Ashokrao Mane Institute of Pharmacy, Ambap, Kolhapur -416112.
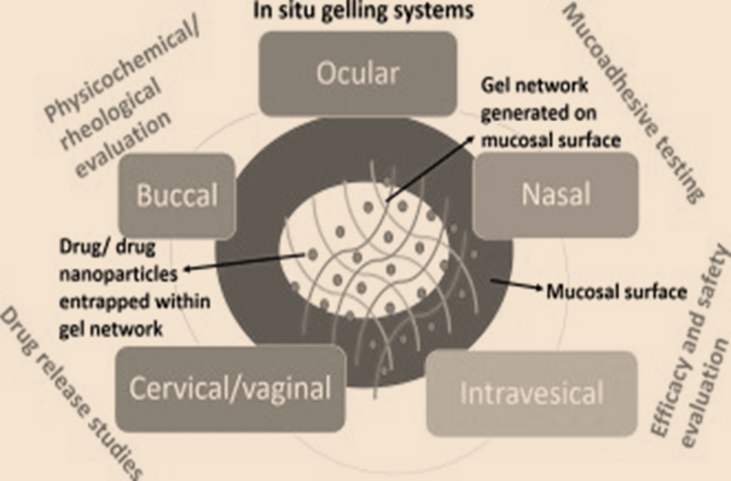
A great deal of investigation has already been done to increase the efficacy and safety of the medicinal products currently available. These medicines use a regulated and prolonged administering method. Due to its benefits over conventional drug delivery systems (DDS), including increased adherence among patients, a longer-lasting sustained activity of drugs, and less frequent medication administration, in situ gels have become a significant novel drug delivery system (NDDS) within recent years. Drug delivery methods, known as "in situ, gelling compositions, " are typically liquids at room temperature that solidify from gels when applied to the human body by several stimulations, including pH, temperatures, and ionic composition changes. This refers to a process involving in-situ gelling. Certain polymers are exposed to the in-situ formation of gels, which can be used for specialized drug delivery methods. To draw particular attention to this, an analysis will be done of the clinical parts of in situ gel-forming technology that have been looked into for likely biologically uses over the past 10 years. They will unavoidably also talk about formulation-related problems that have impeded the clinical translation of certain remarkable medicinal preparations from the preclinical lab. This paper offers a comprehensive overview of in situ gels, including information on how they function, the various polymers they use, and their applications.
In situ gel formulations for suspensions or solutions that gel after application. The unique idea of producing a gel during situ initially emerged during the first decade of the 1970s (al., Lalit Kumar et, 2011). According to studies, several in situ gel formation mechanisms have a long precorneal residency time. Traditionally, the greatest alluring aspect of these novel techniques is in situ gel formation. Many polymeric combinations have been utilized effectively in manufacturing (al, Nirmal H. B. et, 2010) . The beginning of the 1980s saw the introduction of the novel idea of making a gel in situ. The cross-linking of the chain of polymers, which may be either covalent (chemical cross-linking) or non-covalent (physical cross-linking), is what causes gelation (Katarina E, Johan C, Rogaer P, 1998) . Gels are slightly bigger yet denser than tiny particles of liquid that are compact, semi-solid, and scattered across liquids. Hydrogels are defined as aqueous gels prefixed with 'hydro'. The term "hydro" describes a substance that already absorbs water. The cross-linked water-based network of polymers is known as hydrogels. Hydrogels can retain their three-dimensional form even after they expand and take in large amounts of a pool of water. Hydrogels are pre-formed or in-situ. Conventional hydrogels are simple, viscous liquids which solidify after injection, whereas in situ gels are liquids along with solutions of which gel because they alter physically at the exact location (Huffman, AS., et al. , 1986) .
The Essential in Situ Gel Formation Process:
Ideal Polymers for In-Situ Gel Preparations (Rajas NJ, Kavitha K, Gounder T, Mani T., 2011) (Khode PD, Dongare PA., 2019) .
Pros Of in Situ Gel Mechanism:
Disadvantages Of in Situ Gel System (Kubo W, Konno Y, Miyazaki S, Attwood D., 2004) , (Jothi M, Harikumar SL, Aggarwal G., 2012) :
Pharmaceutical Application: (am, ahmed, 2002), (LAKHTAKIA, RITU, 2011) (M. Patlak, 2002) .
