Sudhakarrao Naik Institute of Pharmacy, Pusad Maharashtra, India 445204
Drugs with a limited shelf life of absorption within the digestive system (GIT) have poor bioavailability when given in traditional dose forms due to their brief duration of stay at the absorption location and partial drug release. In-situ gel is the most effective way to address problems with immediate-release dose forms and those with brief gastrointestinal residence durations. Prior to administration, the in-situ gel dosage form is a liquid, but it changes into a floatable gel. The stomach contents when it comes into contact with them. In-situ gel formation can be triggered by a single stimulus or by a mix of various stimuli, including ionic crosslinking, temperature changes, and pH variations. This leads to greater residency as well as a prolonged discharge. Developing drug delivery methods in-situ May have the following advantages: a straightforward manufacturing procedure, comfort, reduced occurrence of administration, convenience of use and enhanced adherence by patients. It is easy to apply to the location where drugs are absorbed, where they expand to form a solid gel that can prolong the residence duration of the active ingredient. Oral, ophthalmic, rectal, vaginal, injectable, and intraperitoneal methods are used to administer in-situ gels methods.
Given how simple it is to administer, the oral route is seen to be the best option. Since many traditional oral medication administration methods have some drawbacks related to stomach emptying time, gastric retention has drawn interest in the latter years by remaining in the stomach region for a few hours, a The GRDDS, or gastro retentive drug delivery system, can prolong the duration of a medication's gastric occupancy. Prolonged stomach retention improves solubility, enhances bioavailability, and minimises medication waste for medications that are less soluble at high pH levels settings. A systems that float, bio adhesive, high-density, swell, and expand etc., are some of the methods used to accomplish gastric retention. Has been created. [1] The floating drug delivery system (FDDS) works well for prolonging the stomach residence duration and improve the bioavailability of the medications. In 1968, Davis gave the first description of FDDS. Low-density devices known as FDDS are buoyant enough to float over the contents of the stomach and stay there for an extended amount of time. Mechanisms for floating medicine delivery were intended. They float atop the stomach's contents for gastric retention due to their low density, and by exhibiting a regulated release, they produce a long-lasting action. Pharmaceuticals that are absorbed from the upper portion of the stomach benefit greatly from this kind of delivery method. It is also beneficial for pharmaceuticals that are administered at an alkaline pH of the stomach and are either not absorbed or have negative side effects due to their insoluble nature. For medications that must possess a stomach local action, the FDDS are very helpful. [2] Gastro-retentive floating systems are used to manufacture a wide range of dosage forms, like tablets, capsules, films, microspheres, microbeads, and more. One recent development in floating DDS is the in-situ gelling technique. A variety of delivery routes, including oral, nasal, ocular, peroral, rectal, vaginal, and parenteral, can be used with an in-situ gelling system. [2] In recent years, in situ gelling methods have attracted good attention. The use of in situ gel-forming devices in a range of medical applications, such as medication delivery, has been the subject of many published patents in recent years. The rising interest in these delivery systems may be due to the several Benefits of in situ forming polymers include increased patient compliance, comfort, decreased frequency of administration, and case of administration. [3] One the "in-situ gel" technology is one of the most cutting-edge drug delivery techniques. The "sol to gel" transition's special properties mean that the in-situ gelling helps to enhance patient compliance, comfort, and the regulated and prolonged release of the drug. A formulation known as an in-situ gelling system is one that is a solution before it enters the body, but under one or more of many physiological circumstances, it transforms into a gel. Numerous factors, including pH, temperature variations, solvent exchange, ionic cross-linking, etc., affect the the transition from sol to gel. The "system for in-situ gelling" system" offers several benefits, such as simpler dosage delivery and fewer doses [1] other names for oral in situ gel forming systems include stomach-specific or raft forming systems. Improved gastro-retention and controlled drug distribution in the stomach. Despite being more stable than liquids, floating dose forms like tablets and capsules have the drawback of having to