UG Student of Rashtriya College of Pharmacy, Hatnoor.
Liquid biopsy, consisting in the non-invasive analysis of circulating tumor-derived material (the Tumor Circulome), represents an innovative tool in precision oncology to overcome current limitations associated with tissue biopsies. Within the tumor circulome, ctDNA and CTCs are the only components whose clinical application is FDA-cleared. Extracellular vesicles, ctRNA and tumor-educated platelets are relatively novel tumor circulome constituents with promising potential at each stage of cancer management. Here, we discuss the clinical applications of each element of the tumor circulome and the prevailing factors that currently limit implementation in clinical practice. We also detail the most recent technological developments in the field, which demonstrate potential in improving the clinical value of liquid biopsies. Liquid biopsy has also demonstrated utility in predicting treatment responses, monitoring minimal residual disease (MRD), and assessing tumor heterogeneity. Never the less, standardizing liquid biopsy techniques, interpreting results, and integrating them into the clinical routine remain as challenges. Despite these challenges, liquid biopsy has significant clinical implications in cancer management, offering a dynamic and noninvasive approach to understanding tumor biology and guiding personalized treatment strategies.
The liquid biopsy concept was introduced for circulating tumor cells (CTC) 10 years ago and rapidly extended to circulating tumor DNA (ctDNA) and other tumorderived products such as circulating cell-free RNA (noncoding and messenger RNA, extracellular vesicles, or tumor-educated platelets. Research on the two key components of liquid biopsy assays, CTCs and ctDNA, is a very active field, with more than 26,070 publications listed under the key phrase “CTC” and more than 5,720 for “ctDNA” in PubMed in September 2020 (i.e., on average 30 to 40 new publications each week for CTCs in 2020). These liquid biomarkers are used in more than 557 clinical trials registered at the NCI website (http://clinicaltrials.gov; 325 for CTCs and 232 for ctDNA; among them, 7 involving both biomarkers). Strong evidence for CTCs and ctDNA as prognostic markers has been documented in many tumor entities including breast, prostate, lung, and colorectal cancers. In ongoing interventional studies, the clinical utility of CTCs and ctDNA for treatment decisions is being evaluated. In particular, the use of CTCs and ctDNA as real-time liquid biopsy has received attention over the past years. Liquid biopsies present great potential in overcoming these existing sampling limitations. They consist of the sampling and analysis of liquid biological sources, typically blood, for cancer diagnosis, screening and prognosis.
1.1 ) Historical context: From Traditional biopsies to Liquid biopsies. Background Traditional methods of cancer diagnosis and monitoring have primarily relied on tissue biopsies, which involve the surgical removal of a sample of the tumor for analysis. While tissue biopsies remain the gold standard for cancer diagnosis, they are limited by several factors, including their invasive nature, the possibility of tumor seeding, sampling errors, and a small risk of morbidity associated with tissue biopsy procedures. These limitations underscore the need for noninvasive and dynamic approaches that can provide a more comprehensive picture of the disease. In addition, tissue biopsies typically obtain a sample of only a part of the tumor, thus only encompassing a part of tumor heterogeneity, limiting the information obtained on the levels of genetic and epigenetic variability of a patient’s cancer. Liquid biopsy offers advantages over traditional tissue biopsies, providing a minimally invasive, dynamic, and comprehensive molecular analysis of tumors, aiding in early diagnosis, prognostication, and treatment response monitoring. By analyzing biomolecules shed by tumors into the bloodstream, liquid biopsy provides valuable information about the genetic alterations, variational profiles, and treatment response of cancer cells. Moreover, liquid biopsy can be performed after surgical resection and when there is no detectable metastatic mass for cancer treatment monitoring. Due to its minimally invasive nature, liquid biopsy can be performed multiple times or sequentially, which allows for continuous monitoring of disease progression as well as the emergence of treatment-resistant clones, offering insights that can be used to guide clinical decision-making. With the less invasive obtaining method and the various analytes that can be sampled in liquid biopsy, it can be used as a routine method for the real-time monitoring of cancer progression, early diagnosis of cancer, and assessing treatment response.