Pharmaceutical uses for oral in situ gel formulations include the following:
i. Controlled Drug Delivery:
Drugs can be released from in situ gels in a regulated manner, extending their duration of effect and lowering the dosage frequency. This is especially helpful for medications that need prolonged release characteristics or have a limited therapeutic window.
ii. Improved Bioavailability:
By prolonging medication preservation in the oral cavity, gels improve medication absorption and bioavailability when used in situ.This is advantageous for medications prone to first-pass metabolism or low solubility.
iii. Localized Drug Delivery:
For localized medication administration, in situ gels can target certain areas of the mouth cavity, such as the buccal mucosa or periodontal pockets. Treating illnesses, including periodontal disease and mouth infections, can benefit from this.
iv. Ease of Administration:
In situ, gels provide a practical and patient-friendly method of administration, particularly for older and paediatric patients who might have trouble swallowing pills or other traditional dosage forms.
v. Taste Masking:
Drugs with disagreeable tastes can be made into in situ gels, which can increase patient acceptance and compliance—especially for older and paediatric patients.
Categorization of drug delivery methods in situ:
According to the following method of action:
1. pH-sensitive gel
2. Gel that is electrical current sensitive
3. Gel that Thermo-sensitive gel
4. Sensitive to Enzymes
5. Ion presence
Depending on the administrative route
1. Oral delivery of in situ developing polymeric systems
2. Ocular delivery using in situ formed polymeric systems
3. Rectal as well as vaginal delivery using in situ forming polymeric systems
4. Injectable medication delivery systems that develop in situ
6. Nasal delivery techniques with in situ forming (Kant A, Reddy S, Shankraiah MM, Venkatesh JS and Nagesh C, 2011).
Bioactive agent-based in situ gel formation administration studies:
Buccal Formulations:
Semisolid dosage forms are essential for buccoadhesive medication administration since they treat fungal, inflammatory, and periodontal illnesses in the oral cavity. Semisolids have several advantages over solid dose forms, including easier insertion in the periodontal pocket and syringability. They also have a more agreeable mouth feel. However, two significant disadvantages of these formulations are their limited capacity to administer a defined quantity of medication in contrast to unit dosage forms and their low retention at the application site (E. Russo et al, 2016) . In order to get over this problem, LC nanoparticles are frequently formed in solution by dispersing bulk phases using high shear homogenization or ultrasonication. The resultant LC nanoparticles' internal mesophase frequently matches the bulk non-dispersed phase's. (Vigani, S. Rossi, G. Sandri, M.C. Bonferoni, C.M. Caramella, F. Ferrari, 2020) . Most ophthalmic in situ gelling formulations that have been published aim to eradicate glaucoma, an eye condition that can cause irreversible vision loss and blindness (Vigani, S. Rossi, G. Sandri, M.C. Bonferoni, C.M. Caramella, F. Ferrari, 2020) . Usually, surgery, laser surgery, and regular medication administration are used to treat this pathological condition (Boyd, B.J., Dong, Y.-D., Rades, T.,, 2009) . Medications used for glaucoma include beta-blocker medications (betaxolol, timolol), agonists of cholinergic neurons (pilocarpine), α2-agonists (brimonidine), and carbonic anhydrase antagonists (brinzolamide). Carbonic anhydrase inhibitors are recommended for patients who do not respond to beta-blockers or whose medical circumstances prohibit them from using them (H. Bhalerao, K.B. Koteshwara, S. Chandran, 2020) .
Drug Absorption Pathways
Drug transport across the buccal region occurs via two primary processes: transcellular (intracellular) and paracellular (intercellular) (Fig. 1). Intercellular gaps are the primary route for bigger molecules to cross-stratified epithelium, as indicated by studies employing microscope-visible trace elements including small proteins as well as dextrans. These spaces act as a barrier to penetrating because of alterations in the intercellular material in the surface layers. The extracellular space's lipid framework is widely considered critical to the paracellular pathway's barrier effectiveness, especially during the presence of hydrophilic, highly molecular weight molecules like peptides (Rathbone MJ, Tucker IG. ., 1993) . The buccal mucosa's absorption capacity is affected by the diffusant's lipid solubility along with molecular weight. Certain drugs are absorbed more effectively via the buccal mucosa whenever the pH of the carriers is low and less absorbed when the pH is high (Nielsen HM, Rassing MR., 1999). Peptide medicines are commonly considered to enter the buccal epithelium through passive diffusion through a paracellular route. It was recently discovered that drugs containing monocarboxylic acid residues could enter the bloodstream via the oral mucosa and be transported by the carrier (Utoguchi N, Watanabe Y, Suzuki T, Maeharai J, Matsumoto Y, Matsumoto M., 1997) . Several in vitro and in vivo models are being utilized to investigate the permeability of the mucus membrane in the mouth and the efficiency of penetration boosters. The permeation rate of the oral mucosa is currently measured using many diffusion cell kinds, including Franz diffusion cells, Employing chambers, constant-flow perfusion chambers, and Grass-Sweetana (Squier CA, Kremer MJ, Wertz PW., 1997) . Using cultivated epithelial lines of cells, in vitro studies of drug transport along with metabolism across biological barriers and potential mechanisms of action with penetration enhancements have been established (Brun PPHL, Fox PLA, Vries MED, Bodde HE., 1989). According to current speculation, investigations on the buccal delivery through enzymes varying medications, such as leu-enkephalin, have shown promising results in vitro using the TR146 cell culture model, which mimics human buccal mucosa.
