation and simultaneously lowering portal pressure. By reducing the compensatory activation of different systemic vasoconstrictors, this also enhances renal circulation. [45] By raising mean arterial pressure and, consequently, renal perfusion pressure, systemic vasoconstrictors like midodrine and norepinephrine enhance renal circulation.[45] Every study that has been released to date has included patients using the conventional definition of HRS1. Future patients would have started treatment with pharmacotherapy about 4 days earlier and with a lower sCr because the new diagnostic criteria will enable us to diagnose HRS earlier at a lower sCr level.[46] Since lower pretreatment sCr is more likely to be linked to a transient course of AKI,[47] it is hoped that this will result in better outcomes with an earlier start to treatment. However, we will need to wait for the findings of future studies to confirm this hypothesis.[96]
Terlipressin:
Terlipressin, an analogue of vasopressin, causes vasoconstriction by binding to the vascular smooth muscle cells' V1 receptor. By lowering intrahepatic resistance and portal inflow, terlipressin lowers portal pressure. Renal circulation will improve and mean arterial blood pressure will rise as a result of the subsequent redistribution of blood volume to the systemic circulation.[48] By decreasing bacterial translocation in decompensated cirrhosis, terlipressin has also been demonstrated to reduce systemic inflammation and, as a result, lessen the degree of vasodilatation that occurs when an infection is present.[49] The largest trial to date included 300 patients[50] in the most recent published randomized control trial comparing the use of terlipressin versus placebo, both with albumin, in the treatment of HRS1 from North America. The study's findings unequivocally demonstrated that terlipressin improves renal function more effectively than a placebo. Terlipressin was administered as intermittent boluses at a starting dose of 1.0 mg every 4-6 hours. If, by day 4 of treatment, the sCr had decreased by less than 30% after at least 10 doses, the dosage was increased to 2 mg every 4-6 hours, with a maximum daily dose of 12 mg.[50] Up to 14 days of treatment should be administered; if the patient responds completely, treatment should be discontinued sooner. For non-response, which is defined as the sCr rising in spite of treatment, treatment could also be discontinued on day four.[50] Six days was the median length of treatment. 32% of the terlipressin group experienced verified HRS reversal, which is defined as lowering sCr with treatment twice to Up to 90 days following the end of treatment, there was no change in either overall survival or transplant-free survival.[96]
Norepinephrine:
Norepinephrine is a systemic vasoconstrictor because it is an alpha agonist. It causes the vascular smooth muscle cells' alpha-1 adrenergic receptor to become active. In advanced cirrhosis, the resulting elevated peripheral vascular resistance can raise mean arterial pressure and, consequently, renal perfusion pressure. Although norepinephrine is less expensive than terlipressin, the cost-benefit ratio may be outweighed by the need for cardiac monitoring and a central venous catheter in an intensive care unit (ICU). In order to maintain renal perfusion, the dose is adjusted to maintain the mean arterial blood pressure, which ranges from 0.5 to 3 mg/h. There are currently no studies that compare norepinephrine to a placebo. The majority of published trials have compared the effectiveness of terlipressin and norepinephrine in treating HRS1. These are all small randomized trials with 99 patients in the terlipressin arm and 96 patients in the norepinephrine arm.[51-55] According to reports, norepinephrine can reverse HRS1 with an efficacy of 39% to 70%.[51-55], and in this sense is comparable to terlipressin.[68-70] All of the published studies, however, are highly susceptible to bias because they only included a small number of patients. Terlipressin was more effective than norepinephrine in reversing HRS-AKI in patients with decompensated cirrhosis in the context of ACLF as defined by the Asian Pacific Association for the Study of the Liver ACLF Research Consortium.[56] In contrast to a combination of midodrine and octreotide, a different comparative study revealed greater rates of full response with HRS reversal when norepinephrine was used.[71] A small feasibility study from North America that used norepinephrine in a non-ICU setting to treat HRS in patients who did not respond to midodrine and octreotide provided additional evaluation of the use of norepinephrine. 80 With a median treatment duration of two days, 45 percent of patients exhibited a full or partial response. Responders also showed improved transplant-free survival at 90 days.[72][96]
Midodrine and octreotide:
Because terlipressin is not readily available, midodrine, an alpha-adrenergic agonist, is frequently used in North America to treat HRS1. Through systemic vasoconstriction, it raises mean arterial pressure, which enhances renal circulation and perfusion pressure. In order to treat HRS1, midodrine is used in conjunction with octreotide and albumin. Octreotide is a nonspecific antagonist of glucagon and other splanchnic vasodilatory chemicals. It has been demonstrated that octreotide by itself is ineffective in treating HRS1. Only a very small number of patients were included in all published studies utilizing the combination of midodrine, octreotide, and albumin[58,59,73], but the response is very slow and can take weeks to show improvement in renal function, even though HRS reversal is possible.[58,74] It has been demonstrated that the combination has much less of an impact on HRS reversal than terlipressin.[57][96]
