Swami Vivekanand College of Pharmacy, Udgir
Breast cancer is one of the most common cancers among women worldwide and a leading cause of cancer – related death. Its occurrence is increasing in both developing and developed countries. Conventional treatment includes surgery, radiation therapy, and chemotherapy. However, these treatments have limitation. Such as high toxicity, poor tumour specificity, side effect, and drug resistance. Chemotherapeutic drug often fail to reach tumour efficiency due to biological barrier and lack of targeted delivery. Nanotechnology has emerged as a promising approach to overcome the limitation of conventional treatments. Polymeric nanoparticles and Nano-formulations are being developed to improve drug delivery target tumour specifically and reduce systemic toxicity. These Nano system helps in prolonging blood circulation, enhancing tumour accumulation and controlling drug release. Improve bioavailability and drug uptake. Reduced side effects and multiple drug resistance. Increased therapeutic efficiency and localised action at the tumour site. Allow use of smaller doses of drugs with higher effectiveness. Paclitaxel, Doxorubicin, Tamoxifen, Exemestane, Bevacizumab, and 5-fluorouracil are a new drug currently used to treat breast cancer. Nano size of formulation allows passage or permeation of drugs through vasculature resulting in the release of encapsulated drug at tumour tissue this review focuses on various Nano formulation such as liposomes, polymeric nanoparticles, Dendrimers, quantum dots, carbon nanotubes, etc. used for treating breast cancer till date along with certain examples which are in clinical trials and marketed formulation.
Breast cancer is one of the most common cancers affecting women across the world. Its occurrence has increased rapidly due to changes in environmental, hormonal, and lifestyle factors. Although many treatments such as chemotherapy, radiotherapy, and hormone therapy are available, they often cause several side effects and sometimes fail to completely eliminate the cancer. Among all types of breast cancer, triple-negative breast cancer (TNBC) is considered one of the most aggressive and difficult to treat because it lacks the hormone receptors– estrogen (ER), progesterone (PR), and HER2- which are normally targeted by most therapies. This make TNBC more resistant to conventional treatments and often results in poor prognosis and higher recurrence rates.
In recent years, nanotechnology – based drug delivery systems have emerged as a promising solution to overcome the limitation of traditional chemotherapy. Nano carriers can improve drug solubility, stability, and bioavailability, as well as deliver drug direct lyto cancer cell while reducing toxicity to healthy tissues. Among various Nano carriers, solid lipid Nanoparticles (SLNs) and lipid Nanoparticles (LNPs) have attracted considerable attention due to their biocompability, ability to encapsulate both hydrophilic and lipophilic drugs and controlled drug release properties. These Nanoparticles are composed mainly of physiological lipids that can safely carry therapeutic agent through the bloodstream, protecting them from early degradation.
One of the most widely studied natural compounds for cancer therapy is curcumin, a bioactive polyphenol derived from the plant curcuma longa (turmeric) . curcumin has shown multiple pharmacological properties, including antioxidant, anti-inflammatory, antibacterial, and anticancer effects. However, it’s poor water solubility, instability, and low absorption rate limit it’s use in clinical practice. To overcome these challenges, curcumin-loaded solid lipid Nanoparticles (Cur-SLNs) have been developed. These Nanoparticles significantly improve curcumins stability, enhance its solubility, and help it to enter cancer cells more effectively.
Research studies have demonstrated that Cur-SLNs can inhibit the growth of breast cancer cells by inducing apoptosis (programmed cell death) and reducing cell proliferation. Additionally, SLNs can modulate the expression of cell cycle proteins such as cyclin D1 and CDK4, which play a major role in tumour growth. Furthermore, surface modification of SLNs-such as PEGylation or antibody coating – can enhance their circulation time and target tumour cells more specifically, thus improving the therapeutic response while minimizing side effects.
In the case of triple-negative breast cancer, where limited treatment options exist, SLNs provide a potential alternative for efficient drug delivery. They can carry chemotherapeutic agents or natural compounds like curcumin directly to the tumour site, maintain the drug concentration for a longer duration, and enhance overall anticancer activity.