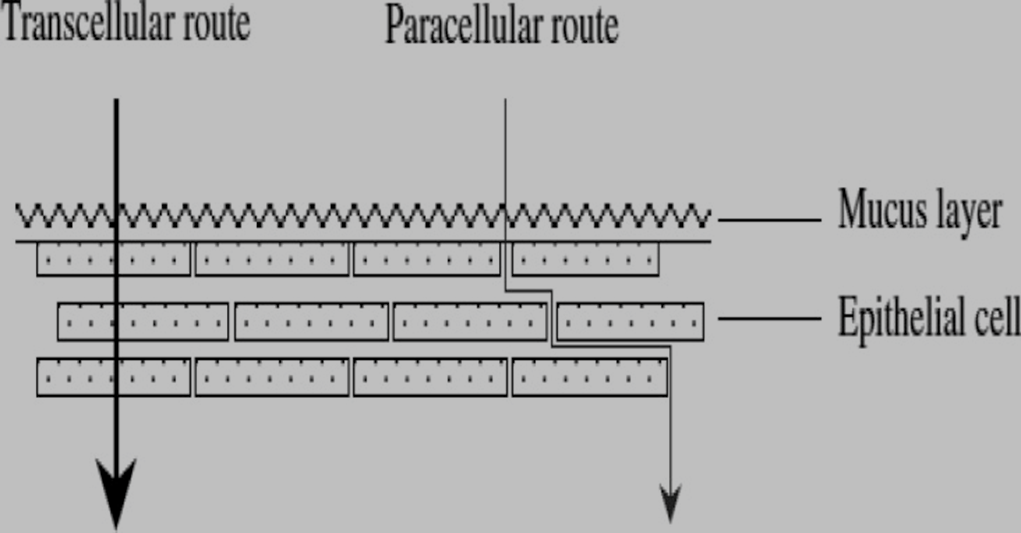
Fig: 1(Diagrammatic representation of the penetrating channels in buccal medication delivery)
Evaluation -
Determination of drug content
Specifically, 10 millilitres of preparation, equal to 250 milligrams of metronidazole, were collected from different trials and transferred to a 100-millilitre volumetric container. Add 50–70 ml of 0.1 N HCl and sonicate for 30 minutes. There has been a 100-milliliter volume adjustment. A look inside indicated that its components were fully disseminated. Therefore, that the fluid was passed through utilizing Whatman Filter Paper. A 10 ml amount of the mixture was obtained and liquefied in 0.1 N HCl to yield 100 millilitres. A UV-visible spectrophotometer found metronidazole's peak absorption around 278 nm. (Biotech eng. ultraviolet (UV)-9200, UK) (Rajalakshmi R, Diwakar Reddy N, Mothilal Naik B, Rajendra Babu V, Vijay Kumar A, Vinesha V, et al., 2013)
pH Measurement
We used a regulated digital pH test on the devices to determine the mixtures' pH (Schott Gerate, Germany) (Patel MJ, Patel KR, Patel MR, Patel NM.., 2012) .
In-vitro gelation study
To test how well the solutions could gel in the lab, 10 mL of the preparation was mixed with 100 mL of a 0.1N solution containing hydrochloric acid (HCl, pH 1.2) within a glass beaker that was kept at 37 degrees Celsius and stirred occasionally to keep the gel from breaking. In vitro gel formation ability was categorized into three groups depending on the rigidity of the generated gel, the gelation duration, and the amount of time that the created gel remained.
(+) Gels seemed immediately disseminated within a few minutes.
(++) Gel formation occurs quickly and lasts for several hours.
(+++) Gel formation occurs quickly and lasts for a long time (Vipul V, Basu B., 2013) .
Measurements of viscosity for an in-situ gel-forming mechanism
The dispersion's viscosity has been measured utilizing a Brookfield NDJ-5S electronic viscometer. Using spindle number 2, the 200 mL samples were sheared at 100 rpm/min at room temperature. Every sample had its viscosity measured in triplicate, taking around 30 seconds for each measurement (Rani K, Garg V, Goswami DS, 2013) .
