1 School of Chemical and Biotechnology, SASTRA University, Thanjavur, Tamil Nadu, India
2 Department of Pharmaceutical Engineering, B V Raju Institute of Technology, Hyderabad, Telangana, India
Hidradenitis suppurativa (HS), otherwise referred to as acne inversa is a chronic inflammatory skin disorder affecting many parts of the body where two surfaces rub together and causes multiple systemic complications and currently has a reported worldwide prevalence of approximately 1.0%. The condition typically presents in early adulthood, presents with painful bumps, abscesses, and draining sinus tracts that commonly affect the armpit (axillary), vagina, buttocks (gluteal), and anal (perianal) areas. There is also an association with Metabolic Disease and Cardiovascular Disease that reduced the expected longevity of the patient with HS. There are several recognised contributing risk factors for progression of HS which include genetic predisposition, smoking, being overweight, and hormones. The pathophysiological process begins around the area of the hair follicle due to abnormalities of both the innate and acquired immune systems. The inflammatory mediators that are thought to initiate this inflammation are TNF, IL-1?, and IL-17(Sabat et al., 2020). The disease usually first appears after someone has gone through puberty but is often diagnosed around the age of 30 and can continue into the senile years. The nature of the disease is primarily chronic and often leads to the development of extensions underneath the skin that can cause indurations, sinus, and fistulae that drastically impacts an individual's quality of life. The treatment options for the disease will vary depending on the stage of disease when it is first diagnosed. In cases where nodular lesions appear early in the disease process (like in the beginning of the disease), antibiotics can be used for acute treatment; long-term antibacterials, zinc salts can often be used as maintenance medication; and anti-TNF medications have been recommended for severe cases of the disease. Systemic steroids, estrogens, anti-androgens, and retinoids can sometimes be employed as options, but usually with limited success. Surgical options may be used to treat abscesses that are limited in nature, but incision and drainage should only be used to treat abscesses that have not expanded beyond that point; for locally recurrent draining sinuses, limited excisions should be performed. In cases of advanced disease, total wide excision with healing by secondary intention or flaps or grafts is the only option for actual cure (Revuz, 2009).
Skin is a highly-familiar organ to the majority of people, as it is visible, and can be touched and felt. Therefore, any abnormal or damaged area of skin can have a huge impact on an individual. The skin disorder Hidradenitis Suppurativa (HS) creates significant changes to the skin. HS is classified as a chronic inflammatory disease that results in painful and recurring nodular lesions, pus-filled abscesses, and sinus tract (fistula) formation within the areas of the body that often come into contact with each other, such as the armpits, groin, under the breast region, and genitals/anus.1 While HS has been the subject of extensive epidemiological, translational, and clinical studies over the past decade, there continues to be a significant lack of awareness of HS in both the medical community and in general public. HS has a profound effect on the social and occupational lives of the vast majority of sufferers, and the majority of sufferers are young and middle-aged adults. Along with its high burden of cutaneous disease, HS has also been linked to numerous comorbidities, including: metabolic disease; cardiovascular disease; musculoskeletal disease; gastrointestinal disease; and several mood- related disorders. With an estimated worldwide prevalence of approximately 1 percent, HS has significant socioeconomic impact on society(Sabat et al., 2020).
When making therapeutic decisions for patients with hidradenitis suppurativa, clinicians should consider both the degree of involvement of the disease and the level of symptom burden and quality of life impairment due to HS for that patient. Topical antibiotics have been evaluated for HS treatment; among the topical antibiotics, only clindamycin has been systematically studied for use in HS. The greatest clinical benefit of clindamycin has been seen in patients with superficial inflammatory lesions--such as folliculitis, papules, and pustules-- and little or no benefit in patients with deeper pathological features such as nodules and abscesses. Thus, topical clindamycin is recommended for patients diagnosed with localized disease, which includes patients classified as Hurley stage I and some patients at Hurley stage II who have not been treated successfully with other medications. Topical therapies and a host of systemic options have also been thrown into the mix. Systemically, clinicians can consider use of antibiotics, such as tetracycline and ertapenem; immunomodulatory and anti- inflammatory agents, such as cyclosporine and dapsone; and retinoids, such as acitretin and isotretinoin, as systemic options in the management of HS. A new wave of treatments including the use of biologics and biosimilars such as monoclonal antibodies (mAbs) have risen (Napolitano et al., 2017).
THE EPIDEMOLOGY OF HIDRADENITIS SUPPURATIVA
Estimates of the number of people who have Hidradenitis Suppurativa (HS) have improved in the past few years, but still vary greatly from place to place. This is due largely to geography, but more importantly to how researchers have gathered data. The majority of studies that use medical diagnosis codes that are applied to abnormal tissue have lower prevalence rates for HS, because it has not been fully recognized in most clinics. Surgeons, doctors, and clinics typically do not identify HS until the patient has developed excessive swelling and/or infection. Studies that measured prevalence rates utilizing questionnaires that used self-reported symptoms produced higher estimate results because of potential misclassifications of the disorder. In relation to this type of research, questionnaires that identify HS using self-reporting have shown only a positive predictive accuracy of between 27% and 67%, indicating that more research is needed to validate the accuracy of these self-reported measurements. Most epidemiologic research has analyzed data collected from populations located in Europe and the United States. Within European cultures, rates obtained by large cohort studies range from 1.0% – 2.1%. The rates for registries using diagnostic coding are much lower and range from 0.09% – 0.51%. In the United States, early prevalence estimates using clinical coding systems show that the prevalences exist at a level of approximately 0.1%. The prevalence data collected in South America show similar variability to that in North America. The rates in South America vary from 0.007% based on Diagnosis Reporting to a rate of 0.41% based on self-rereported data. The survey studies conducted in Africa reported rates of prevalence of HS between 0.67% – 2.2%. In stands to reason that the survey-derived estimates from East Asia (not including Japan) have been reported to be lower compared to the estimates from the rest of the world with the estimated prevalences in East Asia reported at 0.14%. Regional differences also exist in the prevalence of HS according to gender. In many populations around the globe, the prevalence of the condition has been found to affect women two to three times more than men. The female-to-male prevalence ratio in central Europe, however, is 1.5. Noteworthy is the fact that the reverse has been found in some Asian nations. In the US, African Americans are the ones most affected by the condition. This disparity can be attributed to the complex pathogenesis of the condition. Lifestyle and healthcare factors could also significantly impact the above-mentioned findings (Sabat et al., 2020).