Therefore, the development of solid lipid Nanoparticles as drug carriers offers a novel and effective strategy for improving the treatment of breast cancer. By combining modern nanotechnology with bioactive compounds such as curcumin, researchers aim to design safer, more targeted, and more efficient therapies that can overcome the limitation of existing treatments.(1,2)
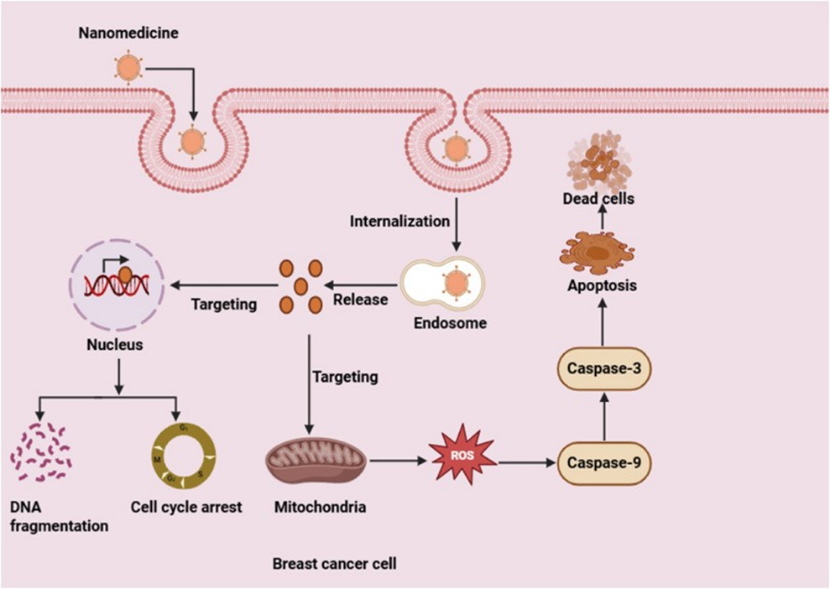
Figure no.1:-Mechanism of drug delivery using solids lipid nanoparticles in breast cancer management
3. BREAST CANCER OVERVIEW:-
3.1 Epidemiology:-
Breast cancer is the most common cancer globally and the leading cause of cancer death in women, with incidence rates increasing worldwide, especially in developed countries due to factors like lifestyle and fertility patterns. Key epidemiological feature includeit’s prevalence in women (over 99% of cases), the significant burden in both developed and, increasingly, developing countries, and a younger aver-age of onset in some population like india.
Breast cancer is the most common invasive cancer in women globally.MIt became the most diagnosed cancer worldwide in 2020, surpassing lung cancer, with an estimated 2.3 million new cases that year. In 2022, breast cancer caused an estimated 670,000 deaths globally. The incidence of breast cancer is increasing in all regions of the world, through it remains highest in industrialized countries. Despite high incidence rates in developed countries, regions with historically low rates are also seeing increases, potentially due to lifestyle and fertility changes.
Approximately 0.5-1% of breast cancers occurs in men.