In vitro Floating research-
Despite no noticeable disruption, a in-vitro floating experiment included adding 10 mL of the solution into a cylindrical vessel that contained 100 mL of 0.1N HCl (pH 1.2) at 37?C. The floating lag period (the period of time that it took for the solution to become visible on the medium's surface) & the floating endurance (the span of time it stayed floating over the dissolving medium's surface) were further recorded (Mahagen Y, Patidhar V, Balaram Y, Gopkumar P, Sridevi G, 2014) .
Nasal Formulations:
The Indian medical system, known as Ayurveda, recognizes intranasal medication as a legitimate kind of treatment. In the past few years, it has been demonstrated that administering medications nasally instead of orally improves their systemic bioavailability. The nose's mucous membrane is permeable to chemical throughout the gastrointestinal system due to the lack of pancreatic as well as stomach activity of enzymes, however it is advised for pharmaceutical administration to improve absorption (Aishwarya J Jadhav, Sheetal B Gondkar, Ravindra B Saudagar., 2014) . Progressively molecule sizes increase, nasal absorption diminishes. One of the biggest obstacles to nasal drug administration is mucociliary leaks. It cuts drug absorption time significantly. On the other hand, mucoadhesive materials boost dosage form interaction with the nasal cavity mucosal layers. (Gowda D.V, Tanuja. D, Mohammed S. Khan, et al., 2011), (Jadhav R, Gambhire MN, Shaikh IM. , 2007), (Nagesh C, Manish Patil, S Chandrashekhara., 2012), (IR, Schmolka, 1972), (Sudam Nagargoje, Atul Phatak, Chandrashekhar Bhingare, et al, 2012). Intranasal micro emulsions, gels, & microspheres have been receiving greater interest as a technique of delivering protein as well as peptides through the nose (Kushwaha SKS, Keshari RK, Rai AK., 2011) .
Drug Absorption:
When a drug reaches the nasal cavity and travels throughout the mucous membranes as well as epithelium prior to accessing the systemic circulation and central nervous system (CNS), ability to speak absorbed via the nasal route and has an effect on both the systemic along with CNS. Systemic medication absorption occurs in the respiratory region, including the turbinates along with nasal septum. Beyond the pulmonary region, the area around the nose absorbs most central nervous system medications. Drugs delivered by the nose can get to the brain via the olfactory area, systemic circulation, or trigeminal neural networks. Drugs go through the nasal cavity to cerebrospinal fluid. Therefore, molecules of medications working as the central nervous system (CNS) within depression, migraine, schizophrenia, seizures, brain tumors, psychosis, pain, Parkinson's, and Alzheimer's may be addressed to the nasal mucosa's olfactory, connecting the nose and brain. The nasal passageways carry absorption drugs to the mucus layers. The absorption process begins here. Charged medications are bigger and harder to pass through mucus compared to small-particle drugs. Mucus' main protein, mucin, binds molecules and hinders diffusion. Environmental factors like pH and temperature may affect mucous layer structure. Medicine absorption through the mucosa varies. Transcellular (simple membrane diffusion) as well as paracellular (cell motions and transcytosis via vesicle carriers). A drug's time in its cavity after absorption is limited, and it may be processed before reaching the systemic circulation. Medication transport across the nasal epithelium might have occurred in many ways, including diffusion (transcellular), (Ban MM, Chakote VR, Dhembre GN, Rajguru JR, Joshi DA, 2018) (Kaur P, Garg T, Rath G, Goyal AK., 2016), (N TN, R DM., 2019) .