Hidradenitis Suppurativa is estimated to affect between 0.5% – 4% of the population, but this is probably on the low side due to a substantial amount of missed diagnoses and insufficient reporting. The typical age range for the onset of this disease is from Puberty to 40 years of age. However, the highest rate of occurrence appears to be 21-29 years. Female patients appear to be affected by Hidradenitis Suppurativa approximately three times more frequently than males, and the absence of studies indicating any racial or ethnic predisposition is probably due to the misdiagnosis; studies have likely failed to include patients of Black or Hispanic descent (Ballard K et al., 2025).
ETIOLOGY AND PATHOPHYSIOLOGY
The etiology of hidradenitis suppurativa seems to be affected by genetic, environmental, and behavioral factors. A prevalence of 33% to 40% of affected family members in first-degree relatives with hidradenitis suppurativa has been noted, making it autosomal dominant. A loss- of-function mutation in the γ-secretase complex, a Notch signaling pathway, has been found in a few families with hidradenitis suppurativa. The genes mutated in hidradenitis suppurativa are the genes encoding dermcidin protein (DCD), PSTPIP1 protein responsible for hidradenitis suppurativa syndrome, SOX9, and KLF5. The role of environmental and behavioral aspects in the development of hidradenitis suppurativa cannot be ignored. Many patients with hidradenitis suppurativa present with associated illnesses such as obesity, resulting in skin, glandular, and nervous system-related influences in the form of skin friction, sweating, and androgen insensitivity. Hidradenitis Suppurativa has also been linked with the presence of Metabolic Syndrome, which has become more common in the obese population. Smoking appears to increase the severity of Hidradenitis Suppurativa. Nicotine is thought to enhance follicular plugging, making people who smoke have more severe and progressed disease. Female hormones appear to affect Hidradenitis Suppurativa; i.e. females are more often affected than males, have more severe and progressive forms of disease during their menstrual cycles, and are more often affected during puberty or menopause due to exogenous hormone replacement theory. There are other factors that could also trigger or increase the risk of developing Hidradenitis Suppurativa such as medications, infections (bacteria), and mechanical friction. The Pathophysiological development of Hidradenitis Suppurativa occurs when the hair follicle has a defect leading to occlusion and rupture which results in the release of keratin and bacteria into the surrounding skin. This occlusion leads to the proliferation of keratinocytes and an immune response. The increased activity and proliferation of neutrophils and lymphocytes lead to the development of an inflammatory abscess and follicular destruction involving adjacent tissue. Other probable triggers and contributing factors for the development of Hidradenitis Suppurativa include metabolic disorders, structural abnormalities of the hair follicle, hormonal influences on receptors, complement system activation, and deficiency in sebaceous glands. The evidence of immunological abnormalities suggests the presence of elevated levels of inflammatory cytokines such as Tumour Necrosis Factor Alpha and interleukins in the lesions of Hidradenitis Suppurativa, providing potential targets for treatment. While the presence of bacteria has not been considered the primary cause of Hidradenitis Suppurativa, these organisms may cause an inflammatory response in the skin and are frequently given antibiotics based on the assumption of infection, thus leading to resistant flora on the skin (Ballard K et al., 2025).
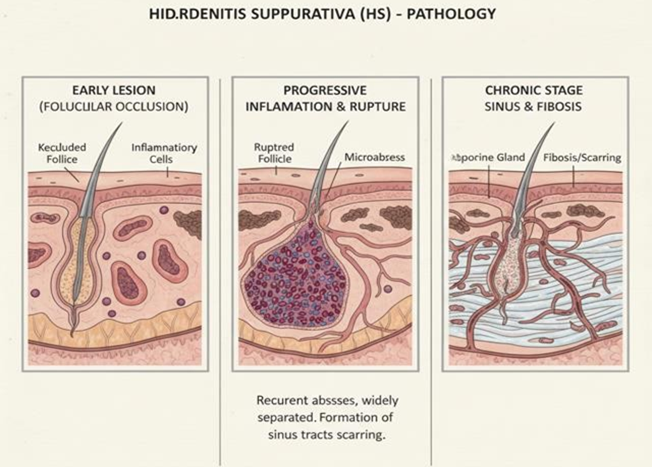
Image 1: Pathology of HS
Genetic studies on HS have unravelled loss of function in mutations in 3 out of 4 subunits of gamma-secretase, including presenilin-1, presenilin enhancer-2, and nicastrin. Type I integral membrane proteins such as Notch, E-cadherin, or CD44 are candidate target proteins. Notch is crucial for the development of normal hair follicles. Impaired Notch signalling leads to follicular keratin-enriched epidermal cysts. The occlusion of the follicular infundibulum in HS pathogenesis is beyond doubt. Independent of disease stage, follicular occlusion is an early event in the pathogenesis of the disease. A pronounced peri-folliculitis and ruptured follicles were also seen quite commonly. Hormones may induce follicular occlusion by enhanced proliferation of follicular keratinocytes. This eventually leads to intrafollicular acanthosis, keratosis, and plugging of the follicle. A very valid counterargument against the involvement of sex hormones in HS is the typical androgen profile of most HS patients. It is possible that obesity exacerbates HS due to increased skin–skin and skin–clothing friction. Human skin detects mechanical forces, including mechanical compression, friction, or shear via several Mechano-transducers. Among the different types of Mechano-transducers are various mechanically sensitive complex transmembrane receptors, including stretch-activated ion channels, integrins, growth factor (GF) receptors, and G protein-coupled receptors (GPCRs) (Prens et al., 2015).
