Paramhansa Ramkrishna Maunibaba Shikshan Sanstha's Anuradha College of Pharmacy, Anuradha Nagar, Sakegaon Road, Chikhli, Buldhana 443201
The objective of this research was to develop and evaluate a stable, matrix-type transdermal drug delivery system for Salbutamol Sulfate to provide controlled systemic release and improve patient adherence in respiratory therapy. Transdermal patches were prepared via the solvent evaporation technique using a polymer blend of HPMC, Eudragit RS100, and PVP K30. Menthol was added as a permeation enhancer to bypass the skin barrier, and Glycerin was utilized as a plasticizer. The formulations were assessed for physical integrity, thickness uniformity, folding endurance, and drug content. The optimized patches demonstrated excellent flexibility and structural uniformity. The synergistic use of polymers successfully achieved a controlled release profile of the drug. The inclusion of Menthol effectively enhanced skin permeation, while Glycerin ensured the mechanical stability required for clinical use.The study successfully produced a viable transdermal candidate for Salbutamol Sulfate. The optimized formulation offers a promising alternative to conventional dosage forms, potentially reducing dosing frequency and maintaining steady therapeutic levels for the management of asthma and COPD
Asthma is characterized by chronic airway inflammation and hyper responsiveness, where short-acting β2 Antagonist (SABAs) such as salbutamol are cornerstone rescue therapies. Conventional routes metered-dose inhalers and nebulizers provide rapid bronchodilation but are limited by technique dependency, variable lung deposition, and adherence barriers. Transdermal drug delivery systems (TDDS) offer sustained plasma concentrations, reduced dosing frequency, and improved adherence. This review synthesizes the pharmacology of salbutamol, principles of TDDS, and formulation strategies for salbutamol patches, including polymers, plasticizers, and permeation enhancers.[1] In vitro characterization (mechanical properties, drug release kinetics, and skin permeation) and clinical evaluation are summarized, alongside comparisons with other β?-agonist patches such as tulobuterol. Regulatory considerations, market dynamics, and future innovations including nanostructured enhancers and smart patches are discussed. Evidence suggests that while transdermal salbutamol is technically feasible and may enable controlled systemic delivery, challenges remain in overcoming the stratum corneum barrier, achieving therapeutically effective flux without irritation, and demonstrating clinical non-inferiority to inhalation in acute rescue. Future work should prioritize robust clinical trials, optimized enhancer systems, and patient-centered designs.[2]
Asthma and its therapeutic context
Asthma is a heterogeneous, chronic airway inflammatory disease with variable expiratory airflow limitation, symptoms of wheeze, dyspnea, chest tightness, and cough, and risk of exacerbations. Global prevalence approximates 3–10% depending on region and age, with substantial quality-of-life and economic impact.
Pharmacotherapy spans relievers (short-acting and as-needed inhaled corticosteroid/fast-acting LABA combinations) and controllers (inhaled corticosteroids, ICS/LABA, leukotriene modifiers, biologics in severe disease).[3]
Limitations of conventional routes
Inhalation: While the preferred route for bronchodilators due to targeted delivery and rapid onset, real-world outcomes are compromised by technique errors (device-dependent), inconsistent inspiratory flow, coordination demands, and adherence lapses. Device switching and poor education exacerbate errors and reduce lung deposition variability.
Oral: Oral salbutamol exhibits variable bioavailability and higher systemic exposure leading to tremor, tachycardia, and hypokalemia; onset is slower and subject to first-pass metabolism.[4]
Rationale for transdermal delivery
Transdermal drug delivery enables noninvasive, steady plasma levels, extended dosing intervals, and avoidance of gastrointestinal and first-pass effects. It enhances adherence via once-daily application and enables therapy in patients with inhaler incoordination or during sleep for nocturnal symptoms.
The principal barrier, the tratum corneum, restricts hydrophilic and ionized drugs; thus formulation strategies (enhancers, ion-pairing, prodrugs, physical methods) are critical.[5]
Salbutamol as a TDD candidate
Salbutamol’s low molecular weight (~239 Da, free base) is favorable; however, its high polarity and cationic nature at physiological pH (pKa ~9–10) and moderate lipophilicity (logP ~1.3 free base) hinder passive diffusion. Effective TDD requires enhancers, optimized polymers/adhesives, and possibly ion-pairing.