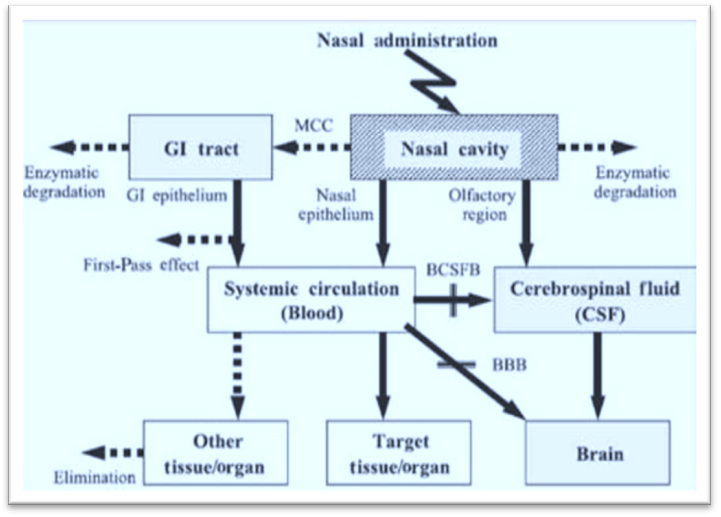
Fig. 2 Mechanism of drug absorption by nasal route
Evaluation –
Drug content
The amount of medication in the preparations was measured threefold with a Shimadzu UV-1800 double-beam Ultraviolet-visible spectrophotometer. One millilitre of the mixture was put into a volumetric container with a capacity of 10 ml that could hold 10 ml. This was subsequently diluted using double-distilled water to make the amount 10 ml. One millilitre of the resulting solution was diluted once more with ten millilitres of water that had been double-distilled. Finally, the UV-visible spectrum spectrophotometer measured the solutions' absorbency at 226 nm (V., Gaikwad, 2010).
pH
The Equip-Tronics EQ-610 computerized pH meter (India) underwent calibration using pH buffers 4 and 7. A beaker had 20 milliliters of each combination, and the glass electrode was plunged deeply within the chemical. The mixture's pH has been verified three times. The pH values of each preparation ranged from 4.66 to 5.53, which is within the usual nasal pH range from 4.5 to 6.4 (Nisha GS, Maithi P, Charyulu RN, 2012).
In-vitro drug release study
The six-cell thermoregulated Franz diffusion cell system (Thermo Fischer Scientific, Haake S5P Newington, USA) tested the gel's release of drugs within in vitro. Two hours before usage, artificial dialysis membranes (1200-1400 KDa) were pre-soaked within a receptor medium. At 34 ± 1°C, the receptor chamber was filled with 12 cc of pH 6.4 phosphate buffer saline. A gel containing 2.5 milligrams of the drug was put within a donor compartment, and the apparatus was constantly agitated. We removed 1 ml aliquots through receptor compartments at predetermined intervals and added new buffer for 12 hours. Before spectrophotometric measurement at 283 nm, the compounds were diluted suitably. A curve for calibration was then utilized to determine the amount of medicine discharged. The DD solver programme was utilized to study release kinetics (Z. Yong, M. Huo, J. Zhou, A. Zou, W. Li, C. Yao, S. Xie,, 2010) .
Ocular Formulation:
Due of the anatomical, physiological, as well as defensive properties of the lens of the eye, among the most difficult challenges in drug delivery is getting drugs targeted to tissues within the eye (Ludwig, 2005) , (Pijls, 2005). The ocular medication delivery system is viewed as both necessary and problematic considering the human eye has a single organ, making drug delivery highly difficult. Because solutions drainage, lachrymation, and inadequate absorption via the conjunctiva quickly and completely remove medications out of pre-corneal lachrymal fluid, normal eye medication had little residence length and limited bioavailability (AH, EL-Kamel, 2002)
Drug absorption:
The cornea is a representative of the primary biological barrier to drug penetration. Three of the five tissue types that comprise the human cornea—the endothelium, inner stroma, and epithelium—act as the primary absorption barriers. Figure (3) depicts the pre-corneal along with intraocular drug transport through topical dosages. Conventional solutions for the eyes have inadequate bioavailability and treatment response because of rapid pre-corneal elimination of the medications. To address this, a gel framework implanted as decreases into the eye can be used. The rest has been washed away along with absorbed by means of the nasolacrimal duct as well as the mucosal membranes of the nose, oropharyngeal, and GI systems (Shastri DH, Patel LD, 2010).

Fig: Drug absorption in Cornea
Evaluation –
Ocular irritancy
Four male albino rabbits weighing between two and three kilograms were used in an optimised formulation for ocular irritation research. For 14 days, every rabbit was given 0.1 ml of a sterile, optimal dosage of moxifloxacin hydrochloride twice a day. The rabbits had been periodically observed for signs of eye oedema, redness, and wetness (Draize J, Woodward G, Calvery O., 1994).
Accelerated stability studies
The optimal sterile solution underwent stability testing. Glass vials containing tailored, sterilized optic solutions have been sealed with covers. Vials of the improved formulation were kept in a chamber designed for stability for one month at 40 ± 2°C and 75 ± 5% humidity. It was possible to take samples every week and test the drug content, pH, gelling ability, and in vitro drug release (Mathews BR. , 1999).