PATHOGENESIS OF HIDRADENITIS SUPPURATIVA
The follicular occlusion tetrad is a grouping of related diseases that overlap in clinical features and share the same pathophysiology. Although they differ significantly from each other, all four are believed to be the result of blockage (occlusion) of hair follicles located in skin abundantly supplied by apocrine glands. The blockage of these hair follicles is caused by excessive amount of keratin produced by follicular epithelial cells due to abnormal conditions. This blockage prevents normal flow of fluid through the follicle, allowing fluid to become lodged in the follicle, causing the size of the follicle to increase over time. In addition to mechanical stress, increased body weight, and tobacco use, there are several environmental factors that contribute to follicular occlusion. There also is an inherent susceptibility among some people with genetic mutations that affect how keratinocyte cells grow and operate, and therefore, those people are more likely to experience blockage of their hair follicles. When an excessive amount of pressure accumulates in a blocked follicle, the follicle burst and release the cellular contents into the adjacent tissue. This initiates a strong inflammatory response that may lead to permanent damage to skin tissue. After the breach, keratin debris, lipid-rich sebum, and fractured hair shafts spread throughout the dermis and act as a signal for immune activation. The immune activation occurs due to these signals and results in chronic inflammation and immune dysfunction. The immune dysfunction further gives rise to a web of dermal sinus tracts. The chronic-ness of the condition is sustained through persistent immune cell entry and activation, mainly composed of neutrophils, macrophages, CD3+ T cells (including CD4+ and CD8+ T cells), and B cells (Jastrz?b et al., 2023).
Immune involvement in hidradenitis suppurativa (HS) can be better understood by highlighting immune infiltrates found in lesional skin. Immune cells observed in lesional skin include dendritic cells, neutrophils, macrophages, CD3+, CD4+, CD8+, and B cells. HS skin is remarkably characterised by significant dermal inflammation due to neutrophilic infiltrates. There is new evidence on HS neutrophil priming in promoting neutrophil extracellular traps (NETs), which are linked to HS severity and type I interferon response activation. NETs may contribute further to inflammation by serving as autoantigens to induce autoantibody production. There is a potential role of NETs in promoting inflammation that still requires validation. There are also adaptive immune system mechanisms that play a role in the HS disease. There is an infiltration of B cells and plasma cells into the lesional skin due to the suspected presence of autoantigens associated with NETs. These cells secrete IgG that contributes to the inflammation through the inflammation mediator pathways. Infiltration of the lesional skin is enhanced by the high expression of the IL-10 factor. The unique patterns of cytokine expression in skin lesions are a major contributor to the inflammatory process associated with HS. Frew and colleagues performed a systematic review that identified these differences in cytokine expression between the lesions themselves and surrounding, or peri- lesional skin. According to the review, the inflammatory mediators were composed primarily of keratinocytes, T cells, Dendritic cells, and Innate Lymphoid Cells. Among these mediators, the most well-studied is tumour necrosis factor-alpha (TNF-α), which has been extensively documented to induce pro-inflammatory responses. In both lesional and peri-lesional skin, TNF-α has been reported at elevated levels and contributes to the hyperkeratosis and inhibition of adiponectin release while inducing the secretion of matrix metalloproteinases and facilitating destruction of the surrounding tissue by both local and systemic responses. Although TNF-α is an important player, TNF-α expression levels in HS have not been consistently observed across studies, with conflicting reports of elevated TNF-α levels in both lesional and peri-lesional skin and peripheral blood. Based on studies in clinical settings that have used TNF-α inhibitors, such as adalimumab, it would appear that TNF-α is likely to play a much smaller role in HS than other inflammatory mediators such as other cytokines. For example, when investigating the use of adalimumab to treat HS, it has been shown that TNF-α is maintained at high levels following treatment, while other cytokines have been shown to be modulated to a much greater extent than TNF-α. Therefore, it is likely that HS is a product of an inflammatory network that includes multiple cytokines rather than simply TNF-α (Preda-Naumescu et al., 2021).
