Rajiv Gandhi proudyogiki Vishwavidyalaya, Bhopal
Cobalamin (vitamin B12) deficiency is caused by pernicious anaemia, food–cobalamin malabsorption, vegetarianism, and other deficiency states. It has a reported prevalence of 3–29%. The usual treatment for cobalamin deficiency consists of intramuscular injections of the drug. However, these can be painful, are difficult to give to disabled or elderly patients, and are costly if administered by health professionals. About 1% of cobalamin is absorbed orally in subjects without intrinsic factor. The daily requirement of cobalamin is 1.0–2.5 µg, and thus, large oral doses may meet these needs. The present investigation was to deliver methyl cobalamin via sublingual route for the effective treatment for management of pernicious anaemia, It was hypothesized that drug delivery through the use of sublingual spray is a unique alternative to the more conventional oral or I/V administration of drug. The preliminary study was conducted to build up a formulation for management of pernicious anaemia. Further formulation was analysed for its composition, Stability study (Photo stability) samples were tested by various chemical and analytical method for calibration. Based on the studies and analysis. Optimized composition for present formulation was delivered. The parameter like in vitro permeation, pH, Drug content, Appearance, Viscosity, have been analysed for characterization of optimized sample, Further sublingual spray was loaded with optimum drug which has shown faster drug response to the blood stream and does not degrade the drug as it travels through the digestive system. Vitamin B12 (Cobalamin) is a vital micronutrient. Although, it is required in miniscule levels in the body, it performs many vital functions. It is found exclusively in animal sources with a very few plant sources available. Deficiency of Vitamin B12 is a very common cause for megaloblastic anaemia particularly affecting the elderly population and people on vegetarian diet. With very limited plant sources available, fortification of common food with Vitamin B12 supplements in form of Cyanocobalamin becomes the obvious choice for maintaining appropriate levels in vegetarian population to avoid deficiency. However, many challenges are posed when Vitamin B12 is given orally and intramuscularly. Thus, there is a continuous need for development of newer strategies to effectively deliver the appropriate levels of Vitamin B12.
I.1 Overview of Methycobalamin
Vitamin B12 is an essential element for the proper growth & reproduction of normal cells, haematopoiesis & formation of nucleoprotein or myelin. Cells which have rapid cell division need high amount of vitamin B12.Methylecobalamine is linked with fat &carbohydrates metabolism but have major functions in protein synthesis (1).
I.2 Major functions of vitamin B12
Synthesis of DNA in cell and replication - Vitamin B12 is responsible for the synthesis of DNA and structural stability of centromeres and the sub telomeric DNA, as a methyl donor it contributes in mono carbonic acid metabolic pathway and play critical role in methylation of DNA.DNA methylation is catalysed by DNA methyl transferases that transfer methyl group from Adenosyl methionine to cytosine. Vitamin B12 along with folate and Iron have crucial role in Erythropoiesis, where erythroblast cell requires folate and vitamin B12for proliferation during differentiation by stimulate the formation purine and thymidylate synthesis which ultimately lead to formation of DNA synthesis (2).
Vitamin B12 is important for the proper functioning and development of the brain and nerve cells. They play major role in maintains of the sheaths that cover and protect nerves of CNS and PNS ensuring fast and effective nerve impulse transmission Vitamin B12play significant role in synthesis and maintain of myelin. This vitamin assists an important step in one carbon cycle which is responsible for the synthesis of neurotransmitter (3).
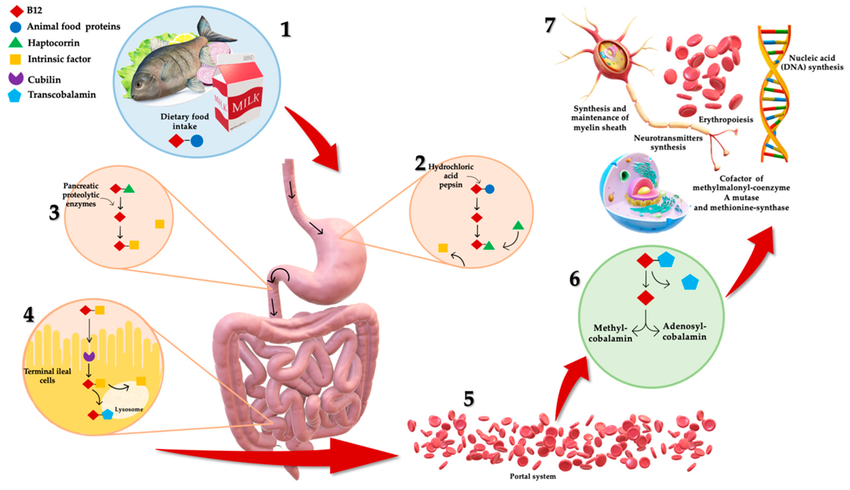
Figure1: Working of Methylcobalamine Inside the body
I.3 Major Causes of Vitamin B12Deficiencies (4):-
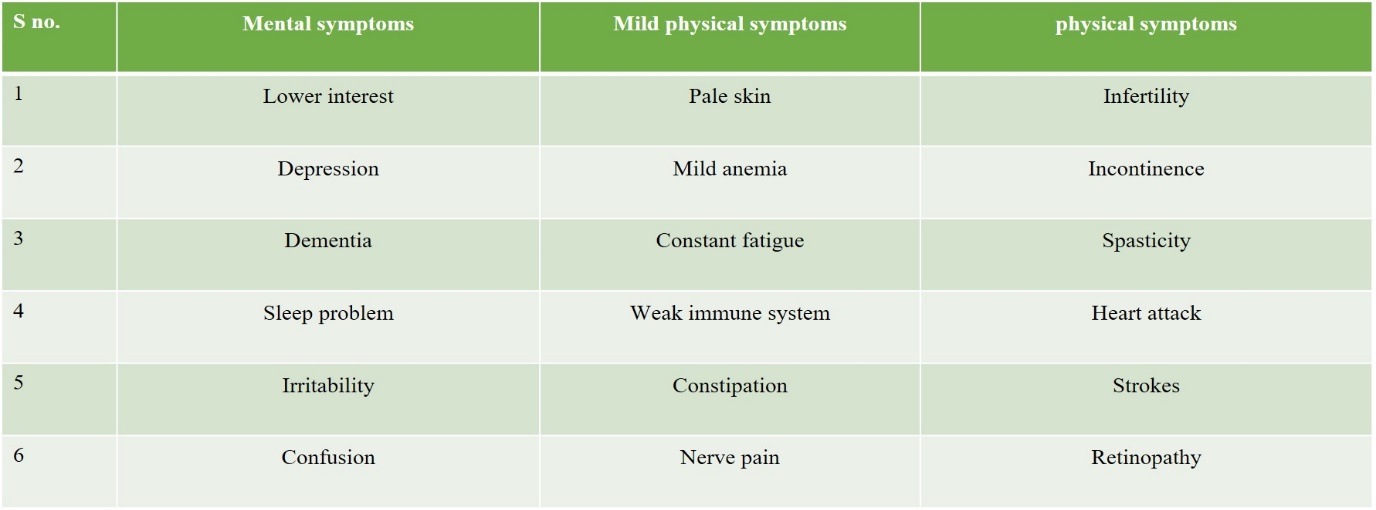
I.4 Vitamin B12 major Deficiencies symptoms
Table no 1- Major Symptoms of Methyl cobalamine Deficiencies (6)
I.5 Absorption of vitamin B12 inside the body(7,8)
Figure 2: Absorption of vitamin B12 from stomach
I.6 Mechanism of Drug absorption by sublingual route.