Albumin:
In healthy people, albumin makes up 60% of plasma protein. Its primary physiological role is to maintain intravascular volume by regulating colloid osmotic pressure.[32] Both increased catabolism and decreased synthesis contribute to hypoalbuminemia in cirrhosis.[32] Patients with cirrhosis are treated with albumin due to its ability to increase volume as well as its antioxidant, immune-modulating, and endothelial-stabilizing qualities.[33] Patients with cirrhosis cannot function at their full potential because their circulating albumin is structurally altered and functionally compromised.[34] Because of the free cysteine moiety at position 34 (cys-34), albumin has natural antioxidant and scavenging qualities that aid in the removal of cytokines, reactive oxygen species, and other bacterial products.[33,35] By enhancing cardiac contractility, albumin's anti-inflammatory and antioxidant qualities also improve cardiac output in patients with advanced cirrhosis.[36] Nevertheless, cirrhosis patients' elevated oxidative stress changes albumin from its typical reduced state to an oxidized one.[37,38] Because albumin cannot bind to free radicals, it cannot carry out its scavenger and detoxifying functions. Even though a recent study indicates that routine albumin use in hospitalized patients with decompensated cirrhosis was unable to prevent renal dysfunction,[39] higher doses of albumin have been shown to have an anti-inflammatory effect. As a result, a meta-analysis discovered that patients who received 600 g of albumin overall during HRS treatment had a significantly higher chance of surviving than those who received 200 g.[40] To distinguish prerenal causes of AKI from HRS-AKI, the International Club of Ascites (ICA) advises using albumin at a dose of 1 g/kg body weight, with a maximum dose of 100 g/day. After that, albumin is advised to be given with vasoconstrictors at a dose of 20–40 g/day,[41] though no dose-responsive study has been conducted on albumin to derive at this dosing regimen. Several academic liver societies have also suggested the use of albumin in the treatment of HRS-AKI. [42,43][96]
Renal replacement therapy:
RRT has been controversially used in patients with cirrhosis and HRS1, and its use usually depends on the patient's liver transplant status. For the critically ill patient, the procedure carries risks and complications. These include the possibility of bleeding and infection, the risk of cardiac events, problems with venous access, and systemic hypotension and hemodynamic instability during dialysis.[75] Since RRT does not increase survival, the decision to start it should be tailored to the patient's needs; otherwise, it only prolongs hospital stays without increasing survival. RRT is recommended for HRS-AKI patients with uremia, electrolyte imbalances, or volume overload who are not responding to medication.[76] In these patient subgroups, continuous RRT (CRRT) is preferred over intermittent RRT because it is always difficult to maintain hemodynamic stability and proper volume management. Cerebral edema and hypotension during dialysis exacerbate the rapid fluid and solute shift linked to intermittent RRT.[75] It is still debatable whether anticoagulation should be used during RRT in critically ill patients who are at higher risk of bleeding, such as those with decompensated cirrhosis. The most widely used anticoagulant during RRT is unfractionated heparin; however, its safety in liver failure patients has not been proven. In critically ill patients, regional citrate anticoagulation (RCA) has a longer circuit life span and is linked to fewer adverse events than systemic heparin anticoagulation.[77] According to a systematic review and meta-analysis, RCA can be used safely during RRT in patients with liver failure without causing adverse effects such as hypocalcemia or an acid-base imbalance brought on by citrate accumulation.[78] Patients undergoing RRT with RCA have been advised to have their electrolyte and acid-base status closely monitored.[79] For liver transplant candidates, RRT is thought of as a stopgap measure before liver transplantation. RRT may increase life expectancy in certain patients by a few weeks to months.[80] Prolonged RRT prior to transplantation, however, has a detrimental effect on renal and post-transplant patient outcomes.[81] By reducing the number of organ failures, improving renal function with RRT may lower 28-day mortality in patients with HRS-AKI as part of the ACLF syndrome, according to recent data.[80,82] Therefore, regardless of their candidacy for a transplant, RRT may be helpful in this very specific group of patients with HRS-AKI.[96]
Liver Transplant:
The only cure for HRS-AKI is liver transplantation, which addresses the underlying liver dysfunction and portal hypertension. Thus, as soon as possible, patients with HRS-AKI should be referred for liver transplant evaluation. Patients with HRS-AKI are given priority on the liver transplant waiting list after being accepted because of their elevated sCr and correspondingly elevated MELD score. Since a positive response would lower the MELD score and negatively impact the priority for liver transplant, there has been some debate regarding whether or not patients with HRS-AKI should receive vasoconstrictor therapy. Nonetheless, better post-transplant survival is linked to a response to vasoconstrictor therapy prior to liver transplantation.[83] Additionally, vasoconstrictor therapy treatment lowers the risk of needing RRT both before and after transplantation.[84] Since the length of pre-transplant RRT is the most significant predictor of post-transplant renal function recovery, liver transplantation should not be postponed in patients who need it. According to reports, 14 days is the cut-off period for predicting the recovery of renal function. Palliative care ought to be provided for patients who are not transplant candidates.[96]