INFLAMMATORY PATHWAYS IN HIDRADENITIS SUPPRATIVA
Interleukin (IL)-1 Signalling Pathway
The NLRP3 inflammasome is a major receptor of the innate immune system and is activated when follicular debris is released from hair follicles. Following activation, NLRP3 creates a link to ASC that leads to the activation of pro-caspase-1 into the active form. Caspase-1 cleaves inactive pro-IL-1β and pro-IL-18 and turns them into their active forms. Studies have regularly detected elevated amounts of caspase-1 and increased amounts of mRNA for NLRP3 in the lesions of people with HS, indicating a heightened level of inflammasome activity. The IL-1 pathway is upregulated in patients with HS, and plays a critical role in recruiting immune cells to damaged skin and causing tissue damage. The IL-1 family of cytokines includes many pro- inflammatory cytokines such as IL-1α, IL-1β, IL-18, IL-33, and IL-36 (α, β, γ) as well as many regulatory/antagonist cytokines including IL-1ra, IL-36ra, IL-37, and IL-38. IL-1α is a crucial cytokine that activates the inflammatory response by inducing other pro-inflammatory cytokines such as TNF-α and IL-18. The majority of the IL-1β that is produced stems from monocytes and macrophages and initially recruits neutrophils, while at the same time stimulating the production of both chemokines (CXCL1, CXCL6) and matrix metalloproteinases, thereby promoting immune infiltration and tissue destruction. The levels of IL-1β have been shown to be elevated in the lesions of HS and at least 3cm surrounding the lesions as well as in serum from patients with HS. Flame is activated systemically Reduced levels of IL-1α have been shown in lesional tissue, although it is believed to be due to intracellular activation within active inflammatory sites. There appears to be conclusive evidence that keratinocytes constitutively overproduce IL-1, thus sustaining a positive feedback loop between the cytokines of IL-1 and IL-17. Among various cytokines of the interleukin-1 family, IL-36 has proven to be of prime significance, which activates NF-κB or MAPK pathways. Elevated levels of various isoforms of IL-36, as well as reduced levels of antagonistic cytokines, have been noticed in HS skin as well as serum. IL-18, another cytokine that requires the involvement of the inflammasome, is known to promote Th1 and CD8+ T-cell and natural killer-cell cytolytic functions as well as stimulate interferon gamma production. Overexpression of IL-18 has been documented in HS lesions and lends further credence to the importance of the dysregulation (Del Duca et al., 2020).
TNF-α and IFN-γ
Both TNF-α and IFN-γ seemingly play a significant role in the pathogenesis of HS. The levels of TNF-α correlate directly with the severity of HS; therefore, this clinical effectiveness of TNF-α antagonists supports an important role for TNF-α in HS. Current biologic medication treatment (currently the only one with FDA approval) Adalimumab (Humira) works as a TNF- α antagonist, which, again, points to TNF-α's significance by way of its clinical usefulness as an HS treatment. TNF-α plays a critical role in dysregulating the immune system because it can upregulate the ratio between Th17 cells to regulatory T cells and upregulate chemokine production by keratinocytes, driving the recruitment of neutrophils, monocytes, and T lymphocytes into lesions of HS and leading to dense immune infiltrates within lesions. IL-12 and IL-23 produced by dendritic cells promote the differentiation of Th1 cells and Th17 cells, respectively. IFN-γ, produced mainly by Th1 cells, promotes activation of the endothelium and recruitment of macrophages, along with driving immune cell trafficking via the production of CXCL10 (Del Duca et al., 2020).
IL-17/IL-23 Axis
It is emerging that Th17 inflammation is more prominent in HS than Th1. This is due to the presence of high levels of Th17 cells in lesional dermis, which are strongly linked with neutrophil infiltration as well as purulent drainage. IL-23, IL-1β, and IL-6 secreted from innate immune cells are key in triggering their development. The Th17 pathway modulates the production of several inflammatory mediators: IL-17, IL-22, antimicrobial peptides, and chemokines. IL-17 promotes the production of LL-37, S100 proteins, and other inflammatory mediators by keratinocytes, which contribute to hyperplasia and the infiltration of immune cells into the dermis and epidermis. The overexpression of IL-17 has been found in lesional, perilesional, and non-lesional areas, indicating the existence of subclinical inflammation before the establishment of visible lesions. The overexpression of IL-17 in the serum indicates the existence of an immune response, but inconsistent results have been obtained from a few studies. Il-23 secreted by macrophages is highly induced in HS lesions, with major roles in driving Th-17 immunity. Both skin and serum levels of Il-23 chain expression are shown to be upregulated, which strongly imparts a role to Il-23/Il-17 in HS pathogenesis (Del Duca et al., 2020).
IL-6
IL-6 is a multi-functional cytokine involved in the initiation of an acute-phase response; it also activates B cells and differentiates T helper 17 cells (Th17). However, when in concert with IL-1β, TGF-β, and IL-23, IL-6 induces the development of the Th17 lineage while simultaneously inhibiting the development of regulatory T cells. There are conflicting reports as to the involvement of IL-6 in HS. Some have noted increased levels of IL-6 within inflammatory lesions, and in the serum of patients with HS; while at the same time, other reports have demonstrated that patients with HS possess lower levels of IL-6 produced by local tissue and defective secretion of IL-6 from patient-derived monocytes. However, the fact that there is currently a heightened level of IL-6 circulating within the blood of HS patients supports an ongoing contribution of IL-6 to maintaining systemic inflammation and promoting granuloma formation. Additionally, this is further substantiated by HS' concomitance with other inflammatory diseases that are IL-6 driven, and therefore possess a shared pathway of pathogenesis (Del Duca et al., 2020).
IL-10 and Regulatory Cytokines
Unlike other inflammatory conditions of the skin, HS is distinguished by an accompanying elevation of anti-inflammation mediators, including IL-10. IL-10 inhibits cytokine production by monocytes and macrophages; inhibits T cell activation; promotes differentiation of T cells with regard to regulation. Additionally, elevated levels of IL-10 produced by the HS tissue itself have been noted in the area around lesions; this elevated level of IL-10 reflects the adaptive response to ongoing chronic inflammation and bacterial insult to the skin. Moreover, elevated expression of IL-10 can contribute to the suppression of IL-17 and IL-22 signalling. A decrease in IL-22 concentration can cause down-regulation of AMP production and impairment of epithelial barrier repair effects; thus, increased spread of bacterial infection cannot occur. This deficiency may be attributed to a lack of Notch signalling and decreased numbers of IL-22- producing cells infiltrating. Neither the precise mechanism of action of IL-10 nor the precise mechanism by which elevated IL-10 in HS skin affects overall health has been determined through studies of serum. The actions of other regulatory cytokines associated with HS, such as IL-4 and IL-13, may also affect the inflammatory component of HS through inhibition by IL-1β expression and augments of IL-1ra expression. Future studies are needed to elucidate the exact role of IL-4, IL-13, and other anti-inflammatory pathways in HS (Del Duca et al., 2020).