Sublingually means “Under the tongue” in which drug placed beneath the tongue this area consists blood vessels, in such a way substance is rapidly absorbed via blood vessel rather than via Digestive tract (9). The extent of absorption is greatly dependent on lipid solubility, the permeability of the solution, the ionization and molecular weight of the drug molecule(10).Drug can be absorbed by both active & passive mechanism,
Some drug molecule trigger endocytosis via buccal epithelium and drug molecule is engulfed by the cell and deliver into the blood circulation (11).
On the other hand passive absorption takes place by two major pathways(12).
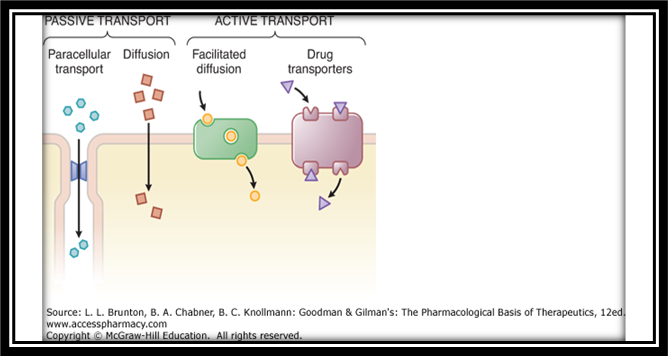
Figure3: Mechanism of drug absorption by sublingual route (13)
Intra cellular pathway is adopted by drug which is highly lipophilic in nature since they are able to cross cellular phospholipid barrier in contrast inter cellular pathway is adopted by the drug molecule which are hydrophilic & large molecule in size they will come in circulation via cellular pores (14).As the drug is more acidic it will stimulate saliva secretion from the salivary gland which will facilitate passive diffusion, increase saliva secretion protect the teeth from acidic degradation by neutralization through saliva (15). The sublingual artery will travel forward to the sublingual glands and it supplies to Branches to the neighbouring muscles & to the mucus membrane of mouth, Tongue & gums another artery will meet to the sub mental facial artery and further to external carotid artery(16). Absorption of drug through sublingual route is explained in figure 4 given below:
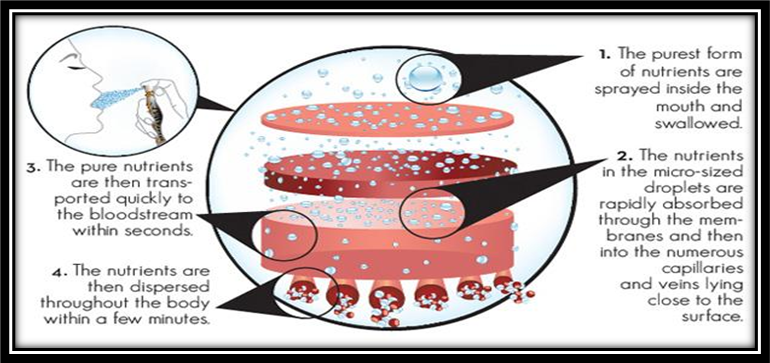
FIGURE4: Working of sublingual solution spray to systemic circulation
I. 7 Major factors which affect sublingual absorption
Diffusion is major process for the transportation of the drug from body cavity to the circulation some of the important factors which affect the diffusion are(17):-
Tabel no:2 factors affecting sublingual absorption(18,19)
|
S. No |
Factor Parameter |
Description |
|
1. |
Lipophilicity of drug |
For complete drug absorption slightly Higher lipophilic character is required to permeate by sublingual route |
|
2. |
Solubility in Saliva |
Solubility in the saliva is also important parameter for absorption, biphasic solubility in necessary. |
|
3. |
pH and pKa of the saliva.
|
Mostly unionized drug are more suitable for sublingual absorption due to pH6 of saliva, pka should be greater than 2 for an acidic drug and less the 10 for basic drug. |
|
4. |
Thickness of oral epithelium
|
Thickness of buccal epithelium is 100-200 µm which is far lower than other buccal area hence this promote absorption at faster rate. |
|
5. |
Molecular Size
|
For Hydrophilic & Large molecules, permeation enhance are used which facilitate a absorption |
|
6. |
Binding through oral mucosa
|
Drug which show binding with slivery protein will show referred absorption and low concentration in circulation. |
|
7. |
partition coefficient |
Partition coefficient range 40-2000 is optimal for the sublingual drug absorption. |
|
8. |
Saliva |
Increase dissolution of drug. There wets dose are mucoadhesive. |
|
9. |
Flexible membrane |
Comparatively less flexible membranes than other parts of intra oral cavity. hence in Delivery system drug is not dis-lodge in mucosa. |
|
10. |
Structures (teeth, gums, tongue, cheek) |
In there are drug delivery site is variety.
|
|
11. |
pH |
Saliva pH has a slightly acidic. They are good for wide range of drugs. |
|
12. |
Keratinized mucosa |
Located in regions of the mouth that do not flex. Therefore, avoid dislodging of dose |
|
13. |
Non-Keratinized mucosa |
More permeable than keratinized mucosa. (buccal, sublingual) which enhance permeation than other parts of mouth |
|
14. |
Membrane thickness |
Sublingual mucosa is a thin, but it is a good for the rapid drug absorption purpose. |
|
15. |
Mastication |
Chewing can distribute drugs around the oral cavity, increase absorption by increase surface area. |
I.8.Criteria for drug selection(20,21).