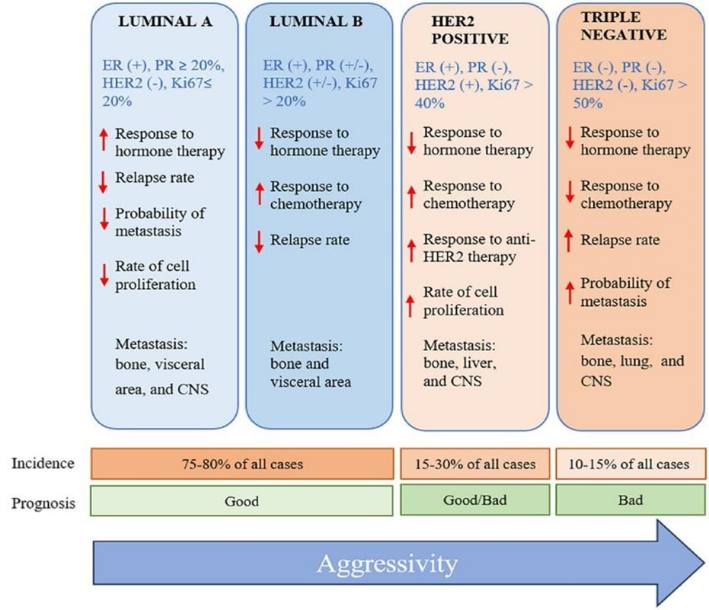
Figure no.2 :- Molecular classification of breast cancer
Breast cancer has been classified by using diverse criteria, including histology, molecular characteristics, and the expression of specific biomarkers. The establishment of the specific characteristics of breast cancer tumours allows for the selection of the most effective treatment. Regarding the molecular perspective, among the various subtypes ofbreast cancer are luminal A, luminal B, normal-like, HER2-enriched, basal-like, and triple-negative. The triple-negative subtype comprises 10–20% of all cases of breastcancer. It is found at a greater prevalence in Afro-descendants, women under 40 years ofage, and/or thosewith a mutation in the BCRA1 gene.(3,4)
3.3 Conventional Therapies :-
Immunotherapy in Cancer Treatment A newer and more advanced way to treat cancer is called immunotherapy.
This treatment uses the body’s own immune system to find and destroy cancer cells. It works by making the immune system stronger or smarter so it can recognize cancer cells as harmful and attack them.
Types of Immunotherapy
Monoclonal antibodies – These are lab-made molecules that can find specific targets on cancer cells. For example, in breast cancer (BC), some drugs block the HER2 receptor, which helps cancer grow. Drugs like trastuzumab and pertuzumab are often used together to block this receptor.
For example,
Nanoparticles In Cancer Treatment
In the last ten years, nanoparticles (NPs) have become an exciting new tool in medicine.
They are very small particles that can carry drugs or RNA (genetic material) into cancer cells.

Figure no.3. Conventional treatments or RNA LNPs therapies
Why Nanoparticles Are Useful
3.4. Limitation :-
Existing treatment strategies have several shortcomings in the treatment of heart cancer, which includes lack of selective toxicity, which leads to diminished therapeutic efficacy and, as an outcome, the medical diagnosis being impaired; injury to healthy tissues and therefore, decreased doses of anticancer medicine are generally delivered to minimize toxicity to normal tissues; poor bio-distribution and drug penetration in solid tumors; heterogenic vessels in tumour site increases extravasation of drugs. Current treatment tend greater drug deposition in normal viscera (10- to 20-fold greater) than that in a comparably loaded tumour site, and several chemotherapeutic agents re unable to permeate from the vasculature more than 40-50 mm (equivalent to the combined diameter of three to five cells) which could result in multiple drug resistance (MDR) and ultimately therapeutic failure. Furthermore, the development of MDR in tumour cells on treatment with one anticancer molecule could generate resistance to an entire range of drugs owing to over – expression of drug efflux proteins. (12,13)
4. SOLID LIPID NANOPARTICLES (SLN) :-
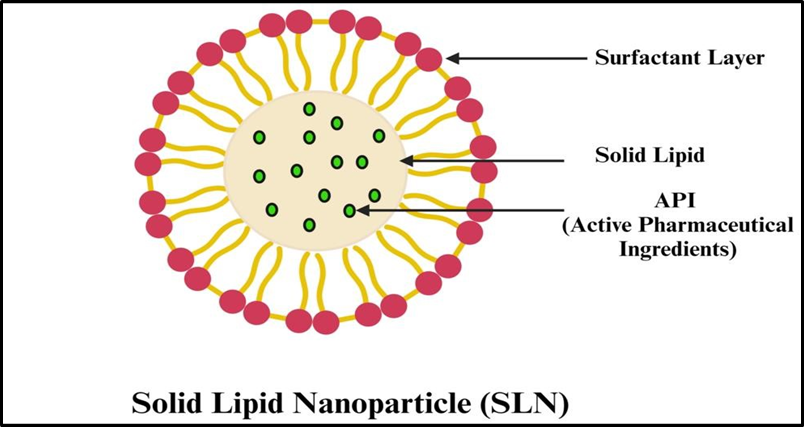
Figure no.4:-Solid Lipid Nanoparticles ( SLN)
Solid lipid nanoparticles (SLNs) are nanoscale carriers used for drug delivery, consisting of a solid lipid core and stabilizers like surfactants. They offer advantages like high biocompatibility, biodegradability, and improved drug solubility and stability. SLNs are produced by methods such as homogenization and ultrasonication and are used to deliver drugs via various routes, including oral, parenteral, and transdermal, and have applications in fields like cancer therapy and cosmeceuticals.