DISEASE STAGING
The Hurley staging system is one of the first tools widely used to assess whether hidradenitis suppurativa is mild, moderate, or severe based on how many areas of the body (anatomical area) are affected by hidradenitis suppurativa. The classification was originally intended to help physicians decide what kind of treatment should be given to patients based on which stage they are in. The classification recommends medication management for stage I, localized surgery for stage II, and extensive surgical excision for stage III. The ease of use and the speed at which this classification can be applied makes it ideal for use during routine clinical visits.
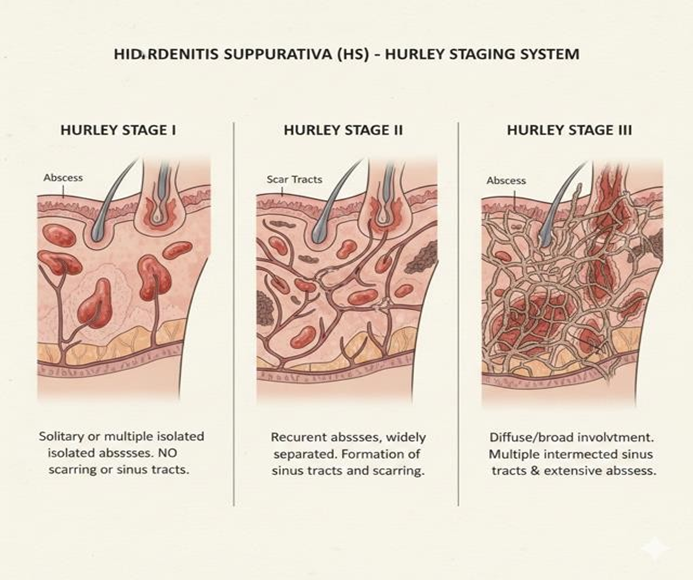
Image 2: Pictorial depiction of disease staging
Table 1: Disease staging of HS using Hurley method.
|
Stage |
I |
II |
III |
|
Abscess |
Single or multiple |
Single or multiple, widely separated, recurrent |
Diffuse or near- diffuse involvement |
|
Sinus tracts |
– |
+ |
Multiple interconnected |
|
Cicatrization |
– |
+ |
+ |
|
Area |
|
|
Entire area |
|
Treatment |
Medicinal therapy |
Combined medicinal and local surgery |
Combined medicinal and wide surgery |
TREATMENT OF HIDRADENITIS SUPPURATIVA
Based on the experiences of patients, treatment with both clindamycin (oral 300 mg twice per day) and rifampicin (oral 600 mg once per day) had been effective in treating patients who were diagnosed with Hurley Stage I (extensive stage) or Stage II (mild) and combined these two antibiotics as part of the patient's overall treatment plan. The duration of treatment was usually twelve weeks, which resulted in remission rates of nearly fifty percent and some patients reporting a partial response. The results of other clinical investigations confirmed that more than 70 percent of institutionalized patients had a positive response to their course of combined treatment with clindamycin and rifampicin during the 12-week follow-up evaluations. In our sample population, the sex of the patient was a significant predictor of response to the combined treatment while (by using the calculated odds ratio for the population of patients) the stage of the disease, body mass index (BMI), and distribution of lesions did not correlate with an increased or decreased risk of responding positively to the combined treatment. Continued improvement in a portion of patients after discontinuation of treatment was observed through long-term follow-up. However, relapse was also common in the following several months after the end of the treatment course (Napolitano et al., 2017).
Rifampicin 10 mg/kg daily, moxifloxacin 400 mg daily, and metronidazole 500 mg three times daily for 6 weeks, then a course of rifampicin-moxifloxacin, has proved efficacious, with a complete remission in 16 of 28 patients (57.1%) with long-standing refractory HS and in 14 of 16 patients (87.5%) with Hurley stage I and II, respectively. One trial demonstrated the effect of ertapenem 1 g per day IV for 6 weeks in reducing Sartorius scores from a median of 49.5 to 19.0 in a group of 30λ?α of severe HS. In total, 67% (29 of 43) and 26% (13 of 50) of FS of Hurley I and II patients' areas attained clinical remission. (Napolitano et al., 2017).
Acitretin could be used for early-stage HS patients (Hurley I or mild II); however, one could rationally suggest the use of this drug for patients with the chronic phase of HS with recurrent abscesses with sinus tracts, even connected, and/or scar formation. Dosing regimens of 0.25–0.88 mg/kg/day for 3–12 months have been used in clinical studies related to acitretin therapy for patients with Acitretin studies included a total number of 46 patients, which stated a moderate to good response rate with marked improvements noted in 28 out of 46 patients (60.9%) treated. However, recently, in a 5-year retrospective study carried out in a tertiary medical institution on 14 patients with Hurley II–III HS, acitretin monotherapy was proven ineffective for the treatment for acitretin, which efficiency was enhanced when used additively to other systemic therapies (Napolitano et al., 2017).