Table no:3 Ideal characteristics of drug for sublingual absorption
|
Dose range |
<10mg/day |
|
Molecular Weight |
< 500 Da |
|
Aqueous solubility |
>1 mg/ml |
|
Lipophilicity |
10<oil:water partition coefficient <1000 |
|
Melting point |
<200?C |
|
pH of aqueous |
pH 5-9 |
|
Irritation Potential |
No |
2.3 Advantages of sublingual sprays.
Table no.4 Advantages of sublingual preparation(22,23)
|
S.no |
Aspect |
Description/ comment |
|
1. |
Accessibility |
To access different site of intra oral cavity are easy , therefore it will increase patient convenience , on other hand accurate placement of the delivery system allow specific membrane targeting(21). |
|
2. |
Administration |
Spray are easily administer by patient no other medical assistance is required(21). |
|
3. |
Removal |
As easy as the administration is same is removal in case of sudden ADR(22). |
|
4. |
Patient acceptability |
This route & formulation is highly acceptable & convent for the patient use. |
|
5. |
First pass effect |
Oral mucosal membrane is having good blood supply which directly meet into jugular vein thus avoiding hepatic first pass effect(21). |
|
6. |
Avoidance of GIT environment |
As the vitamin pass through highly acidic environment of stomach it get degrade in certain amount,by this route drug will directly come in circulation with out suffering degradation.(22) |
|
7. |
By passing active route of absorption |
Sublingually drug will come in circulation by passive diffusion mechanism ,which do not require any intensric factor binding, hence it can be easily given to patient suffering from intestinal mal absorption or any major intestinal surgery(22). |
|
8. |
Enzymatic barrier |
Buccal mucosa will offer comparatively less enzymatic exposure than GIT hence less metabolic conversion is seen in oral cavity(22) |
|
9. |
Use of less additive |
It contain comparativelow amount of additive .Drug is directly available in pure form. |
|
10. |
Swallowing |
As the salivation proceeded it will lead to swallowing which will greatly affect the removal of drug form the site of action. Absorption as a result efficacy will increase.(21). |
I.9. Overview of the oral mucosa (22,23)
Oral cavity majorly contains lips – cheek – tongue – hard plate – floor of mouth (24).
Mainly three type of oral mucosa-
1. Lining mucosa- Found in the oral outer vestibule highly elastic & flexible (26).
2. The sublingual mucosa
3. Specialized mucosa - Present on the dorsal surface of the tongue. Mosaic of keratinized & non keratinized epithelium (25)
4. Masticatory mucosa On the hard palate & gum comparatively pass flexible. Masticatory epithelium is 25% & specified mucosa in 15% lining mucosa is 60% of total oral lining.(27)
I.10. Physicochemical property of oral mucosa:
Oral mucosa is different at different region of oral cavity
Epithelium is attached to under lying structure which is further connected by connective tissue or lamina propria, separated by buccal lamina (29) . These layers will provide major mechanical support & barrier for penetration of active substance (31). Detail anatomy of mouth is shown in fig 5.
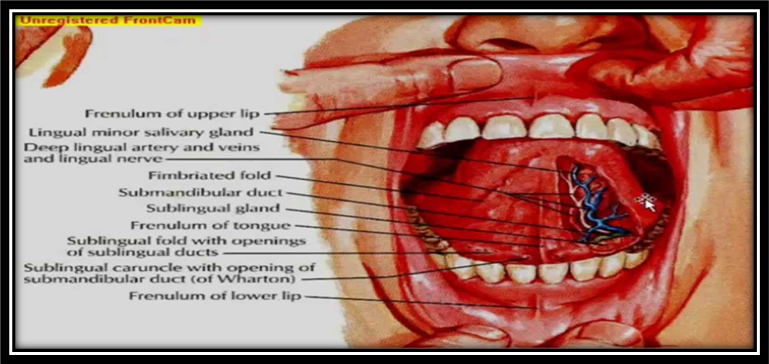
Figure 5: Sublingual Anatomy of Human Buccal Cavity
I.11 Promoting Buccal Absorption
Major barrier is epithelium barrier which property are alter by different mechanism of penetration enhancer. Majorly there are 2 type of penetration enhanceing mechanism –
I.12 Chemical method
They will increase the penetration through membrane without causing any potential damage to oral mucosa(30).