2). Keybiomarkers in liquid biopsies :
2.1) ctDNA : Highly sensitive and specific methods have been developed to detect ctDNA, including BEAMing Safe-Sequencing System (BEAMing Safe-SeqS), Tagged-Amplicon deep Sequencing (TamSeq), Cancer Personalized Profiling by deep Sequencing (CAPP-Seq), and digital PCR to detect single-nucleotide mutations in ctDNA or whole-genome sequencing to establish copy-number changes. In addition to mutation analysis, reliable tests for the assessments of epigenetic changes such as DNA methylation have been developed over the past years. For example, Luo and colleagues analyzed methylation patterns on ctDNA from multiple large cohorts of patients, including a prospective screening cohort of people at high risk of colorectal cancer. A methylation-based diagnostic score was identified and validated to help distinguish patients with colorectal cancer from healthy controls, as well as a prognostic score that correlated with patients’ survival.
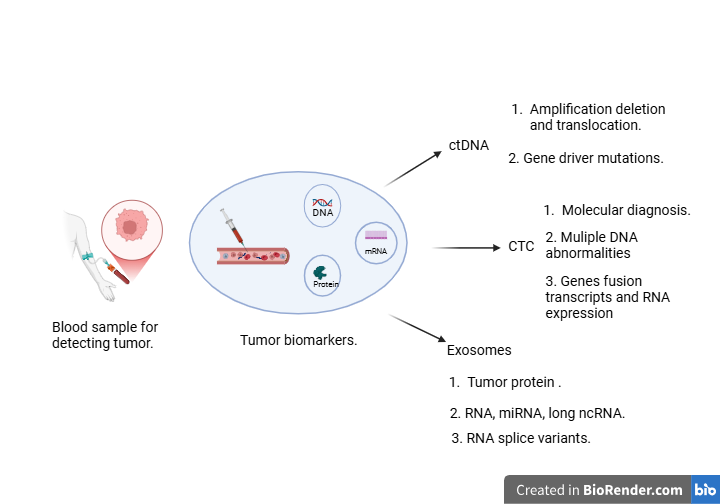
Fig no. 1
2.2) CTCs : CTCs are shed from either primary or secondary tumor sites; they migrate into the circulatory sys tem and are responsible for the development of distant metastases.11 CTCs are extremely rare, occurring at a frequency as low as 1 CTC per 106–107 leukocytes, with even lower numbers in early stage diseases.12 Initially assessed as nonleu kocytic, nucleated cells of epithelial origin, CTCs do not have well defined morphological aspects and they may vary according to cancer type and stage.11 CTCs may also cluster either with paren tal tumor cells or with fibroblasts, leukocytes, endothelial cells or platelets, forming aggregates with higher propensity to seed distant metastases than single CTCs, thanks to a their survival advantage13 and to the protection from the immune system and oxidative stress.14,15. However, CTCs provide an ideal approach to molecular cancer diagnosis and treatment options, and their investigation is widespread in cancer research. Based on their properties, several systems have improved their detection and isola tion, utilizing their physical differences compared with leukocytes,16 including antigen expression. The major differences are their large size, up to 20–30 µm, mechanical plasticity, and dielectric mobility properties compared with blood cells.17–20.
2.3) exosomes and microRNAs :
Exosomes increasingly referred to as small extracellular vesicles have captivated the interest of biomedical researchers particularly because they carry microRNAs (miRNAs) associated with cancer processes such as angiogenesis and metastasis. As reported, with a certain number of cancer-specific biomarkers, tumor cells may produce more exosomes than normal ones. Tus, exosomes have been recognised as the most promising and basic indicators for the diagnosis of patients because they are easily accessible and preserve stability in invitro. Exosomal miRNAs have been discovered in all human physiological fluids, including plasma, serum, urine, saliva, bile, breast milk, and cerebrospinal fluids, and are being exploited as non-invasive tumour indicators. Because of the prevalence of exosomes in such fuids and the stability of miRNAs, exosomal miRNAs may provide a unique class of biomarkers for early and less invasive cancer diagnosis. This review appraises recent studies on potential of exosomal miRNAs as diagnostic and prognostic biomarkers in cancers, including like lung, breast, prostate, oral squamous cell carcinoma (OSCC) and colorectal cancer (CRC). Biogenesis of exosomes are endosomal-derived lipid bilayers with diameter of 40–100nm that contain a wide range of bioactive molecules such as nucleic acids, lipids and proteins. Exosomes are secreted from all cell types namely immune cells, tumor cells and epithelial cells and are also found in biological fuids like plasma, serum, urine, saliva, bile, breast milk and cerebrospinal fuids. In relative to healthy proliferating cells, tumour cells generate an excessive number of exosomes. Exosomes carry cargos (proteins, lipids and nucleic acids) from donor to destination cells via target cell membrane fusion, and hence play a role in cell-cell communication and the regulation of numerous physiological functions. Exosome biogenesis is a two-step process. At first, the development of early exosomes begins with the manifestation of the cell membrane. The inward introversion of endosomal membranes results in the formation of multiple intraluminal vesicles (ILVs), which contributes to the creation of multivesicular bodies (MVBs). Cytosolic constituents like as nucleic acids, proteins, and lipids can be processed into ILVs during this mechanism. MVBs merge with the plasma membrane, delivering ILVs into the extracellular environment. Exosome biogenesis has been linked to a number of causes.