Favourable effects of cyclosporine are noted in individual cases. Recently conducted exploratory retrospect studies with a period of 4 years in three departments of dermatology with special interest in HS demonstrated that in patients treated with cyclosporine, 50% experienced some effect (slight improvement) in the disease in 9/18 cases. Hence, it is recommended to hold cyclosporine in reserve until more data becomes available when failure to respond to the first, and second line of treatment is observed. Anti-TNF-alpha biologics, such as adalimumab and infliximab, have been proven to have therapeutic efficacy among patients with moderate-to-severe hidradenitis suppurativa (Hurley stage II-III), with improved clinical responses and quality of life. In the two medications, however, adalimumab is more tolerable. Cumulative case-data analyses have shown that the clinical response rate of 58% is achieved with infliximab among patients with moderate-to-severe disease, albeit from post- marketing observations. Only one peer-reviewed study is available for evaluation, a phase II randomized crossover clinical trial on infliximab, with insufficient information from phase III clinical trials. Infliximab is given intravenously at a dose of 5 mg/kg at weeks 0, 2, and 6, after which maintenance doses are given every 8 weeks. Adalimumab, a fully human monoclonal antibody raised against TNF-α, is at present the only FDA-approved biologic in the treatment of HS. Response rates of about 60% are reported in case series with once-weekly administration. Its effectiveness and safety were recently demonstrated in two large multicentric trials, PIONEER I and II, which enrolled more than 600 patients with moderate to severe disease (Napolitano et al., 2017).
SURGICAL INTERVENTIONS IN DISEASE MANAGEMENT
Incision and drainage (I&D)
This can be employed in the setting of an acutely inflamed, fluctuant abscess with the goal of immediately relieving the discomfort. But because it doesn’t eliminate the pathological tissue, it doesn’t offer a long-term solution and typically leads to a recurrence rate that’s nearly universal. A lack of efficacy and equal effort make deroofing a preferred treatment option for HS over I&D. Deroofing is a minimally invasive surgical option and is used as an indication for Hurley stage I-II persistent nodules and sinus tracts. This is accomplished by making an opening in the overlying skin to expose the sinus tract and removing the overlying skin, thereby allowing the tract to heal. It can be done under local Anesthesia by means of scissors, electrosurgery, and/or carbon dioxide lasers. There have been reports showing favourable results regarding healing time, recurrence, and cosmetic outcome (Shukla et al., 2022).
Excision Techniques:
Excision involves the aim of eliminating the tissue and can be localized, wide, or radical excision based on the nature of the disease. Excisional procedures are considered in Hurley Stage I-II, wherein localized lesions are removed with good cosmetic results, but moderate rates of recurrence. Wound closure after excision may be done by second-intention healing, primary closure, skin grafting, flaps, and a combination of the two. Second-intention healing has the lowest chance of recurrence; however, this takes longer. Skin grafting heals quickly with increased post-operative discomfort and morbidity at the donor site. Flaps have the advantage of fast healing with a higher chance of ischemia and necrosis. Also, primary closure can only be applicable in small defects and has an increased chance of recurrence (Shukla et al., 2022).
Skin-Tissue-Sparing Excision
STEEP is a method of preserving tissues for Hurley stage II–III disease, involving excision of sinus tracts without excising the base of the wound. Compared with conventional wide excision, it is associated with increased healing rates, improved cosmesis, and reduced complications, although there are few long-term prospective trials (Shukla et al., 2022).
Laser and Light Therapies
CO2 laser excision and vaporization allow adequate excision of the diseased tissue with good haemostasis and with satisfactory results regarding recurrence, while additionally providing comfort after the surgery. Laser therapy acts on the follicular structures and has proved highly effective regarding reduction of disease activity and recurrence, especially in the area where the lesions are more frequent, like the groin and the axillary region. Intense pulsed light/laser and other lasering systems for the removal of hair have proved to be effective in small series and pilot studies (Shukla et al., 2022).
Cryo-Insufflation
Cryo-insufflation is a method of treating sinus tracts through the use of cryotherapy with liquid nitrogen. It has demonstrated preliminary success in the treatment of moderate to severe illnesses. While the data shows that this method appears safe and effective, further study with larger population sizes is necessary to definitively determine the effectiveness and safety of cryo-insufflation in treatment (Shukla et al., 2022).
Post-operative Care and Recovery
Effective post-operative care involves proper wound care, use of a moist dressing, prevention of infection, and early mobilization of the patient following surgery. The use of negative pressure wound dressing may help improve the survival rate of the graft and may help in the healing of the wound. Following standardized protocols for administering pain medication (analgesics) to the patient is essential. The patient is also encouraged to perform physiotherapy to reduce the risk of future contracture formation; in addition, smoking cessation and proper weight management will decrease the risk of recurrence (Shukla et al., 2022).