Basic Mechanism of chemical enhancers are-
Chemical enhance can be mixed in a formulation in a combination or alone depending on their efficacy &physicochemical (36)
I.13 Physical method (37)
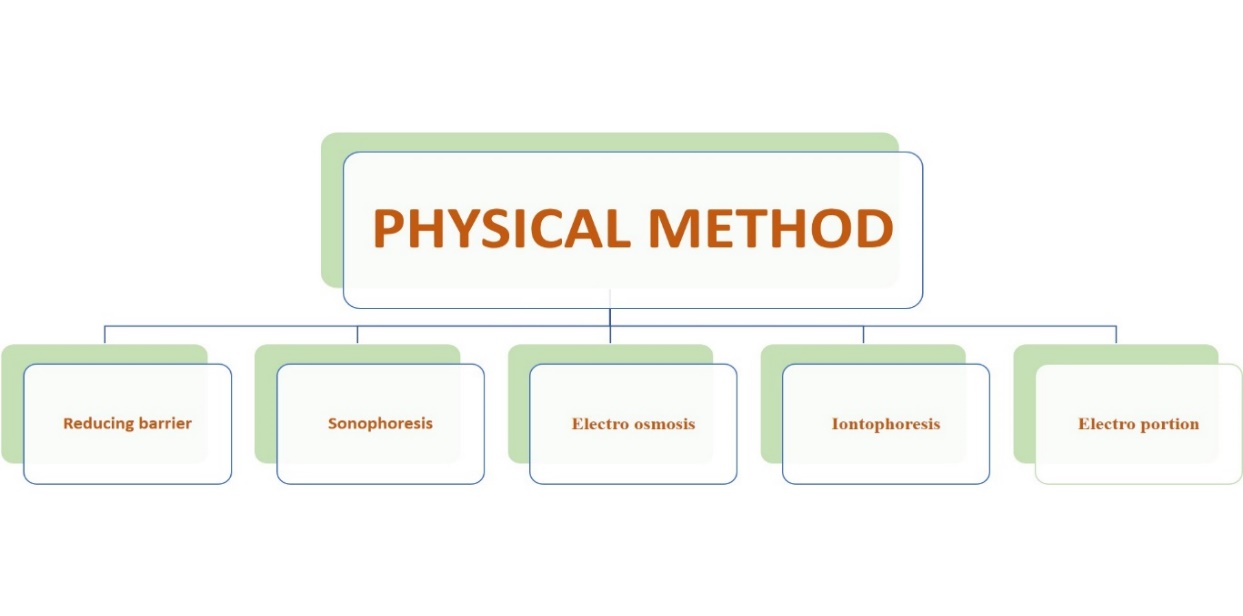
Figure 6: Physical Methods increasing buccal permeation
Reducing barrier- Reducing the barrier thickness by removal of outer most layer (38).
II. Material And Methodlogy
Table 5: List of equipment used with their supplier or manufacture’s
|
S.no |
Equipment name |
Supplier/ Manufacture |
|
1. |
Electronic balance |
Contech analytical balance |
|
2. |
PH meter |
|
|
3. |
Bath Sonicater |
|
|
4. |
Magnetic Stirrer |
Remi, India |
|
5. |
Melting point apparatus |
Uego Instruments limited Mumbai |
|
6. |
U.V visible spectrometer |
Shimadzu-1700 |
|
7. |
Viscometer(Oswald viscometer) |
|
|
8. |
Fourier transform infrared spectroscopy |
Prestige-21 (shimadzu) |
|
9. |
Mohaddessin tester( texture analyzer |
|
[II.1] Preformulation study:-
This basic study is carried out to gain information about the physical as well as chemical characteristic of drug such as PH, solubility , drug identity and its interaction with other excipients for the proper designing of drug delivery system . Methylcobalamine was received as a gift sample from Benet Pharmaceutical Ltd
Methylcobalamine:-
Test For the Identification:-
[II.1.A] Organoleptic Character
Colour:- It was determined by physical appearance.
Taste and Odor:- A extremely small amount of drug is used to acquire taste of drug with help of taste buds and smelled to get odour of it.
[II.1.B] Melting point:-
As small amount of drug is taken in a capillary tube which is used from one end and placed in melting point apparatus, gradually the temperature of apparatus is increased the temperature at which drug start melting is recorded.
[II.1.C] IR Spectra
Identification of drug was done by it IR spectra. Similar spectra was obtain from both FTTR ( Jasco 470 plus) and reference given in USP.
[II.1.D] Solubility Profile:-
Solubility of drug was determined in various aquas and organic solvent . A specific amount of drug is allowed to dissolve in different solvent (constant amount ) at room temperature & observed by visual inspection.
Solubility Profile
[II.1.E] Partition Coefficient:-
Partition coefficient is one of the major parameter which determine the liphophilicity of the drug which indirectly show potential penetrating power of the drug through biological membrane for the determine of the partition coefficient water and octanol mixture is taken in 1:1 ratio and mixed thoroughly for 10 min then 10mg of methylcobalamine is allowed to dissolve in thes mixture and shake it well in definite time internal for some time after 24hr separate the 2 layer with the help of separating funnel 2 analysed drug concentration in both phase separately .
[II.1.F] Quantitative Estimation of methylcobalamine:-
Determination of absorption maxima of the drug- Lambda max was determine by taking 10mg of methylcobalamine 10 ml of phosphate buffer of pH-7 in a volumetric flask of 25ml to make 1000 µg/ml .This make stock solution .Them from the above stock solution “A” 1ml is taken & diluted to 10ml by phosphate buffer this make 100mg . Further sub stock solution is prepared of 10 µg/ml .These sample was screened in the range of 400-20nm in simadzu 1700 UV/visible spectrophotometer to find out lambda max of drug.
[II.1.G] Test Performed for compatibility between the drug &adjuvant{ FTIR}
Physicochemical compatibility between the chitosan used as a mucoadhesive agent and the methylcobalamine is carried out by making physical mixture with kBr pellet and allow them to react for 24 hr in dark condition them in this mixture analysed and infrared radiation from 400-4000 cm.
[II.2.A] Procedure: -
Preparation of concentrate
Mucoadhesive concentrate is prepared by using 1% chitosan solution which was prepared by dissolving 250mg of chitosan in 4% of lactic acid solution and then allow to sonicate for 20 min 5mg of drug is weighed & dissolved in 1ml of water in umber colured container. Further adding appropriate amount of ethyl alcohol in the drug solute to increase it membrane permeability. Finally .9% benzyl alcohol, cyclodextrine citric acid , sodium chloride propylene is added to the solution Both the mucoadhesive mixture & solution is mixed and agitated for 20 min in 50 rpm in mag stirrer In total 1.5gm/ml citric acid is added in finally preparation to protect from microbial growth.