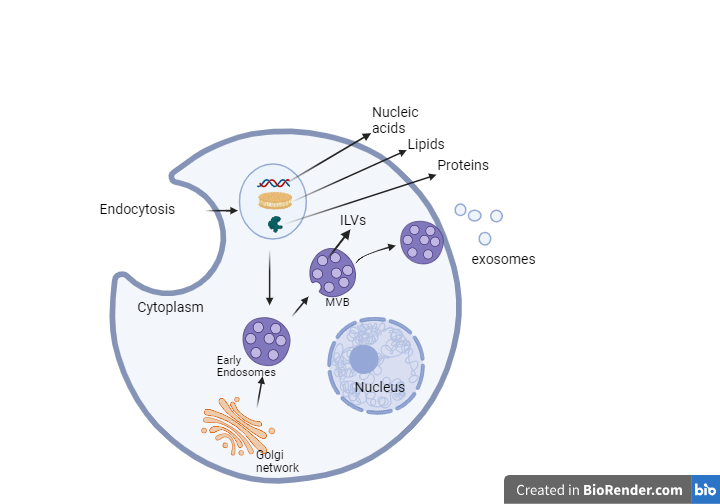
Fig no. 2
cfDNA and other biomarkers : Circulating cell-free DNA (cfDNA) in human body fluids (e.g., plasma) was discovered long ago. Studies found that in healthy subjects, most of the cfDNA molecules in plasma originated from the hematopoietic system however, in certain clinical scenarios, such as pregnancy, organ transplantation, and cancer, the related/affected tissues would release additional DNA into the plasma pool. The detection of this perturbation would allow one to diagnose the abnormality of a subject in a noninvasive manner. In recent years, methods based on the analysis of cfDNA have been largely explored as an emerging technology for noninvasive prenatal testing (NIPT), organ transplantation monitoring, as well as cancer liquid biopsy. For instance, the plasma DNA based fetal aneuploidy test in pregnant women was routinely deployed in more than 60 countries by 2014, and the market value is estimated to reach 3.6 billion USD in 2019. Studies that use plasma cfDNA for cancer testing and tumor origin determination have also demonstrated high clinical potential. In these studies, a variety of approaches were developed for differentiating the cfDNA molecules released by the tissues-of-interest (e.g., circulating tumor DNA (ctDNA) in cancer patients) from the background ones, especially with the advancement of digital PCR (dPCR) and parallel sequencing technologies. Previous studies have suggested that cfDNA molecules were mostly generated through cell apoptosis. The endonuclease enzymes functioning in the apoptotic DNA fragmentation procedure showed cutting preferences on the inter-nucleosomal DNA, while not that bound (or protected) by the histones and thus, led to the coverage imbalance and specific ending patterns of cfDNA. Using a combined analysis of the cutting event and coverage pattern, Snyder et al. proposed a measurement strategy called the “Window Protection Score” to profile the nucleosome positioning from cfDNA. Considering that the nucleosome positioning pattern is highly related to the cell identity Snyder et al. further showed that they were able to trace the tissue origin of cfDNA which showed potential in deducing the tumor origin in cancer patients. In another study, Ulz et al. demonstrated that different nucleosome occupancy in the promoters of expressed and silent genes resulted in differences in the plasma cfDNA coverage. Therefore, through investigating the coverage pattern of the tissue-specific promoters, one would be able to infer the tissue origin of cfDNA.