4.1 Composition of SLN :-
Advantages:
Disadvantages:
4.2 Method of (SLN) :-
High-Pressure Homogenization: Dispersing melted lipids and the active ingredient in an aqueous surfactant solution and then homogenizing at high pressure.
Ultrasonication: Using high-frequency sound waves to break down the lipids.
Other Methods: Spray drying, solvent emulsification, and the double emulsion technique.
4.3 Preparation Of (SLN) :-
For the preparation of D-SLNs hot emulsification method was used . The selected BCS class 2 drug tamoxifen citrate was incorporated into the lipid phase along with surfactant (1%w/v) at 10°c above the melting range of the selected lipid. The aqueous phase consisted of
0.5% w/v surfactant solutions in double distilled water. Temperature of aqueous phase was kept same as lipid phase temperature. Both the phases were mixed under continuous stirring at 600800 RPM using magnetic stirrer (Bio Lab BL 223- B ) upto 1 h. To achieve further reduction and uniformity in particle size, the D-SLN were homogenized for 3 cycles per minute by HPH ( APV 2000 model, lab homogenized), using pressure up to 400 bar .(17,18)
4.4 Role Of (SLN) :-
A. Solid Lipid Nanoparticles :-
Solid lipid Nanoparticles are composed of a matrix, surfactants, and sometimes co- surfactants at physiological temperature. SLNs can be formed through various methods, including high- shear homogenization, and ultrasound, hot homogenization, cold homogenization, strong – pressure homogenization, solvent emulsification, evaporation, and microencapsulation. A microemulsion is an easy method that does not require high- level equipment or high energy input and uses an organic solvent. In addition there are some drug incorporation model for SLNs , such as the solid solution and core-shell models. In the drug – enriched shell model, when the recrystallization temperature of the lipid is reached, a solid lipid core is generated, and the drug is concentrated in the SLN liquid outer shell by decreasing the dispersion tempreture. Cooling the nanoemulsion in the drug rich core model result in the saturated of the dissolved drug in the molten lipid at saturation solubility. After precipitation of the drug occurs before recrystallization of the lipid, recrystallization of the lipid surrounding the drug occurs because of extreme cooling.