[II.2.B] TABLE OF OPTIMISATI
|
Table no 6 : Optimization on the basis of in vitro release and drug content, Viscosity optimizing parameter Concentration of Chitosan |
|||||||||||
|
Batch |
Conc. Of Chitosan |
Conc. Of Cyclodextrine |
PG Conc. |
Release |
Drug Content |
Viscosity |
|||||
|
F1 |
0.5% |
1% |
5% |
20.21% |
98.06% |
8.1cp |
|||||
|
F2 |
1% |
1% |
5% |
24.29% |
97.96% |
9.5cp |
|||||
|
F3 |
1.5% |
1% |
5% |
31.09% |
98.92% |
9.9cp |
|||||
|
F4 |
2.0% |
1% |
5% |
23.09% |
96.11% |
14.2cp |
|||||
|
Table 7: Optimization on the basis of in vitro release and drug content Optimizing parameter - Conc. Of Cyclodextrine |
|||||||||||
|
Batch |
Conc. Of Chitosan |
Conc. Of Cyclodextrine |
PG Conc. |
Cumlatice Release of Drug |
Drug Content |
||||||
|
F5 |
1.5% |
1% |
5% |
31.20% |
98.09% |
||||||
|
F6 |
1.5% |
2% |
5% |
34.08% |
97.11% |
||||||
|
F7 |
1.5% |
3% |
5% |
36.91% |
98.01% |
||||||
|
Table no 8: Optimization on the basis of cumulative drug release and drug content Optimizing parameter - Concentration Of P.G. |
|||||
|
Batch |
Conc. Of Chitosan |
Conc. Of Cyclodextrine |
PG Conc. |
Cumulative Release of Drug |
Drug Content |
|
F8 |
1.5% |
3% |
10% |
38.9% |
98.01% |
|
F9 |
1.5% |
3% |
15% |
40.8% |
98.91% |
[II.3] EVALUTION OF SUBLINGUAL SPRAY
[II.3.A] Visual inspection
All the prepared formulation are visually inspected for color , clarity , visual dirt particles , precipitate formulation by the ingredient discoloration or cloudiness may indicate microbial contamination.
[II.3.B] pH determination
The pH of all the formulation is evaluated by use pH meter. The pH meter was set at neutral pH-7 in distal water by its adjusting screw and finally placed inside the solution and note the reading where the pH meter stops further fluctuation.
[II.3.C] Viscosity determination
Viscosity of the sample is determined by Oswald broke field viscometer by placing the 84 probe 64 of the instrument in the container containing the sample in appropriate quantity that the probe should get immersed in the sample to avoid error. Note the reading should be taken at which is constant repeat the process for as time and take mean viscosity.
[II.3.D] Determination of methylcobalamine permeation pattern.
Permeation study were out losing vertical glass from diffusion cell, which effective diffusion area 12.56 cm 2 donor and receptor compartment is attached to each other by clamp in between both the chamber membrane disk mixed cellulose is placed with [pore size .47µm] Lower chamber is filled with 16ml of phosphate buffer pH 7.4 and temperature is maintained 37± 0.5?C magnetic starring is kept constant at 50rpm to maintain homogeneity , Donor chamber is filled with 1.5ml of test formulation membrane was previously wetted by artificial saliva for 5 minutes. After 30 second the 2ml sample is taken out from the receiver chamber and volume is make up by phosphate buffer to maintain sink condition equal quantity of buffer is place in lower chamber all the sample was analysed in U.V spectro photometer light protected environment
[II.3.E] Determination of total drug content
Assay of accurately weighed amount of formulation were carried out for the determination of net drug content. The weighed sample was dissolved in 10 ml of water distil and further it was filtered. The drug content was estimated Spectrophotometrically at 349nm using standard curve
[II.3.F] Ex vivo drug release study
The in vitro optimized formulation which shows highest permeation is selected for ex vivo study was performed on sublingual membrane of goat, which was preserved at low temperature in krebs solution. sublingual mucosa of 14 cm2 was excised carefully and left for 1 hour in artificial saliva to maintain moisture and mimic the condition of sublingual mucosa finally this membrane in mounted of glass vertical franz cell, the donar compartment and receiver compartment with 16ml of phosphate buffer of pH 7.4 at 50 rpm. To maintain sink condition 3ml of sample withdrawn from receiver chamber in equal interval of time and equal amount of phosphate buffer is added into the receiver chamber with constant stirring and temperature is maintained at 37?C±1at last all the sample are diluted with phosphate buffer and analysed by u v photo spectrometer and for the concentration of drug in each sample , permeation pattern of the drug.
[II.3.G] Stability study:-
In assay the percentage drug content was found to be 98% which complied with ICH guideline limit 98-103%. In degradation studies for thermal stress at 50?C,60?C,80?C, was provided for 30 min then store in then change in viscosity, pH, drug content was analysed by U.V. photo spectrophotometer for forced degradation study, 10ml the formulation is taken and mixed with 5% H2O2 in a umber colour glass container the resultant solution in allowed to stand for 6hr in a dark room to facilitate oxidation of the drug.To test the sensitivity towards light the proximal formulation is allow to kept in UV light for 6 hour and in dark room for 6 hour and analysed for active drug content.