3). Technology enabling liquid biopsies :
NGS (next generation sequencing): Although PCR-based methods are sensitive and inexpensive, they can only screen for known variants, and the input and speed are limited. NGS has high throughput and can screen unknown variants. Currently, NGS is able to detect MAF < 1% . Furthermore, many methods like unique molecular identifiers or unique barcodes can help to increase the sensitivity and reduce the false negatives. These methods are able to detect 59% of stage I or II lung cancer patients with MAF around 0.1% and have good agreement between ctDNA response and radiographic response. NGS can be applied to the targeted panel for specific and highly sensitive detection of targeted ctDNA mutations. Many methods are applying NGS to target panel, namely Tagged-Amplicon deep sequencing (TAm-seq), Safe-Sequencing System (Safe-SeqS), CAncer Personalized Profiling by deep sequencing (CAPP-Seq), and Ion Torrent. For TAm-seq, researchers first design special primers to amplify regions of interest. In order to control sampling errors and allelic loss, the primers are first used to bind to the template during a preamplification step to amplify the original signal. Next, the templates undergo individual amplification for purification. Benefiting from this two-step amplification design, TAm-seq may able to identify mutations ~ 2% MAF with sensitivity over 97% . The enhanced version of TAm-Seq, named eTAm-Seq™ can detect MAF as low as 0.25% with a sensitivity of 94%. In addition, it has been revised to identify single-nucleotide variants (SNVs), short insertions/deletions (indels), and copy number variants (CNVs). For Safe-SeqS, the key idea is adding a unique identifier (UID) to each template. After amplification, if a mutation does not appear in most of the same UID-connected sequences, it is likely to be induced by other errors. In this way, Safe-SeqS reduces the sequencing errors by at least 70-fold and has sensitivity as high as ~ 98% for detecting tumor mutations. CAPP-Seq is a combination of the library preparation method and a specialized bioinformatics workflow. The library generates many hybrid affinity captures of recurrently mutated genomic regions from the population of interest to create a “selector.” The “selector” is applied on tumor DNA to identify individual-specific mutations as prior knowledge. Then, it is applied ctDNA for quantification. CAPP-Seq can detect MAF ~ 0.02% with a sensitivity of nearly 100% among stage II-IV NSCLC patients. Ion Torrent is an NGS platform developed by Thermo Fisher Scientific. It allows CNVs, single-nucleotide polymorphisms (SNPs), indels, and fusion detection with as little as 1 ng DNA input. One study applied this platform covering 2800 COSMIC (the Catalogue Of Somatic Mutations In Cancer) mutations from 50 cancer genes to successfully identify 71% of metastatic breast cancer patients . Another study covered more than 6800 COSMIC mutations of 46 genes. About 97% of mutations identified in metastasis biopsies were detected in matched ctDNA in the study. However, researchers who compared dPCR with Ion Torrent concluded that dPCR was more sensitive and can detect smaller MAF for some targeted panels. Although targeted panels may be preferred for their high sensitivity and low cost, they can only detect point mutations and indels. One unique advantage of NGS is that it can be applied to the untargeted panel to find genome-wide DNA variation. Whole-genome-sequencing (WGS) is usually used to get the whole genomic profile of tumor DNA including point mutations, indels, rearrangements, and CNVs. Although WGS provides us with abundant information, it is expensive and less sensitive. Whole-exome sequencing (WES) is a popular alternative of WGS. It is less expensive by only sequencing the exons. Nevertheless, both WGS and WES require high input sample volume, hindering their application in screening and early diagnosis when the concentration of ctDNA is considerably low. Many genome-wide sequencing methods have been proposed for different variation types like PARE (personalized analysis of rearranged ends) for the detection of rearrangement, digital Karyotyping for DNA content quantification, and FAST-SeqS (Fast Aneuploidy Screening Test-Sequencing System) for the detection of CNVs. PARE first uses next-generation mate-paired sequence analysis to identify individualized rearrangements from tumor tissue. Then, it applies PCR for quantitatively monitoring the detected rearrangements. It is highly sensitive for detecting ctDNA lower than 0.001% in patient plasma samples. Some studies suggested that ctDNA at levels > 0.75% could be detected in cancer patients with sensitivity over 90% and specificity over 99%. Even a single copy of rearrangement from ctDNA can be detected without false positives. Digital karyotyping is a quantitative approach to detecting genome-wide abnormalities at high resolution, including unknown chromosomal changes, altered regions, and DNA sequences. It uses two enzymes to cut the DNA into short fragments around 10 kb and ligates each fragment with a tag. The tags help to align the DNA fragments back to the genome and detect abnormalities in DNA sequence through their density. Orthodenticle homologue 2 (OTX2) amplification was identified in medulloblastomas using digital karyotyping. The overexpression of OTX2 was later confirmed to be causal for certain medulloblastomas type. FAST-SeqS (Fast Aneuploidy Screening Test-Sequencing System) can discriminate as low as 4% of trisomy 21 DNA from euploid samples. The key is simplifying the library preparation steps by only using one designed single primer pair to amplify the repeat regions of interest, so that the cost can be controlled while increases the throughput. There is an updated version of FAST-SeqS called modified FAST-SeqS (mFAST-SeqS). Unlike methods like PARE for quantification of target mutations predetermined by sequencing tumor tissue, mFAST-SeqS is an untargeted method to monitor residual disease or treatment response. Compared with the targeted approaches that can detect MAF as low as 0.01% to 0.5%, untargeted approaches can only detect MAF > 10%. Nevertheless, untargeted approaches require no prior knowledge and can develop genome-wide copy number pattern or assess mutation spectra.