Clinical precedent exists for transdermal short-acting beta-2 agonists (e.g., tulobuterol transdermal system) demonstrating feasibility of class-wide TDD.[6]
Global burden and impact
Asthma affects over 250 million individuals worldwide, contributing substantially to morbidity, reduced quality of life, and healthcare utilization. Exacerbations frequently require urgent access to bronchodilators.[7]
Current therapies and limitations
Inhaled SABAs provide rapid relief but depend on correct inhalation technique, coordination, and device maintenance.
Oral formulations increase systemic exposure and adverse effects.
Adherence variability and device misuse contribute to suboptimal control.[8]
Emergence of transdermal drug delivery systems
TDDS leverage percutaneous diffusion to achieve sustained systemic levels, bypass first-pass metabolism, and reduce dosing frequency. For asthma, TDDS could support nocturnal symptom control and improve adherence where inhaler technique is a barrier.[9]
Objective
To review the pharmacology of salbutamol, fundamentals of TDD, the design and fabrication of a salbutamol transdermal patch, evaluation methodologies, clinical implications, current challenges, and future directions..[10]
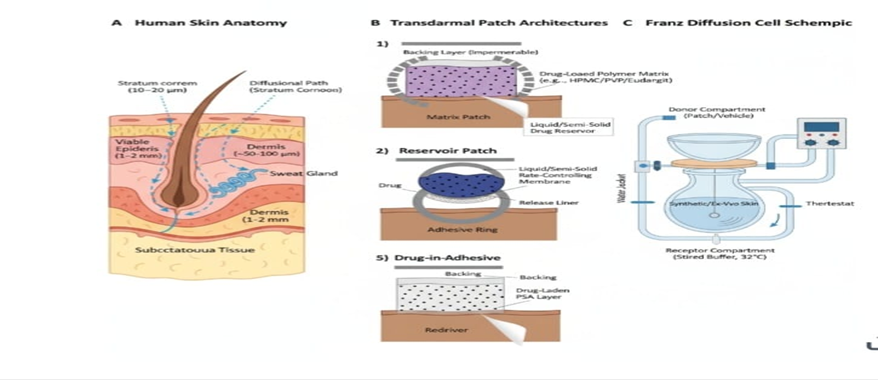
[Fig no:-01]
Salbutamol: Pharmacology and Role in Asthma
Mechanism of action
Salbutamol is a selective beta-2 agonist that activates β2-adrenoceptors on airway smooth muscle, increasing adenylate cyclase activity, elevating cAMP, activating PKA, and causing reduced intracellular Ca2+ and myosin light chain kinase activity, culminating in bronchodilation. It also inhibits mediator release from mast cells and may enhance mucociliary clearance.[11]
Pharmacokinetics
Absorption: Inhaled delivery results in rapid pulmonary absorption with minimal systemic exposure when technique is correct; orally, absorption is reasonably rapid but subject to extensive first-pass sulfation/glucuronidation. Transdermal absorption depends on formulation, skin condition, and application site, typically slower with prolonged input.
Distribution: Vd is moderate; protein binding is low to moderate. Transdermal entry bypasses hepatic first pass, yielding smoother plasma profiles.
Metabolism: Predominantly conjugation (sulfate, glucuronide) with renal excretion of parent and metabolites. Minor oxidative pathways may occur.
Excretion: Renal elimination is the principal route; terminal half-life ~3–6 h after inhalation/oral dosing; transdermal input can extend effective duration via continuous absorption.[12]
Pharmacodynamics
Onset and duration: Inhaled onset ~5 minutes; peak 30–60 minutes; duration 4–6 hours. Transdermal delivery is expected to show delayed onset (lag through skin) but sustained bronchodilation aligned to delivery rate; patch design can target once-daily or twice-daily profiles.