[II.3.H] Mucoadhesion Testing
Texture analyzer was used to test mucoadhesion strength of the formulation. Initially mucoadhesive rig was cleaned thoroughly then 2 ml of saliva was spreader on the surface of rig and the optimized formulation was placed on it after that rig was tightly closed by upper half and place in a beaked which contain water of temperature 31±?C Then prove is allowed to come in contact with formulation and then reading of mucoadhesion strength was analysed
III. RESULT AND DISCUSSION
[III.1] Preformulation study:-
(III.I.A)Organoleptic Character
Table 9 : Organoleptic character of pure drug
|
S.no |
Parameter |
Observation |
|
1. |
Color |
Dark red crystals |
|
2. |
Taste |
Tasteless |
|
3. |
Odor |
Odorless |
(III.1.B) Melting point: -
Table no10: Melting point of pure drug
|
Drug |
Reported |
Observed |
|
Methylcobalamine |
>300?C |
304?C |
<a href="https://www.ijpsjournal.com/uploads/createUrl/createUrl-20250320204530-1.png" target="_blank">
<img alt="Figure 7 I.R. spectra of pure drug.png" height="150" src="https://www.ijpsjournal.com/uploads/createUrl/createUrl-20250320204530-1.png" width="150">
</a>
Figure 7: I.R. spectra of pure drug
|
Tabel No11: Interpretation of IR spectra of Methylcobalamine |
|||
|
Sr. No. |
Band |
Expected absorption |
Observation |
|
1 |
1556-1570 |
C=N stretching |
1564 |
|
2 |
520-437 |
Co-N axial ligand |
518 |
|
3 |
432-420 |
Co-C stretching |
430 |
|
4 |
3300-3400 |
N-H stretching |
3180 |
|
5 |
1000-1100 |
PO4 stretching |
1068 |
|
6 |
1600-1700 |
C=O stretching |
1668 |
(III.1.C) Solubility Profile: -
Table No 12: solubility profile of drug
|
S.no |
Solvent |
Observation |
|
1. |
Distil water |
Soluble |
|
2. |
Ethanol |
Soluble |
|
3. |
Chloroform |
Insoluble |
|
4. |
Ether |
Insoluble |
|
5. |
PO4Buffer 7.4 |
Soluble |
|
6. |
.9% saline solution |
Soluble |
(III.1.D) Partition Coefficient:-
Table No 13: Partition coefficient of drug
|
DRUG |
REPORTED |
OBSERVED |
|
Methylcobalamine |
1.897 |
1.596 |
(III.1.E) Quantitative Estimation of methylcobalamine:-
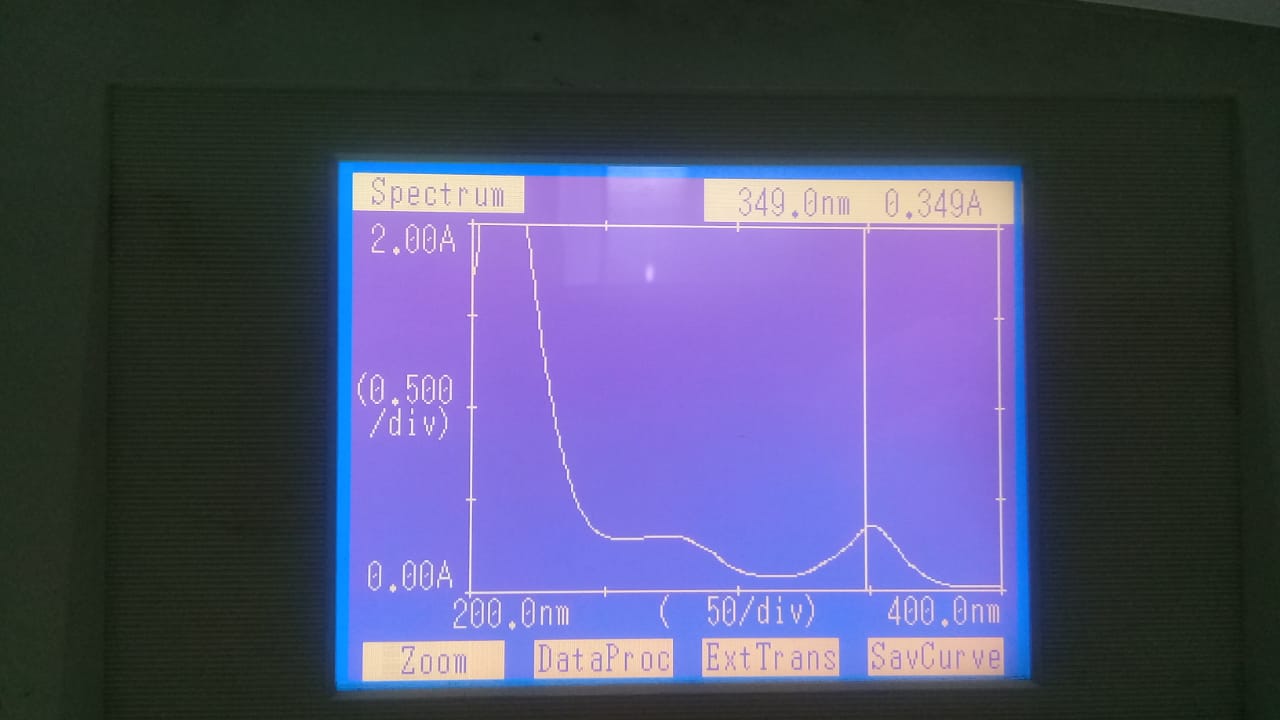
Figure 8: Showing maximum absorbing wavelength
(III.1.F) Standard curve in phosphate buffer 7.4 –
Table No 14: Absorbance profile of drug
|
S. no |
Concentration ug/ml |
Absorbance |
|
1 |
20 |
0.196 |
|
2 |
40 |
0.400 |
|
3 |
60 |
0.662 |
|
4 |
80 |
0.852 |
|
5 |
100 |
1.100 |
|
6 |
120 |
1.311 |
|
7 |
140 |
1.600 |

Figure 9: Standard Curve In Phosphate Buffer 7.4
(III.1.G) Test Performed for compatibility between the drug &adjuvant {FTIR}
Physicochemical compatibility between the chitosan used as a mucoadhesive agent and the methylcobalamine is carried out by making physical mixture and sample are compatible not showing any incompatibility.
The spectrum of chitosan showed a broad peak at 3447 cm!1 and a small peak at 2800 cm!1 corresponding to the N-H symmetrical vibration and the typical C-H stretch vibrations, respectively. Amide I and III peaks appeared at 1658 and 1322 cm1, respectively. Sharp peaks appeared at 1383 cm!1 and 1424 cm!1 corresponding to the CH3 symmetrical deformation mode. The figure also showed broad peaks at 1030 cm!1 and 1080 cm1 corresponding to the C-O stretching vibration and other peaks around 893 cm!1 and 1156 cm!1 corresponding to saccharide
(III.2.A) Visual inspection:- Appearance of all nine batch was tested against white & Black background to check to celerity and turbidity . All the above formulation were checked for 24 hours. The formulation were observed as transparent with reddish tint , no phase separation or precipitate were observed after keeping still for 24 hours.
Table no15: visual inspection of formulation
|
S.no |
Batch |
Precipitation |
Clarity |
|
1. |
F9 |
No |
Yes |
(III.2.B) pH value of methylcobalmine drug during Sublingual spray:-
pH value of methylcobalmine sublingual spray (F4,F8,F9) were determine using digital pH meter .The stability of concentration is generally affected by pH . the excipient used in the formulation will majorly decided the pH of concentration for example mucosa sublingual absorption pH should be 6-7.5
|
Table no16: pH value of methylcobalmine drug during sublingual spray |
|||||
|
|
N1 |
N2 |
N3 |
Mean |
SD |
|
F9 |
7.2 |
7.2 |
7.3 |
7.23 |
±0.057735 |
(III.2.C) Viscosity of the formulation
Viscosity of the solution will show great influence to the formulation if the solution is more viscous it will permeate in more time , hence optimum viscosity of the formulation is required so that it can be easily sprayed through actuator of the spray. Other wise it will block the nozzle of the spray.