be swallowed whole. These are likewise designed for controlled release, and because the size of the tablet affects its capacity to float, they cannot be split in two if the dosage is changed. It becomes challenging for older patients, youngsters, and patients with certain diseases (such as dysphasia) to swallow tablet or capsule dose forms. [4] Verbal Drug distribution that is regulated and maintained can be achieved with in situ gel-forming technologies. An appropriate technique of regulated medication administration within the stomach is provided by the conversion of an environment-specific gel-forming solution into gel, which, because of its lower density than the gastric acid, floats on the surface of the stomach fluids contents. Using a low-viscosity solution, this technique that changes its polymeric structure when the stomach contents and a viscous gel with a density less than the stomach contents come into touch. This gel formation with a low density not only creates a continuous and progressive release of the medicine but also provides the required gastro retention and extends the contact duration. The gel's capacity to float can also be improved by adding substances that produce effervescence, like carbonates or bicarbonates, both with and without tartaric or citric acid The gel will become significantly lighter due to the carbon dioxide release, which will aid in its ability to float. By adding viscosity enhancers, such as HPMC (Hydroxy propyl methyl cellulose), the gel's ability to generate a more controlled and extended release can also be improved. [5] Drug delivery techniques that are in sol form prior to body administration but gel in-situ to form a gel after injection are known as floating in-situ forming polymeric formulations. The variables that affect the gels from which the drug is extracted include temperature control, pH variations, the presence of ions and UV light, electrical sensitivity, and enzyme sensitivity. Released under control and gradually. Due to a great deal of research being done to improve the performance, dependability, and safety of pharmaceutical goods, regulated and extended drug administration has recently become more common in modern pharmaceutical design. The In-situ gel-forming
Polymeric formulations have numerous benefits over traditional drug immunisation methods, such as strong patient compliance and prolonged and prolonged action and excellent biocompatibility and durability qualities, which make in situ gel dosage forms very reliable. The biodegradable polymers used to create in situ gels include gellan gum, sodium alginate, HPMC (hydroxypropyl methylcellulose), xyloglucan, pectin, chitosan, poly (DI, lactic acid), poly (DI-lactide-co-glycolide), and poly caprolactone. [6]
GASTRORETENTIVE DRUG DELIVERY SYSTEM BENEFITS (GRDDS)
The GRDDS approach could be applied to analyze a wide range of drugs or pharmacological classes. Among the primary advantages are:
FACTORS AFFECTING GASTRIC RETENTION
Numerous factors influence the gastrointestinal residence time, which in turn influences the gastroretentive system's bioavailability and effectiveness.
THE SIGNIFICANCE OF THE IN SITU GELLING SYSTEM
ADVANTAGES OF IN SITU GELS
DISADVANTAGES OF IN SITU GELS
It can be challenging to create a stable in situ gel formulation that gels in the ideal setting, at the ideal moment, and in the ideal circumstances.
PRINCIPLE OF IN-SITU GEL FORMATION
A gelling agent that may create a stable sol with other excipients and the medication being administered are utilised in the creation of the gastroretentive in situ gel system. Ionic complexation brought on by a pH shift is what causes this sol system to gel in a stomach environment. The formulation used is a sodium alginate solution that contains sodium citrate and calcium carbonate (as a source of Ca2+); it complexes the free Ca2+ ions and releases them only into the stomach's acidic environment. Sodium alginate is the gelling agent. Sodium alginate polymeric chains cross-link to form a macrostructure when free Ca2+ ions are trapped within them. This gelation process produces double helical junction zones, after which the double helical segments reaggregate to form a three-dimensional network through hydrogen bonding with water and complexation with cations. [9]
Sodium citrate + Ca-Carbonate (Ca2+)→ Ca-Citrate complex--------------> Ca²+COO
Until the formulation reaches the stomach, where sodium alginate gels instantly, it stays in liquid form. Together with the cross-linking agent, the gelling agent acts as a dispersion medium in the form of an aqueous solution to hold the medication in a dispersed state. [10
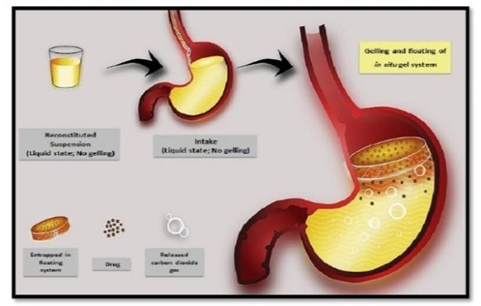
Figure 1: Floating in situ gelling system [11]
FLOATING DRUG DELIVERY SYSTEM CLASSIFICATION
The buoyancy principle has led to the development of floating drug delivery systems using two completely distinct methods.