Intravesical Formulation:
The urinary bladder plays a crucial role in holding onto urine produced by the kidneys and keeping urine components from the bladder cavity from being reabsorption by the body until urination (Lewis, S.A.,, 2000) . An alternate method of administering medication is through urethral catheter distribution of intravesical drug delivery devices (IDDS). When medications are administered intravenously, substantial drug concentrations are produced in the bladder tissue, improving therapy effectiveness (Guhasarkar, S., Banerjee, R.,, 2010) .Numerous innovative intravesical injections were documented, the primary goal of which was to increase the duration of medication residence in the bladder. Temperature-sensitive hydrogels with sol-gel transitional properties, such as Poloxamer 407 (P407), are of great interest (Jeong B, Kim SW, Bae YH., 2012), (Xu K, Wang L, Qiang M, Wang L, Li P, Tang B., 2011) .Among the more modern IDDS methods is the use of a gel in situ to prolong the period of drug residence after intravesical delivery (Tyagi, P., Kashyap, M., Hensley, H., Yoshimura, N., ., 2016) . There has been some curiosity about in situ gelling solutions as possible targeted and long-term chemotherapeutic administration methods. Controlled drug release is possible when sol systems transform into hydrogels responding to particular stimuli. The hydrogel's shape in three dimensions sustains drug release, extending the tumor's responsiveness to chemotherapeutic treatments, increasing anticancer benefits, and decreasing systemic side effects (Shaker, D.S.; Shaker, M.A.; Klingner, A.; Hanafy, M.S., 2016), (Zheng, L.; Li, C.; Huang, X.; Lin, X.; Lin, W.; Yang, F.; Chen, T., 2019).
Blood urine barrier:
For drugs to be therapeutically effective after luminal delivery, they need to cross a watertight barrier and enter the urine bladder. The uterohelium represents the body's strongest and most impenetrable barrier (Parsons CL, Boychuk D, Jones S, Hurst R, Callahan H., 1990) . Preventing the entry of injectable drugs and urine contents is an equally effective use of the urothelium, which regulates numerous physiological processes (MM, Melicow, 1978), (podaca, G., 2004) . It prevents harmful metabolites, ions, and solutes from exchanging uncontrolled by forming a barrier at the urine-connective tissue interface. Chemicals that ordinarily move quickly across the membrane, such as water, ammonia, and urea, have poor urothelium permeability (MM, Melicow, 1978), (podaca, G., 2004) . It has an extremely high transepithelial resistance. This ranges from 10,000 to more than 75,000 Wcm2, depending on the combination of the paracellular impedance of close junctions and the transcellular impedance of the plasma membrane at the apical end (Lewis SA, Diamond JM., 1976) (Negrete HO, Lavelle JP, Berg J, Lewis SA, Zeidel ML., 1996) . Tight urothelial connections exhibited the greatest paracellular resistance of all epithelia studied. They include transmembrane proteins (occludin and claudins), cytoskeletal components, and cytoplasmic proteins (zonulaoccludens-1) (Khandelwal P, Abraham SN, Apodaca G. ., 2009) . More specifically, extracellular resistance is caused by uroplakins, a group of unique proteins found in the urothelium's apical plasma membrane. Electron microscopy of umbrella cells directed toward urothelium's luminal region has shown that uroplakins are structured like a hexagon, with all six parts of each particle tightly connected to create a complete ring. Lipids are present in the central cavity of all particles (Min G, Zhou G, Schapira M, Sun TT, Kong XP., 2003) . Urothelial barriers are believed to have poor permeability due to a peculiar protein structure and strong intercellular interactions.The Urothelial obstruction limits not just the transportation of drugs after intravenous dosage but also the active medicinal product component's activity in the urine. Because of this, many drugs do not have any pharmacological effects since they do not reach the urinary system at the right therapeutic doses (Khandelwal P, Abraham SN, Apodaca G., 2009), (Min G, Zhou G, Schapira M, Sun TT, Kong XP., 2003) .
Evaluation-
Histopathological evaluation
A 4-hour ex vivo permeation test discarded surplus formulations and archived mucosa specimens within 4% neutral-buffered formalin. Using standard methods, 4 mm tissue slices were made and stained with hematoxylin along with eosin (Gomez P 3rd, Gil ES, Lovett ML, et al., 2011) .
Syringe ability of formulations
The force needed to remove chemicals through an injection device has been measured employing a force transducer coupled to the TA-XT Plus texture analyzer. After a brief time, solutions that have been prepared were placed in 2 mL polypropylene syringes as well as linked to a catheter. After that, the plungers of the syringes were repeatedly squeezed with 0.5 N of force while being inserted into metallic supports. The resistance due to the syringe materials expressing themselves throughout a catheter following plunger contractions was determined using the area beneath the force-time curve at 25°C (n=6) (Jones DS, Woolfson AD, Brown AF, Coulter WA, McClelland C, Irwin CR., 2000) .