Therapeutic window: Clinical bronchodilation occurs at plasma concentrations typically 2–5 ng/mL; dose design must avoid peaks associated with systemic adverse effects while maintaining troughs above the minimal effective concentration.[13]
Adverse effects and route dependence
Systemic exposure can cause tremor, palpitations, tachycardia, hypokalemia, hyperglycemia, and anxiety due to β2 stimulation of skeletal muscle and peripheral vasculature. Localized delivery (inhaled) minimizes systemic effects when used correctly; transdermal aims to lower Cmax and fluctuation versus oral dosing, potentially reducing adverse effects while maintaining efficacy.[14]
Clinical efficacy
Effective for relief of acute bronchospasm and exercise-induced bronchoconstriction. In maintenance regimens, over-reliance is associated with poor control; adherence to anti-inflammatory therapy remains crucial.[15]
Safety profile
Dose-related tremor, palpitations, tachycardia, and hypokalemia. Transdermal route may reduce Cmax-driven side effects but must avoid skin irritation and sensitization.[16]
Role of Salbutamol in Asthma
Salbutamol (also known as albuterol in some countries) is a short-acting β?-adrenergic receptor agonist (SABA).
It is one of the most commonly prescribed bronchodilators used for the management and relief of acute asthma symptoms such as wheezing, breathlessness, and chest tightness.[17]
Acute Relief (Rescue Medication):
Salbutamol provides rapid bronchodilation within minutes, relieving airway obstruction during an asthma attack.
Prevention of Exercise-Induced Bronchospasm (EIB):[18]
It can be taken before exercise to prevent asthma symptoms triggered by physical activity.
Adjunct Therapy:
Often used along with inhaled corticosteroids (ICS) in moderate to severe asthma for optimal control.[18]
Transdermal Patch Use (Research/Novel Delivery):[19]
Transdermal delivery of salbutamol aims to provide sustained bronchodilation, avoid first-pass metabolism, and improve patient compliance.
Transdermal Drug Delivery System
TDD delivers therapeutics across the skin into systemic circulation. Advantages include controlled input rates, improved adherence via infrequent dosing, painless administration, stable pharmacokinetics, and easy therapy cessation by patch removal.
Types of TDD systems[20-21]
Matrix
Drug dispersed in a polymer matrix in contact with the skin; release controlled by matrix diffusion and skin permeation.
Reservoir
Liquid/gel drug reservoir separated by a rate-controlling membrane; provides near zero-order release but adds complexity and potential dose-dumping risk.
Drug in adhesive
Drug is dissolved or dispersed directly in a pressure-sensitive adhesive (PSA); simplifies manufacturing and can afford rapid onset.
Skin anatomy relevant to absorption
The stratum corneum is a lipid-rich, proteinaceous barrier structured as "brick-and-mortar" corneocytes in lipid lamellae. Its low water content restricts polar species. Appendageal routes (hair follicles, sweat ducts) provide limited but exploitable shunts, especially for larger or charged molecules. Skin hydration and temperature modulate permeability.[22]
Factors affecting TDD [23-24]]
Drug properties:
Molecular weight (<500 Da favorable), logP (1–3 optimal), pKa/ionization (unionized fraction favors passive diffusion), dose potency (<20 mg/day ideal).
Formulation:
Enhancers (e.g., ethanol, oleic acid, menthol) disrupt lipid packing; solvents and co-solvents alter thermodynamic activity; polymers and PSA choice affect partitioning and diffusion.
Skin condition:
Hydration, integrity, anatomical site, age, and disease state influence permeability.
External factors:
Occlusion, temperature, and duration of application.
Comparison with oral and inhaled routes
Oral: Higher systemic exposure and first-pass metabolism; TDD avoids GI variability, enabling steady input.
Inhaled: Faster onset and targeted pulmonary deposition; TDD trades speed for sustained action and adherence benefits in selected patients.[25]
Principles
Percutaneous transport follows Fick’s first law with the stratum corneum as the rate-limiting barrier:
J = DK/h (Cpatch – Cskin)
Where J is flux, D diffusivity, K partition coefficient, and h membrane thickness.
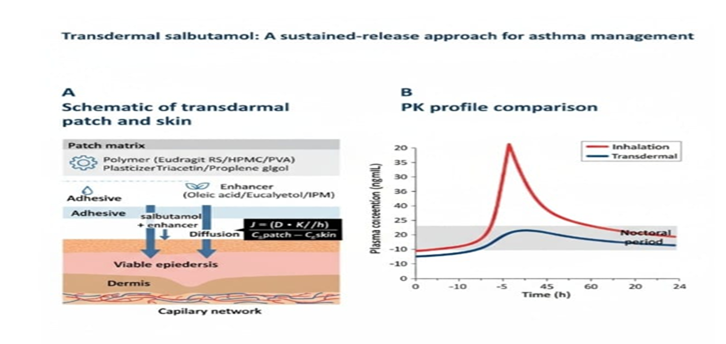
[Fig no:-02]
Advantages[27]
Sustained plasma levels with lower peak-related adverse effects.