Table no 17: viscosity of final formulation
|
Viscosity of the formulation |
|||||
|
N1 |
N2 |
N3 |
Mean |
SD |
|
|
F9 |
9.7 |
10.2 |
10.2 |
10.03 |
±0.288675135 |
(III.2.D)Determination of drug content
The drug content of methylcobalamine concentration was measured by U.V spectrophototmetric method . The percentages drug content was determine by considering 5 mg of methylcobalamine as a 100% . All the above formulation are within the limits 37% 97% 75% to 99.05% of drug content.
Table no 18: drug content in final formulation
|
Determination of drug content |
|||||
|
N1 |
N2 |
N3 |
Mean |
SD |
|
|
F9 |
98.2% |
98.4% |
98.2% |
98.3% |
±0.001155 |
(III.2.E) DRUG PERMEATION STUDY
In formulation { F1,F2, F3, F4} as the concentration of chitosan increase ,as polymer tend to trap the drug & used to release drug in sustained fasion, only 23% of the drug release in initial 3 minutes. On the other hand when concentration of cyclodextrine increase it will increase partion coefficient of the formulation as a result increasing the permeation characteristic of the formulation { F5, F6, F7 } release rise up to 36%. In formulation [F8,F9] as the amount of PG increases it will increase pore size as a result passage of the formulation is facilitated to 40%.
Table no 19: Invitro Permiation Data Of Various Formulation
|
Invitro Permition Data Of Various Formulation |
|||||||||
|
Time |
CUMLATIVE PERCENTAGE DRUG PENETRATION |
||||||||
|
Batch F1 |
Batch F2 |
Batch F3 |
Batch F4 |
Batch F5 |
Batch F6 |
Batch F7 |
Batch F8 |
Batch F9 |
|
|
15 |
4.22% |
5.61% |
5.99% |
4.98% |
6.23% |
7.04% |
7.69% |
8.17% |
9.24% |
|
30 |
6.24% |
7.49% |
8.64% |
7.11% |
9.01% |
9.19% |
10.74% |
11.91% |
12.23% |
|
45 |
7.84% |
8.94% |
9.69% |
8.11% |
12.14% |
13.69% |
13.81% |
13.99% |
14.87% |
|
60 |
9.84% |
10.21% |
10.91% |
10.21% |
13.69% |
14.02% |
14.99% |
15.63% |
16.76% |
|
75 |
11.64% |
12.14% |
13.69% |
11.66% |
16.11% |
15.91% |
16.66% |
17.91% |
18.64% |
|
90 |
13.69% |
14.94% |
15.01% |
14.91% |
18.91% |
17.69% |
18.91% |
19.69% |
20.46% |
|
105 |
15.11% |
16.12% |
17.89% |
16.19% |
21.94% |
20.91% |
22.12% |
23.22% |
24.98% |
|
120 |
16.90% |
18.24% |
19.96% |
17.91% |
24.11% |
23.91% |
27.17% |
28.16% |
29.73% |
|
135 |
17.64% |
20.11% |
21.11% |
19.21% |
28.91% |
27.91% |
29.21% |
31.69% |
32.79% |
|
150 |
18.11% |
22.69% |
24.62% |
21.21% |
30.61% |
29.17% |
31.22% |
34.19% |
35.89% |
|
165 |
19.01% |
23.91% |
27.93% |
22.11% |
31.77% |
32.19% |
34.11% |
36.49% |
37.54% |
|
180 |
20.21% |
24.29% |
31.09% |
23.09% |
32.11% |
34.08% |
36.91% |
38.99% |
40.80% |
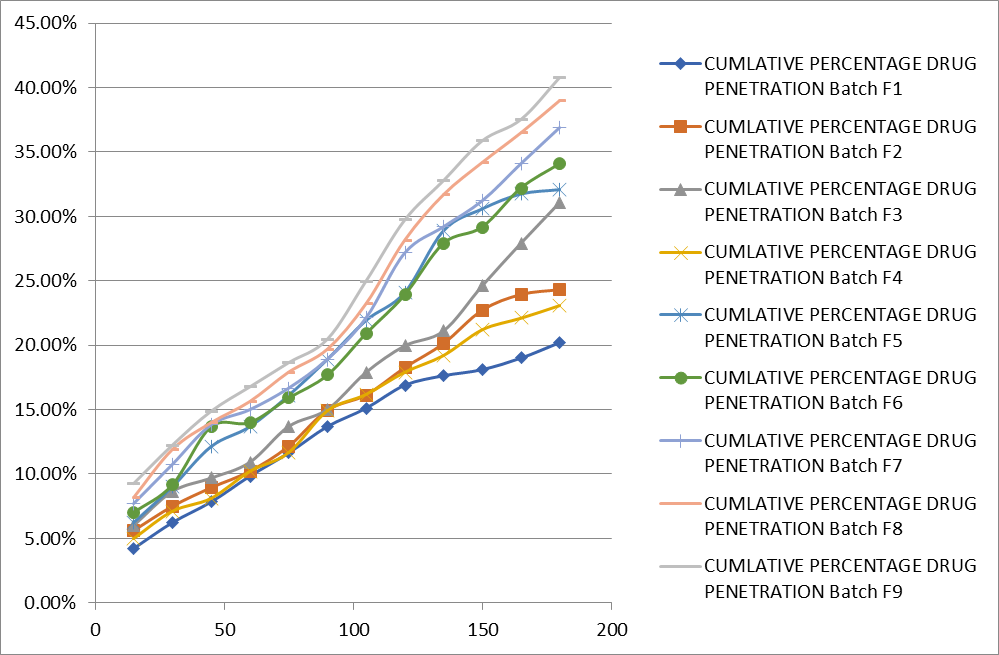
Figure no 9: %CDR of all formulation
Optimized formulation is following zero order of kinetics, which conclude that permeation pattern of formulation is independent of its concentration of drug.