Digital PCR and quantitative PCR : Ultrasensitive sequencing technologies are crucial for the analysis of ctDNA due to the low abundance of ctDNA in biological samples. These technologies, such as ultradeep massively parallel sequencing with unique molecular identifier tagging enable the detection and quantification of minute amounts of ctDNA, which are typically released into the bloodstream by tumor cells undergoing cell death. By utilizing ultradeep coverage sequencing methods, such as Illumina (San Diego, CA, USA) and Thermo Fisher (Waltham, MA, USA), researchers can achieve comparable performance to droplet digital PCR (ddPCR), like Bio-Rad (Hercules, CA, USA)’s QX200 and Thermo Fisher’s QuantStudio, for the detection and quantification of ctDNA from cancer patients. For accurate identification of and quantification of genetic changes in ctDNA, the ultrasensitive nature of these sequencing technologies is essential, providing insight into tumor dynamics, treatment response, and disease progression based on the molecular profile of ctDNA, which ultimately guides personalized therapeutic strategies. qPCR was performed in accordance with the Minimum Information for Publication of Quantitative Real-Time PCR Experiments (MIQE) guidelines. The reaction volume was set as 20 μL and each reaction contained 1× Taqman Universal PCR mastermix (cat # 4304437, Life Technologies, Carlsbad CA), 900 nM final concentration forward and reverse primers, 200 nM Probes and 6 ng template DNA. At least one PCR No Template Control (NTC) was run for each assay as controls on all plates. All qPCR analyses were performed in triplicate on a real time PCR system (Model 7500 Fast, Thermo Fisher Scientific®). qPCR thermal cycling conditions were as follows: 95 °C for 10 min, followed by 40 cycles of 95 °C for 15 s, 60 °C for 1 min. The SDS software v2.4 (Life Technologies) was used to calculate the quantification cycle (Cq) value. Invalid PCR results indicated by high cycle threshold (CT) values > 33 were omitted from the analysis.
Microfluidics and cell capture technologies :
4) Applications in early cancer detection :
Liquid biopsies in earlystage cancer identification :
Most cancers can be classified according to the stage of disease, a measure of how widely it has spread in the primary organ and beyond: stage 0 (i.e., in situ), I, II, III and IV. Localized disease refers to cancer that is contained where it started with no sign of spreading (Stages 0-I-II). Regional disease represents spread of the cancer to nearby, organs, tissue, or lymph nodes (Stages II-III). Distant disease is often referred to as metastatic cancer and relates to cancer which has spread to other areas of the bodies (Stage IV). Higher stage cancers are more difficult to effectively treat. As the tumor stage progresses from I to IV, the growth rate increases and the time period to the next stage decreases .
Potential for population wide cancer screening:
Colorectal Cancer : The EFGR signaling pathway also plays a role in colorectal cancer, but here mutations in the EGFR gene itself are less important for response to EGFR-targeting therapies, whereas gene mutations in the gene encoding the downstream signaling molecule KRAS are known mediators of resistance. KRAS mutations have been detected on CTCs and then became prime targets for ctDNA analyses in colorectal cancer. Sequential assessment of ctDNA in patients with advanced colorectal cancer receiving anti-EGFR therapy revealed the development of resistance, which could be reversed by drug breaks. Recently, the genomic evolution of individual metastases during HER2 blockade was revealed by ctDNA analysis. Thus, real-time monitoring of ctDNA (and CTCs) can provide insights into tumor evolution with potential implications for cancer therapy. For more information, we refer you to the recent whitepaper of the NCI colon and rectal–anal task forces that outlined the current ctDNA applications and integration in colorectal cancer.