Bioadhesive properties of formulations
The recipes' bioadhesive qualities were evaluated using the TA-XT Plus texture analyser and a 5-kilogram load cell. After obtaining fresh cow mucosal bladder tissue from a local slaughterhouse, it was meticulously cleaned, sliced, and separated from the adjacent tissues. Certain sections with a thickness of 2 mm were removed from the interior of the mucosal membrane and affixed to the bottom of 10 mm-diameter texture analyser probes. The gels were kept at 37°C and put at the bottom of a 10-mm-diameter texture analyzer probe. After placing the gel-containing probes against the bladder's mucosa regions at a steady speed of 0.1 mm/s, a 2-minute force of contact was delivered using 0.05 N. Following then, the probe was raised vertically at a steady rate of 0.1 mm/s. The forces-distance plot yielded the area under the curve (AUC), also known as mucoadhesion, and the highest detachment force (F) (Baloglu E, Karavana SY, ?enyi?it ZA, et al., 2011).
Vaginal Formulation:
It has long been known that drug delivery by vaginal birth can produce pharmacological impacts that are both local as well as systemic. The vaginal route has several advantages over the parental route, such as preventing first-pass metabolic processes, lowering digestive and hepatic side effects, and minimizing pain, harm to tissue, and infection. Poor retention, disarray, and leakage are among the disadvantages of the traditional vaginal dose forms (such as semi-solids, tablets, capsules, pessaries, liquid preparation, vaginal films, vaginal rings, foams, and tampons), which irritate users and decrease therapeutic efficacy (Bilensoy E, Rouf MA, Vural I, et al., 2006), (Neves J, Bahia MF, 2006), (Patel P, Patel P., 2015) . Furthermore, rectal and vaginal delivery are options for in-situ gels. The aforementioned medication is an anti-inflammatory drug produced as a kind of liquid suppository gelled in situ using synthetic polymers like polycarbophil, poloxamer F188, and poloxamer 407. This method should improve bioavailability. Itraconazole, an anti-inflammatory, is manufactured as a uterine in-situ gel with poloxamer 407, 188, along with HPMC for vaginal candidiasis. There are additional allegations of vaginal clotrimazole administration (Kast CE, Valenta C, Leopold M, Andreas BS., 2002) .
Mucoadhesive Approach
A lamina propria supports the stratified, multi-layered squamous epithelial cells that make up the healthy vaginal mucosa. The stratum basale, suprabasal, and stratum corneum make up the epithelium after differentiation. The epithelium that covers the vagina changes with hormones and environments throughout a woman's lifecycle. Girls' genital epitheliums are thin and basal along with parabasal before puberty. While the reproductive system grows, the vaginal epithelium thickens as well cornifies. It thins immediately after menopause, lowering a glycogen storage capacity, and the stratum corneum gets started to keratinize. In BV, mucins in the vaginal stratum corneum help bacteria connect and stay (Baloglu E, Karavana SY, ?enyi?it ZA, et al., 2011). Mucin is the primary component of mucus, including lipids, water, and proteins, along with cells to produce a coating resembling gels in the mucosal tissues (Ways, T.M.M.; Lau, W.M.; Khutoryanskiy, V.V., 2018) . Due in large part to the vaginal self-defence mechanism's inadequate absorption as well as retention of medications across the vaginal epithelium, non-mucoadhesive preparations are still difficult to carry successfully throughout the vagina ( Gu, J.; Yang, S.; Ho, E.A. , 2015) (Ways, T.M.M.; Lau, W.M.; Khutoryanskiy, V.V., 2018) .