Transjugular intrahepatic portosystemic shunt:
Since portal hypertension and cardiac output are two of the main causes of HRS-AKI, transjugular intrahepatic portosystemic shunt (TIPS) treatment is being considered. A meta-analysis of 128 patients treated with TIPS for HRS revealed that 93% of patients with HRS-AKI had improved renal function, despite the fact that data on the role of TIPS in HRS typically involves small numbers of patients. Because of the high mortality, significant heterogeneity, and lack of a comparison group, it is challenging to evaluate the significance of this finding [75]. In patients with HRS-AKI, TIPS insertion carries a considerable risk as well, with a 90-day mortality rate of 25% to 80% [76]. It is challenging to ascertain the extent to which TIPS contributed to the high mortality rate, though. It is still challenging to precisely identify patients who will benefit from TIPS insertion in patients with HRS-AKI due to the high procedural risks and complications involved, as well as the lack of prospective or larger, well-conducted retrospective analysis of TIPS for HRS. By reducing portal hypertension, TIPS may have the most obvious advantage in the treatment of HRS-AKI. A lower incidence of HRS (9% vs. 31%) in patients with diuretic-resistant ascites treated with TIPS as opposed to serial paracentesis supports this [77].[95]
Artificial liver support systems:
In HRS-AKI, liver support systems, such as the extracorporeal liver assist device and the molecular adsorbent recirculating system, are types of albumin dialysis in which albumin recirculates as a scavenger of bacterial products and inflammatory cytokines. Studies on improving renal blood flow and survival have yielded conflicting results, and there are currently no obvious advantages to AKI-HRS [44]. Therefore, more research is required before its use in HRS-AKI can be formally advised; however, in certain patients, it may be taken into consideration as a bridge to transplantation.[95]
Organ replacement:
Since liver transplantation reverses the underlying pathophysiology causing renal impairment, it is regarded as the final treatment for HRS-AKI. Up to 75% of patients with HRS after liver transplant alone (LTA) experience renal recovery, which is evidence of this [79,80]. The length of pretransplant dialysis is the best indicator of HRS-AKI non-recovery; the risk of non-recovery rises by 6% for every extra day of pretransplant dialysis [89]. Additional pre-transplant variables linked to poor renal recovery following LTA include advanced age, elevated baseline SCr, extended ischemia during transplant, nephrotoxic agent exposure, diabetes, and ATN development [79-82]. Regretfully, by one year after transplantation, end-stage renal disease will develop in 6–10% of HRS patients with LTA [79-81]. Thus, it is crucial to think about whether the patient would benefit more from a simultaneous liver-kidney transplant (SLKT) and the possibility of renal recovery following LTA. The primary indications for SLKT at the moment are CKD, which is generally defined as GFR < 30 mg/dL at the time of listing with a GFR persistently < 60 mg/dL for at least 90 days, and AKI requiring RRT or GFR < 25 mg/dL for more than 4-6 weeks (guidelines vary) [44,91]. When deciding between LTA and SLKT, the potential benefits for each patient must be weighed against the just and equitable organ allocation principles. Organizations in charge of organ distribution have established particular rules in their nations in an effort to strike a balance between these variables [94].[95]
CONCLUSION:
Hepatorenal Syndrome (HRS) remains a severe complication of liver disease with high morbidity and mortality. While liver transplantation remains the definitive cure, recent advances in treatment strategies have improved patient outcomes and survival rates. Pharmacological interventions, particularly the use of vasoconstrictors like terlipressin, norepinephrine, and midodrine with octreotide, have shown promising results in reversing renal dysfunction. Albumin therapy continues to play a crucial role in managing circulatory dysfunction and preventing further kidney injury. Additionally, new approaches such as Transjugular Intrahepatic Portosystemic Shunt (TIPS) and artificial liver support systems offer potential benefits, though their efficacy requires further research. Early diagnosis and timely intervention remain key to improving prognosis, emphasizing the need for a multidisciplinary approach in managing HRS. As research continues, emerging therapies and innovative techniques may further enhance treatment outcomes, ultimately reducing mortality and improving the quality of life for affected patients.
REFRENCES





Kazi Abdulaziz*, Kadam Akanksha, Maheshan Darshana, Mehtre Gauri, Dr. Ashok B. Giri, Managing Hepatorenal Syndrome in Viral Hepatitis: A New Era of Treatment Strategies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 535-551. https://doi.org/10.5281/zenodo.14993213
 10.5281/zenodo.14993213
10.5281/zenodo.14993213