Breast cancer : The ER signaling pathway is the main driver of tumor growth in 70% to 80% of breast carcinomas classified as ER+. Recent work has identified mutations in the ESR1 gene that confer resistance to endocrine therapies and can be detected on ctDNA. For patients who become resistant to endocrine therapy, CDK4/6 inhibitors have been recently approved for therapy, and mutations in the PI3K gene are known to confer resistance to this new form of therapy. These mutations have been detected first in CTCs and recently also on ctDNA with remarkable results toward the development of a predictive biomarker. As demonstrated in a retrospective analysis of samples from the phase III PALOMA-3 trial in advanced ERpositive breast cancer, a decline in PIK3CA ctDNA levels compared with baseline after 15days of treatment with palbociclib and fulvestrant was predictive of PFS. ER protein expression has been determined routinely for decades by immunohistochemistry. Interestingly, only 1% of primary tumor cells have to express ER to be classified as ER+. Thus, it is conceivable that ER+ tumors shed ER− CTCs which are the source of ER− metastases that may arise after years of ER-targeting therapies. Indeed, ER− CTCs were found in patients with breast cancer with ER+ primary carcinomas. Ongoing follow-up studies will show whether these CTCs can escape ER-targeting therapies and cause relapse during or following endocrine therapy in patients with breast cancer. Endocrine therapy fails to induce a response in half of patients with HR+ MBC, and almost all will eventually become refractory to endocrine therapy. To predict resistance to endocrine therapy in patients with HR+ MBC, Paoletti and colleagues developed a multiparameter CTC-Endocrine Therapy Index (CTC-ETI) using the CELLSEARCH system. The CTC-ETI combines enumeration and CTC expression of four markers: ER, BCL2, HER2, and Ki-67. The clinical relevance of CTC-ETI is being evaluated in an ongoing clinical trial.
Prostate Cancer : The androgen receptor (AR) is the key target in prostate cancer. Most if not all tumors are hormone-sensitive at the beginning, and growth can be suppressed by hormonal therapy. However, this therapy will eventually lead to the development of castration-resistant prostate cancer (CRPC), which can still be treated by new generations of AR-targeting drugs such as abiraterone or enzalutamide. Recent work by Antonarakis and colleagues has shown that cells expressing the splice variant of ARv7 lacking the ligand-binding domain can become resistant to these drugs, and ARv7 detectable on CTCs predicted clinical outcome. Immunocytochemical detection of nuclear ARv7 expression on CTCs has been developed into a new predictive biomarker. Nevertheless, a marked intrapatient heterogeneity in ARv7 expression between individual CTCs has been reported by single-cell analysis , which may also affect clinical outcome. Besides transcriptional plasticity, amplifications of the AR gene locus could be detected in 30% to 38% of patients with CRPC, and AR mutations were identified in CTC-enriched peripheral blood samples from patients with CRPC. AR amplifications enable the tumor cells to profit from the minute amounts of residual androgens in patients receiving drug-induced castration therapy, whereas AR mutations can result in tumor cells that are refractory to androgen blockade. Thus, both types of genomic aberrations support the growth of prostate cancer cells in patients with CRPC.
Lung Cancer : NSCLC is the model tumor for the relevance of genomic aberrations (e.g., EGFR, ROS1, ALK, BRAF) relevant to cancer therapy. Work on EGFR mutations that affect response to anti-EGFR therapy (TKIs, antibodies) has therefore paved the road for ctDNA-based liquid biopsy, including the first FDAcleared ctDNA assay sLow-frequency mutations (e.g., in ROS1) or translocations (e.g., ALK) have been detected on ctDNA and CTCs, which allows an effective personalized treatment of an otherwise deadly disease. Recently, ICI has become the primary option for patients with NSCLC and has now even been explored as first-line adjuvant therapy. Promising results on the use of ctDNA (e.g., assessment of tumor mutational burden) and CTCs (e.g., assessment of PD-L1 expression) have been published and reviewed in detail elsewhere. Recently, Moding and colleagues showed that ctDNA dynamics predict benefit from consolidation immunotherapy in locally advanced NSCLC.