MENTAL HEALTH
Depression is also a comorbidity seen in association with hidradenitis suppurativa and is defined by persistent feelings of sadness, loss of interest in activities, and feelings of grief and/or loss. The associated suffering and embarrassment associated with HS can add to psychological susceptibility to depression. It has been observed in clinical studies that about a third of people with hidradenitis suppurativa experience clinical depression, and disease severity does not necessarily dictate suffering in the psychological sense. Large meta-analyses have demonstrated prevalence rates of depression in HS, which vary between 17% and 25% and above, with the affected individuals having almost double the odds of depression. The disparity between the findings of various studies can be attributed to the difference in the diagnostic methods, where depression measured by the depression scale has shown higher prevalence rates. Various mechanisms have been suggested to explain the relationship between the two conditions. Lack of comfort, poor quality-of-life, sexual dysfunction, restricted occupation, and social isolation are known to cause distress. Anxiety disorders are also prevalent in HS and characterized by excessive fears, excessive stress responses, and autonomic symptoms such as palpitations and sweating. Estimated values for the prevalence of anxiety based on meta-analytical data vary from 12% to 18%, and individuals with HS experience the risk twice that of those who do not have HS. While there is significant variation in the values of prevalence based on the assessment criteria, all studies have been consistent in showing high levels of anxiety. The psychosocial stressors associated with the burden of chronic diseases, presence of visible lesions, odour, and pain have been regarded as the prominent contributing causes. Moreover, the chronic inflammatory processes may also affect the neuroimmune pathways, thereby propagating the association of the presence of systemic inflammation and the disturbances in the psychological health. Bipolar disorder, involving intermittent depression and manic or hypomanic episodes, may occur more often in HS patients. There appears to be an important rise in the prevalence of bipolar disorder among individuals with HS. This is based on observations from community research. One of the potential contributing factors may be the use of lithium therapy, well-established for the management of bipolar disorder, that has been observed to induce or aggravate HS-like lesions.
Lithium affects signalling pathways inside cells, stimulates the growth of keratinocytes, increases neutrophil infiltration, and increases follicular obstruction, all of which are common with HS pathogenesis. Furthermore, shared mechanisms of inflammation related to tumour necrosis factor-alpha and interleukins may provide a potential bridge between HS and this disease. Schizophrenia refers to a chronic psychotic disorder, with symptoms involving hallucinations, delusions, and cognitive and social deficits. It has been postulated in certain epidemiological studies that the prevalence of schizophrenia has been found to be much higher in HS patients. Certain factors, including the disturbance of the immune system, inflammation, and shared environment, which could make susceptible persons vulnerable to both disorders, could be responsible. HS is closely related to a considerably increased risk of suicidal thoughts as well as suicidal behaviours. From the point of view of epidemiology, it is proven that the risk of suicide is two times as high as compared to the control group within the HS patients. Screening studies carried out among patients have demonstrated that a considerable number of them, up to one-fifth, display a risk of suicide as moderate to high. Higher risk has been noted in those with psychiatric co-morbidities, late presentation, and more severe disease needing biologic agents. By contrast, social support and family history of HS have been noted to have protective roles. Crucially, pharmaco-vigilance has noted that the use of anti-TNF agents does reduce suicidal behaviour, perhaps because of improvements in disease activity and quality of life. The use of substances is a problem in HS, and it has a strong association with pain and psychological issues. The studies show that the use of substances in HS patients has nearly twice the rate of substance use disorder compared with controls. Alcohol, opioids, and marijuana are the commonly abused substances. Alcohol use is extremely common and can be related to socioeconomic issues and self-care for emotional distress. Opioid abuse is hard to calculate accurately as these medications are commonly prescribed for pain control in individuals with HS. Marijuana use is also high, but the changing legal environment makes abuse difficult to assess. Pain is also the fundamental reason for drug abuse practices among HS students. Pain can significantly affect the functionality of a person and is a guarantor of its occurrence to seek analgesic drugs. Alcohol, opioids, and cannabis act as analgesics by suppressing different mechanisms of pain, ensuring the development of dependence. Pain management should also form part of the total management of HS because of its significance (Caccavale et al., 2023).
MISDIAGNOSIS AND OTHER PROBLEMS
In hidradenitis suppurativa, delay in diagnosis is related to ethnicity, severity of the disease, and the number of associated morbidities. Interestingly, although it is more prevalent in females, delay in diagnosis is higher in females than in male patients. HS is uncharacteristically associated with delay in diagnosis when it is a major condition compared to other inflammatory dermatoses like psoriasis. Such findings may be hampered in pediatric populations by a higher body mass index, early age of onset, widespread distribution, and genital distribution. A fear of physical contact, loss of anonymity, and discomfort during a physical exam may prevent patients from revealing their symptoms. It is often inaccurately diagnosed as "folliculitis, abscesses, or bacterial infection." Many patients see several physicians before they, or the condition, receive the proper diagnosis, which can be made by a dermatologist. The wrong ideas about the infectious nature of the disease contribute to incorrect treatment and the "stigmatization" of the patient. The relative unavailability of dermatology care leads to a point where the initial diagnosis and treatment of HS are provided at the primary care, emergency medicine, and pediatric and gynecology settings. The sensitivity and awareness of the condition on the part of the physician remain low due to a misunderstanding of the condition being a consequence of infection. While the overall number of publications on HS has increased significantly, the vast majority are contained within the dermatology literature. In addition, there are cases of internal stigma in HS, which involve feelings of embarrassment, social isolation, low self-esteem, involvement of the genital area, obesity, low socioeconomic status, and other misconceptions about HS in terms of it causing poor hygiene. This cycle of ignorance makes these people less likely to come to healthcare providers. Management for HS could include lifestyle management, pharmacologic therapy, biologic therapy, and procedural treatment depending on the disease’s severity. Flares could be managed with antibiotics, steroids, and drainage maneuvers, but the rate of recurrence is high. The treatment modalities used in maintaining the disease could include oral antibiotics, hormones, retinoids, and biologics. Adalimumab is currently the only FDA-approved biologic agent in moderate to severe HS and has had a clinical response rate noted in 40 to 60% of those treated with the drug. However, infliximab is currently used off-label and has demonstrated good results in IL- 17 trials with both secukinumab and bimekizumab. Surgical procedures such as deroofing and excision are always needed in cases of sinus tract disease as well as resistant lesions. There are evidences that support combined procedures of biotherapy with surgery. Due to its link with metabolic disorders, PCOS, inflammatory bowel disease, arthritis, psychological illnesses, and chronic pain syndrome, HS requires comprehensive medical management by multiple specializations. Assistance from nutrition counsellors, smoking cessation clinics, psychiatrists, pain management experts, surgeons, and endocrinologists would be beneficial in the management of this condition. Despite medical progress made in various treatments, inconsistent outcomes are still common due to disease heterogeneity. There is agreement on first-line treatments only. In second- and third-line strategies, treatments differ from one consensus to another. Unvalidated clinical phenotypes can be a barrier to personalized treatments. Biologic therapies are commonly begun late in the course of the disease. There is a great deal of dissatisfaction with the efficacy of the treatment, particularly with the use of antibiotics and surgical drainage. Delays in the initiation of systemic therapies and the use of biologic therapies may decrease responsiveness. Early use of biologic therapies may prevent scarring and advancement of the disease (Snyder et al., 2023).