1. Effervescent systems
The matrices used in these buoyant delivery methods include polysaccharides like chitosan, swellable polymers like Methocel, effervescent chemicals like sodium bicarbonate and citric or tartaric acid, and liquid chambers that gasify at body temperature. Either organic solvents (such as ether or cyclopentane) or carbon dioxide generated by an effervescent reaction between organic acids and carbonate-bicarbonate salts can volatilise and release gas into the floating chamber. Since the stomach's contents are acidic, the matrices are designed to ensure that carbon dioxide is released and retained in the gellified hydroonilloid when it reaches the stomach. The dosage form rises and keeps its buoyancy as a result. Recently, a floating tablet that contains multiple carbon dioxide gas-emitting components was created.
2. Non-effervescent systems
Gel-forming or highly swellable polysaccharides or matrix-forming polymers such as polyacrylate, polycarbonate, polystyrene, and polymethacrylate are typically used to create non-effervescent floating drug delivery systems. In the stomach environment, it retains its relative shape and bulk density below unity. The medicine can come into contact with the stomach fluid after oral administration when it is intimately mixed with a gel-forming hydrocolloid. These dosage forms are buoyant because the expanded polymer traps air. Polyacrylates, calcium chloride, sodium alginate, carbopol, polyethylene oxide, and polycarbonates, polyvinyl acetate, and hydroxyl propyl methylcellulose (HPMC) are the excipients most frequently used in these systems. [2]
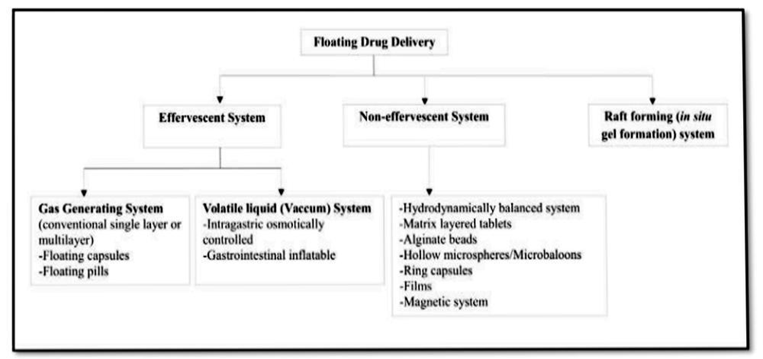
Figure 2: Classification of floating drug delivery systems [1]
THE STOMACH-SPECIFIC FIOTATION IN SITU GEL AND ITS APPLICATIONS
1. Enhanced absorption
For medications that are primarily absorbed from the upper part of the stomach, a longer contact time at the site of maximum absorption increases the degree of absorption.
2. Enhancement of bioavailability
Improved bioavailability is the outcome of increased medicine absorption in the stomach. As the stomach transit time increases, so does the medication's bioavailability.
3. Less negative medication effects
As the medication stays in the stomach until it is fully released, the frequency of the negative effect on the colon reduces.