5) monitoring disease progression and treatment response:
Treatment selection and prognosis ctDNA :
After cancer diagnosis, ctDNA sequencing enables tumor-specific molecular profile of the patients to guide targeted therapy for precision medicine. The half-life of cfDNA in the circulation is between 16 min and 2.5 h. That is why ctDNA can be considered “real-time” snapshot to reflect the overall evolution of lesions. This enables real-time and long-term monitoring of the treatment effect, allowing feasible treatment adjustment and better prognosis. Moreover, ctDNA facilitates dynamic monitoring of the clonal evolution and helps to identify the emergence of resistant subclones. Up to now, the European Medicines Agency and the FDA have approved epidermal growth factor receptor (EGFR) mutation testing using ctDNA for therapy guidance among non-small cell lung cancer (NSCLC) patients. Moreover, some newly approved immunotherapies are known to produce different tumor response patterns from other systemic treatments. Using the regular practice of monitoring therapeutic efficacy might not be appropriate anymore. For patients treated with immune checkpoint inhibitors for NSCLC, ctDNA was shown to be an early marker of therapeutic efficacy and could better predict survival outcomes. Residual disease and risk of relapse Even when treatment is successful, relapse is still a significant threat to many cancer patients, and it is hard to detect the residual disease in time using imaging or tissue biopsy. Very few effective and reliable markers are available currently. Recent studies demonstrated that ctDNA assays were able to detect residual disease several weeks earlier than radiologic imaging, and ctDNApositive patients were at higher risk of relapse and exhibited worse outcome (like shorter overall survival and disease-free survival time) compared to the ctDNAnegative group. In addition, it was shown that phylogenetic ctDNA profiling could be used to track the subclonal nature of lung cancer relapse and metastasis. With the collected profiles, cancer patients could be stratified into different adjuvant therapies to prevent overtreatment.
Clinical Trials Evaluating Liquid Biopsy for Cancer There have been numerous clinical trials on liquid biopsy, including the detection of actionable variants, evaluating treatment response, and predicting prognosis. For instance, an ongoing clinical trial at the Jewish General Hospital in Montreal, Canada, called “TRICIA” (TRIPLE Negative Breast Cancer Markers In Liquid Biopsies Using Artificial Intelligence), is developing a test or score based on ctDNA expression within a cohort of patients with triple-negative breast cancer, which demonstrates the potential of liquid biopsy to guide treatment decisions based on specific breast cancer subtypes. Another prospective phase II clinical trial in CRC utilized liquid biopsies to detect spatial and temporal heterogeneity of resistance to anti-EGFR monoclonal antibodies by combining sequential profiling of ctDNA with mathematical modeling and imaging of tumor progression. This clinical trial showed that liquid biopsy can be used to monitor the progression of cancer and the response to treatment. Furthermore, EGFR variant status is being evaluated in NSCLC patients using the ddPCR method in ongoing clinical trials, suggesting that liquid biopsy can play a major role in guiding treatment decisions for NSCLC patients. As a result of these trials, it is evident that liquid biopsy can be useful for identifying specific variants in lung cancer patients and guiding targeted therapies.
Future Clinical Directions Following increasing availability of NGS techniques and greater understanding of the fundamental molecular pathways in cancer, there has been an increasing focus on tumor subtyping and assessment for actionable mutations. This has led, at least in part, to cancers being classified based on their molecular profiles rather than on tissue of origin and histologic subtype. A further result of this has been the establishment of so-called molecular tumor boards (MTBs) in which fundamental molecular pathways responsible for malignant transformation are identified in an individual patient and determining treatments likely to directly target these pathways. MTBs have been proliferating significantly in recent years and are likely to continue to expand and enter more routine practice. Liquid biopsy is likely to greatly facilitate this as it enables both convenient initial tumor molecular assessment and longitudinal molecular assessment. Thus, resistance mechanisms may be elucidated and, theoretically at least, directly targeted. Although limited by cost, technical challenges and availability, liquid biopsy techniques have definite and clinically relevant applications to the management of LCa both early and late stage. Thus, while it is highly likely and predictable that liquid biopsy will play a major future role in the diagnosis, response assessment and ongoing surveillance of LCa, supportive data are, at present, relatively limited. Perhaps the greatest challenge facing healthcare services is the rising cost and complexity of interventions (including the requirement for detailed molecular diagnosis) with the frequent need to repeat this assessment over time during the treatment course to say nothing of the resultant complication risk and the burden on people with the disease. In light of this, liquid biopsy techniques would appear to offer an ideal combination of convenience and safety while still providing detailed molecular information and at least reducing, if not fully obviating, the need for invasive and technically complex tissue sampling. Thus, the authors feel that liquid biopsy represents probably the major future direction in LCa diagnosis, assessment, surveillance and, probably, screening and will likely play a similar role in other malignancies. That said, further trials with greater numbers as well as “real-world” data will be required to verify this along with cost and time reductions which are the likely result of ongoing technical improvement and economies of scale.