|
Table no 20 : Methyl cobalamin release data from the selected formulations according to different kinetic models |
||||
|
Correlation coefficient (r2) |
||||
|
Batch |
Zero |
First |
Higuchi |
Krosemeyers Peppas |
|
F9 |
0.9879 |
0.9689 |
0.9476 |
0.9613 |
(III.2.F) EXVIVO STUDY
Ex vivo study on goat sublingual mucosa shows increase in permeation of drug through mucosa than that of In vitro condition because chitosan is able to break tight junction hence facilitate the passage of drug through this route .On the other hand PG will increase the pore size of the membrane along with alcohol as a result increase in Para-cellular movement of the drug .Therefore Ex- vivo data will help to predict In- vivo permeation pattern of the formulation.
|
Table no 21: Ex-Vivo Studies data of optimized formulation |
|
|
Time (Sec) |
Cumulative drug release in Ex vivo Condition |
|
15 |
10.20% ±1.01 |
|
30 |
19.96% ±.09 |
|
45 |
22.50% ±1.02 |
|
60 |
24.37% ±1.11 |
|
75 |
26.50% ±.09 |
|
90 |
29.46% ±.06 |
|
105 |
33.90% ±.08 |
|
120 |
37.74% ±1.09 |
|
135 |
46.11% ±1.87 |
|
150 |
52.02% ±1.89 |
|
165 |
56.32% ±.067 |
|
180 |
58.45% ±1.08 |
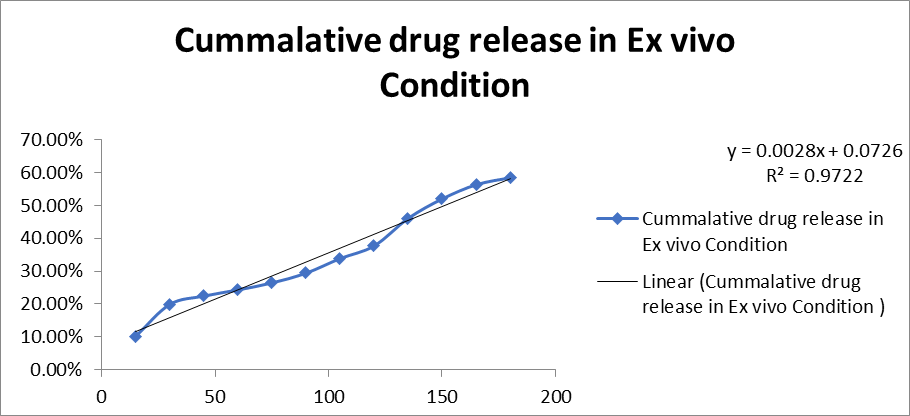
Figure no10: Ex vivo release data
(III.2.G) Stability Study:-
When formulation is allow to expose at higher temperature(50?C,70?C,90?C) the amount of drug content tend to decrease rapidly and the color of the formulation get changed from red to orange This clearly indicate the degradation of methylcobalamine at elevated temperature. Similarly when the formulation is expose to light in presence of oxygen it will degrade rapidely to give aquocobalamine and formaldehyde as a major product , as a result active methylcobalamine concentration reduces in very low time therefore protection from light is primary necessity . table 8.8 to 8.12 show various changes observed at stress condition
A-Thermal stress
Table no 22: Thermal stability study at 50?C
|
Time |
Temp- 50?C for 30 min |
||
|
|
Physical Property |
Drug content |
Viscosity |
|
30 min |
No change in color,No Turbidity |
98.2% |
10.2 |
Table no 23: Thermal stability study at 70?C
|
Time |
Temperature -70’c |
||
|
|
Physical property |
Drug content |
Viscosity |
|
30 min |
slightly orange tinch appearred, No turbidity |
80.2% |
9.7 |
Table no 24: Thermal stability study at 90?C
|
Time |
Temperature- 90?C |
||
|
30 min |
Physical appearance |
Drug content |
Viscosity |
|
|
Slight Change in color No ppt/ Turbidity |
64.47 |
8.9 |
B –photostability study
Table no 25: Photostability stability study
|
Time |
Dark Condition |
|||
|
6h |
Physical Property |
Drug Content |
Viscosity |
|
|
No Change in colour or No PPT No Turbidity |
97.80% |
10.2 |
||
Table no 26: Photostability stability study
|
Time |
Exposed to light (Sunlight) |
|||
|
6 hours |
Physical Property Orange |
Drug Content |
Viscosity |
|
|
Yellow Colour Observed |
32.40% |
9.6 |
||
Table no 27: Photostability stability study
|
Time |
Exposed to UV light |
|||
|
6 hours |
Physical Property |
Drug Content |
Viscosity |
|
|
Colour change |
30.06% |
9.8 |
||
(III.2.H) MUCOADHESIVE TESTING
This result of Mucoadhesive testing conclude that formulation is having appropriate mucoadhesive character so that it can show bio adhesion with sublingual mucosa -0.50 value shows good mucoadhesive character due to presence of chitosan matrix in the solution. As the value become more negative it will show more adhesion with the biology membrane.
<a href="https://www.ijpsjournal.com/uploads/createUrl/createUrl-20250320204530-0.png" target="_blank">
<img alt="Figure No 11 Muco adhesion Results.png" height="150" src="https://www.ijpsjournal.com/uploads/createUrl/createUrl-20250320204530-0.png" width="150">
</a>
Figure No 11: Muco adhesion Results
IV. Conclusion and Summary
Vitamin B12 deficiency is major problem in modern era. This is main problem for the people who follow strict vegetarian. Hence should rely on fortified foods as an alternate. The conventional route of fortification of food, Oral supplements and I/M injection continue to dominate the therapy regime. However, with advances in the technique to deliver vitamin B12 is continuing to improve. The various appraises attempted for the improves delivery of vitamin B12 with their respective pros and cons, sublingual route is very promising route for patient with GIT problem for erratic absorption.
REFERENCES


Ashita Pawaiya*, Dipti Jain, Formulation And Evaluation of Vitamin B 12 Sublingual Spray, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 1973-1993. https://doi.org/10.5281/zenodo.15058274
 10.5281/zenodo.15058274
10.5281/zenodo.15058274