4. Site-specific medication administration
The absorption rate of drugs that are absorbed from the stomach increases because they have enough residence time for absorption. Additionally, the medication's local action in the stomach is maintained, necessitating a reduced dosage. [1]
SUITABLE CHARACTERISTICS OF POLYMERS
Any gel's manufacturing requires the use of a polymer. The following are some essential polymer properties for in situ gels:
CLASSIFICATION OF IN SITU GEL POLYMERS
The origin or gelation method is used to classify polymers. According to an in situ source, gelling systems fall into two categories:
APPROACHES TO PRODUCE IN SITU GEL
The following are some of the different techniques and procedures used to create the in-situ gel formation:
Gel Creation through Physical Modifications
This technique uses either the swelling or diffusion phenomena. The polymer in the system swells and produces a viscous gel, such as glycerol mono-oleate, as it absorbs water from the environment. is used to dissolve or distribute the medication and the polymer seeps into the surrounding tissues, the polymer (such as N-methyl pyrrolidone) precipitates and gels.
Based on Stimuli or Chemical Changes, In Situ Gel Formation
Changes to the chemical environment of the system that produce polymeric cross-linking might lead to gel formation:
Ionic cross connecting
Some examples of ion-sensitive polysaccharides are sodium alginate, pectin, carrageenan, and Gellan gum (Gelrite®). that experience phase transitions when exposed to different ions like K+, Ca+2, Mg+2, and Na+. For example, divalent cations, particularly Ca2+, can cause the low methoxypectins to gel. When divalent or polyvalent cations, such as Ca2+, are present, alginic acid gels because of its interaction in alginate chai with the guluronic acid block.
Catalysed cross-linking
It is believed to be the most feasible way to produce gels when a network of polymers is created by cross-linking caused by enzymes present in body fluids.
Photo polymerization
When tissues containing such a gel forming system are exposed to microwave, ultraviolet, or electromagnetic radiation, gels such as 2, 2 dimethoxy-2-phenyl acetophenone, ethyl eosin, etc., form inside the tissues.
Physiological Stimuli-Induced Gel Formation in Situ:
Changes in the system's pH and temperature are two physiological triggers that might cause gel formation.
pH-Dependent Gelling
A different method of in-situ gel production relies on pH changes. When the pH changes, several polymers, like Polyvinylacetal diethylaminoacetate (AEA), PAA (Carbopol, carbomer) or its derivatives, and blends of poly (ethylene glycol) (PEG) and poly (methacrylic acid) (PMA), shift from sol to gel. As the external pH rises, the hydrogel's swelling decreases when weakly basic (cationic) groups are present, and increases when weakly acidic (anionic) groups are present.
Temperature-Dependent in Situ Gelling
At room temperature (between 200 and 250 degrees Celsius), these hydro gels are liquid; however, when they come into contact with body fluids (between 350 and 370 degrees Celsius), the temperature rise causes them to gel. This technique exploits the temperature-induced phase change. An abrupt change in temperature causes a polymer to become soluble in the system, and interactions between polymers produce a hydrophobic solvated macromolecule. The most researched family of polymers for creating in-situ gel properties are temperature-sensitive polymers, such as polyacrylic acid and polyacrylamide. [5]
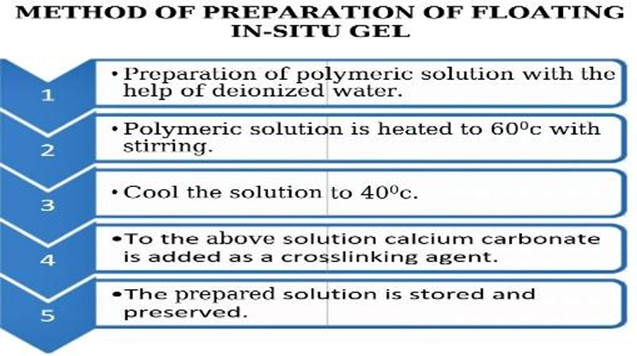
Figure 3: Technique for Floating in Sit Gel Preparation [13]
MECHANISM OF FLOATING IN-SITU GEL
As the drug floats on the stomach, it is progressively released from the sestem at the proper rate. The stomach empties the residual system after the drug is released. In addition to the small quantity of stomach content needed to allow the proper A small amount of floating force (F) is also required to keep the dosage form continuously buoyant on the surface of the meal in order to realise the buoyancy retention principle. In order to measure the kinetics of the floating force, a novel method for computing the resulting weight has been published in the literature. The apparatus measures the force equal to F continuously (in relation to time) required to submerge the primary object. The item floats more readily if F is on the upper positive side. (Figure 2). This device helps to improve FDDS in terms of stability and endurance of floating forces generated, thereby avoiding the drawbacks of unpredictable intragastric buoyancy capability fluctuations.