Diagram of future direction :
Advantages and limitations of liquid biopsies : Biopsies have many advantages They are non-invasive and less expensive than traditional tissue biopsies. They have the potential to detect material shed from multiple metastatic sites rather than analyzing a small piece of tissue biopsied; therefore, liquid biopsies have the potential to better detect heterogeneity in the tumor across sites. Liquid biopsies can be obtained serially to observe changes with therapy. Liquid biopsies have potential in early cancer detection as part of screening, as well as detecting mini mal residual disease following therapy. There are also several limitations of liquid biopsies . ctDNA/cfDNA can be shed in only small amounts and not all patients will have detectable levels, especially those with low tumor burden. Because of the small amount of material shed in the circulation, sequencing can be difficult and expensive. Standardiza tion across laboratories and vendors is needed to ensure reproducibility. Not all detectable cfDNA alterations are cancer-related; indeed, cfDNA may be confounded by the mutations derived clonal hematopoiesis of indeter minate potential (CHIP), especially in older patients . Moreover, not all ctDNA/cfDNA is equally shed from the primary tumor and metastases, so it is unclear if the alterations detected accurately represent tumor hetero geneity. Shedding of ctDNA can be suppressed by treat ment and may be limited at certain disease sites. The isolation of CTCs remains technologically chal lenging, and the number of CTCs isolated can be method dependent. Surface markers may be downregulated in certain tumors, which can limit the ability to detect CTCs . It is unclear if the CTCs are uniformly shed from all areas of the primary tumor and metastases; thus, the CTCs isolated may not provide a full portfolio of tumor heterogeneity . On the other hand, CTCs can provide DNA, RNA and protein results and can be cultured for functional studies.
CONCLUSION:
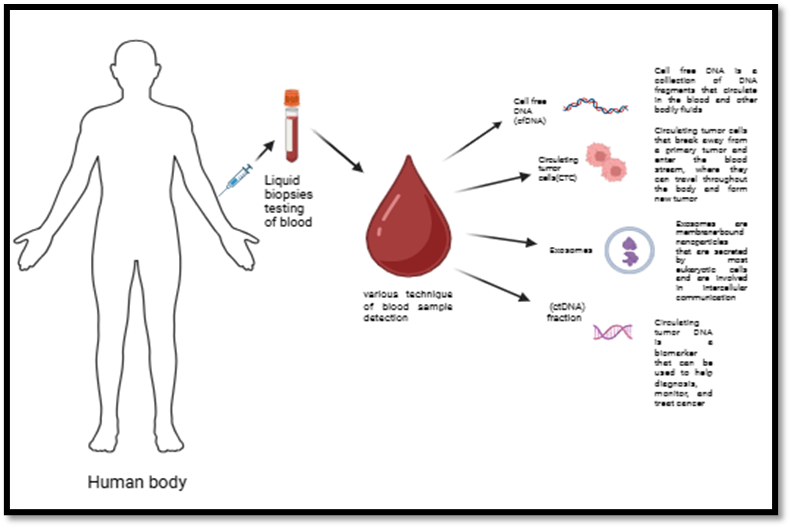
A liquid biopsy is an advanced, non-invasive diagnostic approach that involves the analysis of a blood sample to detect and characterize cancer. Unlike traditional tissue biopsies, which require a direct sample from a tumor, liquid biopsies offer a less invasive method for obtaining critical information about the presence and progression of cancer. The technique relies on identifying and analyzing various tumor-associated biomarkers present in the bloodstream, such as circulating tumor DNA (ctDNA), messenger RNA (mRNA), and exosomes. Circulating tumor DNA (ctDNA) consists of fragments of genetic material shed by tumor cells into the bloodstream. By detecting and analyzing variations in ctDNA, liquid biopsies can reveal genetic mutations and alterations associated with specific types of cancer. Similarly, mRNA detection allows for the analysis of gene expression profiles, providing further insights into tumor behavior, response to treatment, and potential resistance mechanisms. Exosomes, small vesicles released by tumor cells, also carry important biomolecular information, including proteins, lipids, and genetic material. The analysis of exosomal content can help identify tumor-specific markers and track changes in tumor dynamics over time. Liquid biopsies offer several advantages over traditional biopsy methods, including the ability to monitor tumors more frequently, detect minimal residual disease, and assess therapeutic responses with greater sensitivity. As a result, liquid biopsies are increasingly being explored for early cancer detection, prognosis assessment, and the development of personalized treatment strategies, making them an invaluable tool in modern oncology.
Highlights
Graphical abstract:
REFERENCES

Durole Payal*, S. Waghmare, M. Joshi, Gangalwar Amey, Chavan Siddhesh, Chondhe Nikita, Liquid Biopsies: Revolutionizing Cancer Diagnosis and Prognosis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 1724-1743 https://doi.org/10.5281/zenodo.15382783
 10.5281/zenodo.15382783
10.5281/zenodo.15382783