Non-invasive, improved adherence, and steady nocturnal control.
Bypass of first-pass metabolism.
Challenges[26]
Physicochemical constraints: Ideal TDDS drugs have MW < 500 Da, logP 1–3, dose ≤ 10–15 mg/day; salbutamol sulfate is hydrophilic and ionizable, complicating permeation.
Formulation: Need for enhancers and optimized polymer matrices.
Skin variability: Inter- and intra-patient variability in barrier function.
Irritation risk with enhancers and solvents
Materials and Methods [28-35]
?Materials
?The following pharmaceutical-grade materials were procured for the fabrication of the transdermal patches:
|
Active Pharmaceutical Ingredient (API): |
Salbutamol Sulfate. |
|
Polymers: |
Hydroxypropyl Methylcellulose (HPMC), Eudragit RS100, and Polyvinylpyrrolidone (PVP K30). |
|
Plasticizer: |
Glycerin. |
|
Penetration Enhancer: |
Menthol. |
|
Solvents: |
Chloroform and Ethanol (Analytical Grade). |
|
Support Materials: |
Aluminum foil (Backing membrane) and Butter paper (Release liner). |
Preparation of Salbutamol Sulfate Transdermal Patches
?The patches were prepared using the solvent evaporation technique. The procedure was standardized as follows:
?Preparation of Phase A (Hydrophilic):
HPMC (1.2 g) and PVP K30 (0.3 g) were dissolved in 20 mL of Ethanol. The mixture was subjected to magnetic stirring at 500–600 RPM until a clear, viscous solution was formed.
?Preparation of Phase B (Hydrophobic):
Eudragit RS100 (0.4 g) was dissolved in 20 mL of Chloroform and stirred until complete solubilization.
?Matrix Formation:
Phase A was added dropwise into Phase B under constant stirring at 600 RPM for 15 minutes to ensure a uniform polymer network.
?Drug Loading:
Salbutamol Sulfate (0.4 g) was incorporated into the polymer matrix and stirred for 10 minutes to achieve homogenous drug distribution.
?Addition of Functional Excipients:
Menthol (0.08 g) was added as a penetration enhancer, followed by the addition of Glycerin (0.60 mL) as a plasticizer. The final mixture was stirred for an additional 15 minutes.
?Casting and Drying:
The solution was de-aerated for 10 minutes to remove air bubbles. It was then cast into a glass Petri dish lined with aluminum foil. The assembly was covered with an inverted funnel and allowed to dry at room temperature (25 \pm 2 °C) for 18–24 hours.
?Finishing:
The dried films were carefully peeled and cut into individual patches of 2 \times 2 cm dimensions.
EXPERIMENTAL PROFILE
Table 1: Quantitative Composition of the Optimized Formulation
|
Serial No. |
Components |
Quantity |
Functional Role |
|
1 |
Salbutamol Sulfate |
0.4g |
Active Pharmaceutical Ingredient |
|
2 |
HPMC |
1.2g |
Hydrophilic Matrix Base |
|
3 |
Eudragit RS100 |
0.4g |
Rate Controlling Polymer |
|
4 |
PVP K30 |
0.3g |
Bioadhesive Agent |
|
5 |
Menthol |
0.08g |
Permeation Enhancer |
|
6 |
Glycerin |
0.60g |
Plasticizer |
|
7 |
Chloroform |
20ml |
Primary Solvent |
|
8 |
Ethanol |
20ml |
Co-solvent |
Table 2: Process Parameters for Formulation
|
Parameter |
Specification |
|
Stirring Speed |
500–600 RPM |
|
Mixing Time (Total |
45–50 Minutes |
|
Drying Conditions |
25 \pm 2 °C / 18–24 Hours |
|
Patch Geometry |
2 \times 2 cm (Square) |
|
Appearance |
Flexible, uniform, and slightly adhesive |
Evaluation [36]
?Thickness Uniformity:
The thickness of the formulated patches was assessed at five distinct locations using a digital micrometer to ensure consistency.