F = F buoyancy – F gravity
= (Df – Ds) gv
where v is the volume, g is the acceleration caused by gravity, Df is the fluid density, Ds is the object density, and F is the total vertical force. [14]
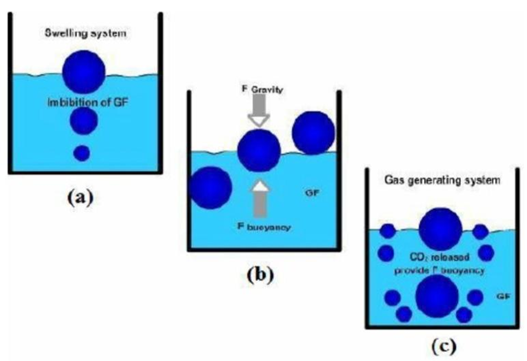
Figure 4: The floating system's mechanism, where GF stands for gastric fluid [1]
EVALUATION PARAMETERS:
Fourier Transform Infrared (FTIR) Studies Of Compatibility
Fourier transform infrared spectroscopy (FTIR) was employed to conduct medication and polymer compatibility tests. Using the KBr design and an FTIR (M/s Shimadzu, Model: IR Spirit) technique, the materials' Fourier transform infrared spectra were acquired in the 4000–450 cm range. [16]
Standard Calibration Curve
A 100 mg dose of the drug 0.1N HCl was added to a 100 ml volumetric flask. was dissolved, and the required volume was created, creating stock 1. A volumetric flask was filled with 0.1N HCL to reach 100 ml after 10 ml of the stock solution was pipetted out and moved there. Using a pipette, remove the solution until the concentration reaches 5, 10, 15, 20, and 25 µg/ml. The absorbance was measured using the UV Spectrophotometer. [17]
Melting Point Determination
A capillary tube's sealed end was filled with a small amount of the powdered material, which was subsequently compacted by lightly tapping it on a hard surface. A tiny rubber band was used to tie the capillary tube to a thermometer, making sure the sample was placed close to the heating element's center. A pace of around 2 to 5°C per minute was used to progressively heat the melting point equipment. Using a magnifying glass, the sample was examined. Nepafenac started to melt as the heating process went on, and the solid eventually became a liquid. The. The temperature at which this transition began was identified as the melting point. [18]
Physical Appearance
The solution's clarity is one of the most important preparatory factors. The solution's clarity was evaluated using a visual component set against a black and white backdrop. [23]
PH
pH is one of the formulation's most important components. The pH of the mixture should be adjusted to stay constant at that level while also preventing patient discomfort when administered. The pH was tested using a calibrated digital pH meter. in each solution at 25°C. [19]
Ideal PH Range:
Formulation (before administration): (PH ~ 4.0-7.0)
Gelation occurs in the stomach (PH ~1.2-2.5)
Drug Content
A magnetic stirrer was used to stir the mixture for an hour after 10 millilitres of in-situ gel had been measured and transferred to 100 millilitres of the volumetric flask containing 0.1N HCI. Following filtering, 0.1N HCl (pH 1.2 medium) was added to the solution to dilute it appropriately. [20] A UV-visible spectrophotometer set to 276 nm was used to measure the concentration of the medication in the filtered solution after it had been appropriately diluted with gastric simulated fluid and contrasted with a suitable blank solution. [21]
Viscosity