CONCLUSION
Hidradenitis suppurativa (HS) is a persistent and recurrent condition which is not only characterized by inflammation related to follicular pathology but is also a systemic condition associated with broad impacts on various other organs and body functions. Recent available studies confirm and prove the systemic and autoimmune nature of this condition due to the involvement of TNF-alpha, IL-1 beta, IL-17, and IL-23 in immunological pathways along with follicular occlusions and genetic factors triggered by environmental factors (Del Duca et al., 2020; Preda-Naumescu et al., 2021).
The result is not only the formation of nodules, abscesses, and sinus communications within the skin but also progresses towards destructive inflammation and fibrosis with subsequent involution and loss in skin functions because of the scars. Moreover, various studies confirm associations with metabolic syndrome, cardiovascular diseases, inflammatory bowel diseases, Polycystic Ovary Syndrome, and Musculoskeletal Disorders (Sabat et al., 2020), adding to various burdens and impacts upon life expectancy associated with HS.
Advances in the molecular/immunological pathogenesis of HS have brought up a new era of treatment. Recent elucidation of mutations impairing the gamma-secretase complex and the resulting Notch signaling pathway dysfunction has clarified the pathogenesis of abnormal follicular keratinization and the immune abnormality of HS (Prens et al., 2015. Ballard et al., 2025). Additionally, the emerging pathogenetic clarifications concerning the IL-17/IL-23 pathway and the inflammasomes-dependent IL1 signaling pathway have presently underlined a main pathogenetic role of the related-Th17 driven inflammation responsible for the HS- cutaneous manifestations activity (Del Duca et al., 2020). These pathogenetic clarifications have promptly led to the development of targeted biological treatments, focused on the modulation of the above-mentioned selected inflammatory pathways, rather than on the nonspecific immunosuppression/long-lasting antibiotic treatment approaches. Although the use of standard antibiotic, retinoid, or immunosuppression therapeutic approaches is still valid for selected cases, the low long-lasting effectiveness, as well as the frequent relapses, confirm the necessity for a more focused treatment strategy (Napolitano et al., 2017).
Biologic agents can be considered the critical turning point for the treatment of HS, especially the moderate to severe form. Among all the biologic agents approved for the treatment of HS, only one is adalimumab. This particular agent demonstrated a substantial improvement in the lesions and severity of the disease along with the quality of life of the patients in large trials like the PIONEER I and II trials (Napolitano et al., 2017). Newer molecules targeted against the pathways of IL-17 have been developed in the form of secukinumab and bimekizumab. These have demonstrated a substantial efficacy profile in the early trials. However, a substantial portion of the patients have demonstrated paradoxical results or have shown poor or only partial response to the treatment (Snyder et al., 2023).
Surgery remains an integral component of the treatment of HS, especially among patients with widespread sinus tracts, recurrences of abscesses, and fibrotic changes. Methods such as deroofing, wide excision, STEEP, laser treatment, and cryo-insufflation have proven their effectiveness among selected patients, along with optimized conventional treatment (Shukla et al., 2022). Although incision and drainage may help temporarily alleviate symptoms, they do not result in the destruction of the pathological tissues, thereby resulting in a significant rate of recurrence. compared to other treatment techniques, tissue-sparing techniques, as well as laser treatment, not only promote faster healing, reduce the rate of recurrence, but also ensure improved aesthetics. Further clinical studies point towards the effectiveness of a combined treatment strategy of HS, including the use of biological therapy alongside surgical treatment, to control post-surgery inflammation as well as recurrence of the disease.
It is also crucial to note the psychosocial impact of HS, especially in light of existing high prevalence rates of depression, anxiety, substance use, and suicidal thoughts, underlining the imperative of psychological interventions in the comprehensive treatment of the disease (Caccavale et al., 2023). Additionally, the presence of chronic pain, the lack of interpersonal connections, decreased work performance, and associated stigma all stand to negatively impair the health of patients, apart from central and peripheral impacts of systemic inflammation on the central nervous system, thereby increasing the severity of associated psychological comorbidities. Comprehensive interventions of health, lifestyle, counselling, and educational initiatives, in addition to psychiatric help and the control of associated comorbidities such as chronic pain, shall present significant alleviations in the current challenges associated with HS. Thus, the reality of hidradenitis suppurativa and its association with an inflammatory state, along with a host of associated challenges, warrants the imperative of early diagnosis, comprehensive biological interventions, and comprehensive health initiatives.
REFERENCES


Krishna Prasath S K, Harshini Raja, Hidradenitis Suppurativa: From Physiopathologies to Targeted Therapeutics, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 3107-3122. https://doi.org/10.5281/zenodo.18390098
 10.5281/zenodo.18390098
10.5281/zenodo.18390098