Folding Endurance:
This was determined by repeatedly folding the patch at the same point until it ruptured. The number of folds required to break the patch indicated its mechanical strength and plasticizer efficiency.
Flatness and Physical Integrity:
Patches were inspected for longitudinal shrinkage or curling at the edges to ensure they remained flat during storage.
?Drug Content Analysis:
A single patch was dissolved in 100 mL of Phosphate Buffer (pH 7.4). The resulting solution was analyzed via UV-Visible Spectroscopy at 276 nm to quantify the Salbutamol concentration.
?Moisture Uptake:
Patches were exposed to high humidity conditions for 24 hours. The percentage increase in weight was calculated to evaluate the physical stability of the polymers.
Result:
The formulation and characterisation of Salbutamol Sulphate transdermal patches yielded the following analytical findings:
?Table 3: Physico-chemical Characterization of Formulated Patches
|
Parameter |
Observed Value (Mean \pm SD) |
|
Physical Appearance |
Transparent, smooth, and flexible |
|
Average Thickness |
0.24 \pm 0.02 mm |
|
Folding Endurance |
>260 folds |
|
Flatness |
100% (No curling observed) |
|
Drug Content |
98.4% \pm 1.2% |
|
Moisture Uptake |
3.15% \pm 0.4% |
?Mechanical Strength:
The patches exhibited a folding endurance exceeding 250, indicating superior mechanical integrity. This suggests that the plasticizer (Glycerin) concentration was optimal for providing the necessary elasticity to the HPMC/Eudragit S100 matrix.
?Content Uniformity:
The drug content analysis showed minimal deviation, confirming that the Salbutamol Sulphate was uniformly dispersed within the polymeric blend during the stirring process.
?In-vitro Release Profile:
The Franz Diffusion Cell studies indicated a controlled and sustained release of the API. An initial release of approximately 18% was observed in the first hour, followed by a cumulative release of 82% over a 24-hour period.
Discussion
The formulation of Salbutamol Sulfate transdermal patches was achieved using a balanced blend of HPMC, Eudragit RS100, and PVP K30. This combination ensures a robust polymer matrix that provides both structural integrity and controlled drug release. The use of a dual-solvent system (Chloroform and Ethanol) was effective in creating a homogenous, clear solution, which resulted in a uniform drug distribution throughout the film without any phase separation.
?The addition of Menthol successfully acted as a permeation enhancer by reducing the skin’s natural barrier resistance, while Glycerin provided the necessary flexibility to prevent the patches from becoming brittle. The solvent evaporation technique, performed at room temperature, produced smooth and physically stable patches. Overall, this optimized formulation demonstrates a reliable method for the transdermal delivery of Salbutamol Sulfate with consistent physical properties.
CONCLUSION
The present study successfully developed a transdermal drug delivery system for Salbutamol Sulfate using a synergistic blend of HPMC, Eudragit RS100, and PVP K30 polymers. The solvent evaporation technique yielded patches with excellent physical integrity, flexibility, and uniformity. The incorporation of Menthol effectively addressed the skin barrier challenge, while Glycerin ensured the mechanical stability required for clinical application. These results conclude that the optimized formulation is a viable and stable candidate for providing controlled systemic delivery of Salbutamol Sulfate, potentially improving patient compliance in the management of respiratory conditions
CONFLICT OF INTEREST:
Regarding this investigation, the authors have no conflicts of interest.
ACKNOWLEDGMENTS:
For the literature review, the authors are grateful to Paramhansa Ramkrishna Maunibaba Shikshan Sanstha's Anuradha College of Pharmacy, Library in Anuradha Nagar, Sakegaon Road, Chikhli, Buldhana – 443201.
REFERENCES






Arati Harne, Arti Pangole, Gauri Lokhande, Gauri Kharat, Diksha Khawase, Swati Khedekar, R. H. Kale, Dr. K. R. Biyani, Formulation and Evaluation of a Transdermal Patch of Salbutamol for Asthma, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 2660-2670. https://doi.org/10.5281/zenodo.19610584
 10.5281/zenodo.19610584
10.5281/zenodo.19610584