Field of Brook A viscometer was used to measure the viscosities of the generated formulations. 50 milliliters of the sample were measured, transferred into Nessler's cylinder, and sheared using spindle 63 at room temperature at speeds of 50 and 60 rpm. The viscosity of each sample was measured three times. [22]
Ideal Viscosity Ranges:
Before gelation (sol state): 50-300 mpa.s
After gelation (gel state): 1,000-10,000 mpa.s
Stability Studies
In compliance with ICH criteria, the stability study for the improved formulation was conducted using the research technique designed for the worldwide market. [27] An amber-colored container with an aluminum lid for sealing was filled with the improved in situ gel composition and sealed firmly. The The formulation was subjected to a range of temperature conditions in order to conduct the stability study, including refrigerator temperature at 5 °C+3 °C, accelerated temperature at 40 °C+2 °C/75%±5% RH, and room temperature at 25 °C+2 °C/60%±5% RH. (thermo stability chamber) for one month. Periodically, samples were taken out (0, 15, and 50 days) and assessed for pH, drug concentration, visual appearance, and floating behavior. [23]
In-vitro Gelling Capacity
remains To evaluate the formulations for their in-vitro gelling ability, a visual technique was used to create solutions of in-situ gel forming drug delivery systems. The in-vitro gelling capacity of the prepared formulations was assessed by placing 5 ml of the gelation solution (0.1N HCL, pH 1.2) in a 15 ml borosilicate glass tube and maintaining it at 37±1°C. One millilitre of formulation solution was added with a pipette. The wording was changed so that the pipette was near the fluid's surface in the test tube and the formulation wan gradually released. When the solution came into contact with the e gelation solution, it immediately transformed into a stiff gel-like structure. The stiffness of the gel and the amount of time it took for the gel to form were used to assess the solution's gelling ability. The in-vitro gelling ability was separated into three groups according to the gelation time and the length of time the gel was produced.
(+)After a few minutes, gels quickly spread.
(++) Gelation lasts for 12 hours right away.
(+++) Over 12 hours pass after immediate gelation. [24]
Duration of in vitro floating
The USP dissolving apparatus II with 900 milliliters of hydrochloric acid (0.1 N) was used to determine the in vitro floating research. Ten milliliters of in situ gel compositions were transferred while the dissolving media was maintained at 37 degrees Celsius. It was recorded how long it took how long it floated continuously on the surface of the dissolving media (floating duration) and how long it took for the formulation to show up on the medium surface (floating lag time). [25] Duration the gel remains floating in simulated gastric fluid.
Ideal:>8-12 hours.
Floating Lag Time
In a dissolving flask, the floating lag time is the amount of time it takes for the gel to rise from the bottom. A Type II USP dissolving test apparatus using 900 cc of 0.1 N HCl at 37°C is used to visually observe the floating lag time. [25] Time taken to float after contact with the medium.