Evaluation-
Microbiological studies
In the microbial investigations, 2% w/v of a plain medicine solution and the enhanced preparation served as a baseline versus bacteria. We shall be using Staphylococcus aureus as the specimen bacterium. A 20 mL layer of nutritional agar containing 0.2 mL of the test microorganisms was planted and allowed to settle within the Petri plate. Upon the agar-based layer that had set, cups were made using a sterile borer that had a 4 mm diameter. Subsequently, each cup will have an equal volume of both the improved formulation and the basic medication solution. Petri plates were permitted to come to room temperature for four hours before being placed in an incubator for twenty-four hours at 37°C. The inhibitory zone was discernible. We'll determine the diameter within the inhibition region using an antibiotic, the area finder (Hatefi A, Amsden B., 2002), (Vernon BL, Fusaro F, Borden B, Roy KH, 2004) . Irritation test (Hen’s Egg Test-chorioallantoic membrane test). This study used the (Velpandian T, Bankoti R, Humayun S, Ravi AK, Kumari SS, Biswas NR, 2006). technique for performing modified Hen's Egg Test-chorioallantoic membrane (HET-CAM) testing. The HET-CAM has shown to be a reliable approach for assessing a chemical's ability to produce pain. Having an eye toward negative alterations inside the egg's chorioallantoic membrane after being subjected to test substances that might irritate were discovered (H., Spielmann, 1997). To summarize, the fertilized hen eggs came from a chicken farm. Each batch of each concoction comprised three eggs weighing 50-55 g. The fertilized eggs were kept in an incubator with a humidity at 37°C ± 0.5°C for three days. During the third occasion, sterile methods extracted three millilitres of egg albumin from the sharpest end. Use a heated spatula to cover the hole with 70% alcohol-sterilized parafilm (American Can Company, USA). Researchers kept eggs equatorial so CAM could develop away from their shells. Day five during incubation saw the eggs candled and non-viable larvae removed daily. The eleventh day involved immediately injecting formulations onto CAM as well as letting them stay for five minutes. We measure wound formation time and membrane vascular damage.
Physicochemical evaluation of the prepared formulation
T gel is the liquid-to-gel temperature. When applied frequently at the place of application site, a continuously flowing liquid around ambient temperature that passes through an in situ transition of phases to create a strong gel is ideal for an in situ gel (Anderson, D.J.; Marathe, J.; Pudney, J.; Anderson, D., 2014) . Human vaginal temperatures are 37.2°C (Kim EY, Gao ZG, Park JS, Li H, Han K., 2002).
Example Of Formulations
|
Buccal |
Dapagliflozin (LAKHTAKIA, RITU, 2011) |
|
Ocular
|
Ciprofloxacin Hydrochloride (Eaga Chandra Mohan*, Jagan Mohan Kandukuri, Venkatesham Allenki., 2009) |
|
Nasal
|
Sumatriptan succinate (Upendra C. Galgatte, Amruta B. Kumbhar, and Pravin D. Chaudhari,, 2014) . |
|
Intra vesicle
|
Bimatoprost (Monika Yadava, Ana Guzman-Aranguezb , Maria J. Perez de Larab , Mandeep Singha , Joga Singha , Indu Pal Kaura, 2019) . |
|
Vaginal
|
Carrageenan (Yu Liu, Yi-ying Zhu, Gang Wei, Wei-yue Lu, 2009) . |
CONCLUSION:
"In situ gel," among the most cutting-edge drug delivery technologies on the market, has enabled the transition from "sol to gel." When solution or suspension gels (also known as in situ gels) react with fluids that have certain chemicals or ions present, temperature, UV radiation, ionic concentration, or other physiological and physicochemical properties, the reaction takes place. An extended drug time of place of residence at the intended site, fewer medication administration doses, a low dose required for therapy, and a decrease in both localized and systemic negative consequences are just a few of the many notable advantages of the in situ polymeric gel-based formulation. Two drawbacks of in-situ gel systems include the drug's propensity to break down in solutions and stability issues brought on by chemical breakdown. A few of the many notable benefits of the use of in situ polymeric gel-based compositions include increased patient compliance, a longer drugs time of residence at the intended site, fewer doses of medication required for therapy, less medication required in general, and a reduction in both local and systemic adverse reactions. The drug's tendency to degrade in solution and stability issues brought on by chemical breakdown are two disadvantages of in-situ gel structures.
ACKNOWLEDGMENT
Acknowledging the debt is not easy for us as I am indebted to so many people." I take this opportunity in expressing the fact that this report writing is the result of incredible amount of encouragement co-operation, and moral support that I have received from others. I would like to express my deep gratitude to our respected principal Dr. N. B. Chougule sir, I would also like to express my gratitude from the core of my heart to my guide Mr. Pranjal. D. Chaugule sir who helped me and coordinating my entire Review paper . Their consistent support and co-operation should the way towards the successful completion of project. I am also grateful to all other faculty and staff members for their kind of cooperation and help. Lastly, I would like to express my deep appreciation towards my classmates and in definess to my parents for providing me moral support and encouragement.
REFERENCES

Pranoti Ulape*, Pranjal Chougule, Nilesh Chougule, Novel Approaches for In Situ Delivery, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 812-831 https://doi.org/10.5281/zenodo.15168207
 10.5281/zenodo.15168207
10.5281/zenodo.15168207