Ideal: <1 minute
Drug Release Study in-vitro
The USP Type II was used to perform the in vitro release investigation. II dissolution test apparatus (Paddle Method, Karl Kolb, Germany). At 37±0.2°C and 50 rpm, 900 ml of dissolving medium (0.1 N HCl, pH 1.2) were used. For fifteen, thirty, forty-five, one, two, four, eight, and twelve hours at a time approximately 1 milliliter of the sample was extracted and promptly replaced with the new dissolving medium. Using a UV-visible spectrophotometer, the spectrophotometric technique was employed to ascertain the drug concentration in the extracted sample. Three readings of each measurement were taken, and the average reading ±SD was noted. [26]
Target Release pattern:
|
Time (hours) |
Cumulative Drug Release (%) |
|
1 hour |
10-20% |
|
4 hour |
40-60% |
|
8 hour |
80-90% |
|
12 hour |
~100% |
Drug Release Kinetic Studies
The study was conducted using a variety of mathematical models, such as the Pappas equation, Higuchi's square root, Hixson-Crowell cube root rule, zero order, and first order. drug release kinetic experiments. The correlation coefficient (R) value in several models is used to choose the model that best matches the release data. The model that most closely matches the data from the release is the one with a high "R" value. The regression coefficient (R2) and the release constant were computed using the slope of the relevant graphs. [27]
Density Measurement
75 ml of 0.1 N hydrochloric acid (pH 1.2) was put into a 100 ml measuring cylinder and weighed. The volume and weight were recorded following the addition of 10 millilitres of in gel solution. It was concluded that the floating in situ gel's density (g/ml) ought to be less than that of the stomach contents. The mean and standard deviation of the results, which included at least three measurements, were displayed. [28]
Measurement of Density of Gel
In a beaker, 50 milliliters of 0.1N HCl were mixed with thirty milliliters of the in situ formulation. Ten milliliters of the gel that had developed in a measuring cylinder were weighed. The mass and volume were both utilised to determine the density of the gel. [29]
Water Uptake By The Gel Is Measured.
The water uptakes by the gel of the selected sodium alginate formulations were measured using a simple method. The gel that was produced in situ in 0.1 N HCL pH 1.2 was utilized in this investigation. Each formulation's gel component was removed 0.1 N HCl, and any more HCl solution was wiped off using tissue paper. Ten milliliters of distilled water were added to the gel after its initial weight was determined. The water was then decanted every half hour, and the gel's weight was recorded. After that, the weight difference was calculated and reported. [30]
Measurement of Gel Strength
This gel strength provides insight into the gelled mass's tensile strength. It provides the gelled bulk with the capacity to tolerate internal peristaltic motions. Both the cationic source and the gelling agent concentration affect gel strength. A 50 ml beaker was filled with 30 g of the gel, and a 50 g weight was set in the middle of the gel's surface and allowed to pass through. For each formulation, the amount of time it took for the 50 g weight to pierce the gel 5 cm was recorded. [23]
FUTURE PROSPECTS
The distribution of herbal drugs is a new area in pharmacy. One innovative method for improving medicine delivery is the application of floating drug delivery methods for herbal remedies. This is a great opportunity to work on GI transit profiles reason. As a result, new products have emerged that offer patients significant advantages. Since the introduction of FDDS, products that release the medication for up to 24 hours have been developed. The following herbal remedies can be administered by floating medication delivery systems: Black Myrobalan, Ginger, Turmeric, Licorice [15]
CONCLUSION
According to the review above, among many other benefits, the in situ gelling system helps with the prolonged and controlled release of medications, decreases the frequency of doses, and improves patient compliance and comfort. One advantage of such a system is improved absorption of drugs that are absorbed from the upper part of the stomach. The system remains in the stomach for an extended amount of time. Which increases the local activity of the medication since it has more opportunity to interact with the gastric mucosa. Under situ gel formation occurs under a variety of physiological conditions. In situ gel formulations can be improved as a drug delivery strategy and made more palatable by using water-soluble and biodegradable polymers. The development of liquid orals with prolonged drug release has a lot of potential, thanks to in situ drug delivery. This floating in situ gel method works well for medications that have a limited window for stomach absorption or that have a local impact there. All things considered, floating in situ gels show great promise for enhancing the efficacy and efficiency of many medications, particularly those that need targeted stomach administration or prolonged release. Ionic conditions, pH, and temperature all affect the stability and biocompatibility of in situ gel. As a result, it served as a. It features an improved drug release, making it a more dependable dose form than the traditional one.
REFERENCES




Anushka Deshmukh, Dr. Arun Mahale, Dipali Rathod, Venkatesh Nalabale, Floating In Situ Gel Systems: A Novel Approach for Prolonged Gastric Retention, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 1871-1885. https://doi.org/10.5281/zenodo.15879213
 10.5281/zenodo.15879213
10.5281/zenodo.15879213