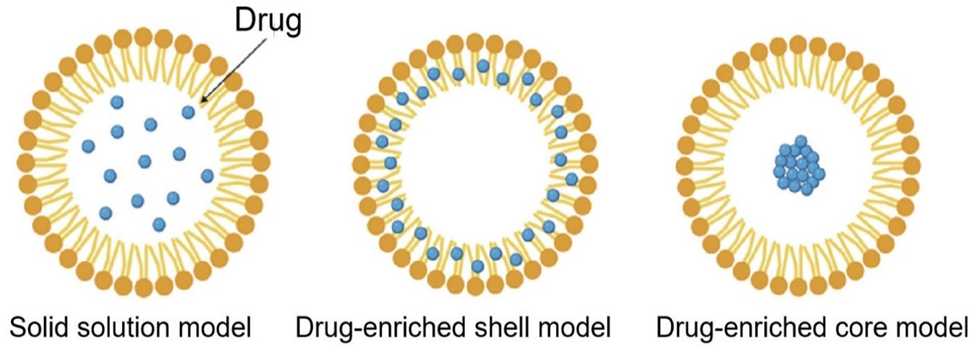
Figure no.5 :- Schematic drug loading model of SLNs
SLNs are suitable for intravenous application by uncomfortable dispersion in solutions to treat various chronic diseases, such as diabetes, obesity, neurodegenerative diseases, and cancer. It has been reported that SLNs can be easily internalized and can be proposed as a surrogate colloidal drug delivery systems for drug administration, especially for malignant melanoma and colorectal cancer, suggesting that SLNs influence antitumour activity. Compared to other nanoparticles SLNs present significant features. SLNs allow for the possibility of scale up production, decreased biotoxicity while enhance bioavailability, and can be used in versatile applications with hydrophilic and lipophilic drugs. Furthermore, engineered SLNs can effectively deliver DNA to the binding sites, resulting in poor transfection efficacy and cytotoxicity. Thus, SLNs cover all sites for drug delivery and can be administered via transdermal penetration, oral absorption, and injection, suggesting that SLNs have potential as carriers of bioactive material. Although SLNs have been introduced as attractive LNPs , there are still some limitations to overcome, such as expulsion and the low loading efficiency of the drug, which has led to the development of the next generation of nanoparticles and nanostructured lipid carriers (NLCs). (NLCs) Facilities high drug solubility, have an increased loading capacity, and increased storage duration. Hence, further studies need to be conducted for optimal lipid Nanoparticles.
Table No .1 :- Advantages and Disadvantage of SLNs
|
SLN type |
Study type |
Advantages |
Disadvantages |
Critical remark |
|
Solid solution model |
In vitro |
Long term drug release capacity |
Drug stability issues under certain conditions |
Efficient when combined with lipophilic drugs |
|
Drug – enriched shell model |
In vitro |
Effective burst release |
Inappropriate for extended release of active pharmaceutical ingredient |
Necessity of controlled burst release |
|
Drug – enriched core model |
In vitro |
Regulated drug release |
Lack of drug loading ability |
Application with highly concentrated drug |
B. SLNs As Drug Delivery Systems :-
To provide more efficient treatment, delivery techniques based on the advantages SLNs have been developed. To overcome the limitation of conventional technological, SLNs have attracted attention because of their unique technological and biological properties. Consequently, SLNs have emerged as feasible nano cariers for drug delivery that complement polymeric nanoparticles. Drug delivery systems encompass formulations, approaches, and technologies for specific purposes. The goal of successful drug delivery is to reduce problem such as side effects, non- specifically, burst or interrupted release, and toxicity. The characteristics. SLNs biodegradability and biocompability, which are based on the nature of the lipid, provide diverse possibilities for administration, and lower the of safety issues.
a. Combination of SLNs With Hydrophilic Compound :-
SLNs can be combined with hydrophilic and hydrophobic drug to stabilize and protect the drug from harsh conditions such as degradation. As the original delivery efficiency of drugs, lipids, and hydrophilic compound is poor, the use of SLNs can offer improved drug delivery mechanism. It can contribute to board applications with drugs of various natures due to the unique benefits of SLNs. Owing the solid lipid matrix, hydrophobic molecules can be encapsulate using appropriate surfactants. Hydrophilic compound interacts insufficiently with lipophilic molecules and divides into aqueous phases, resulting in poor drug delivery and release. To overcome this problem, the double emulsification method is widely used to carry hydrophilic drugs. Hydrophilic drugs liquefy in Water and lipid materials melt in an organic solvent to circumvent drug partitioning. A primary water- in – oil (w/o) emulsion is formed using a dispersed water phase in lipid solvents. A double emulsion, water – oil- water (w/o/w) is obtained when the primary emulsion is emulsified with an aqueous surfactant and the lipid solvents is evaporated. However, there is a possibility of toxicity because of the residue from organic solvent, which can be solved using the melt dispersion techniques in combination with the double emulsion method. Consequently, bioavailability is enhanced via absorption from various sources of the drug.
b. Versatile Administration :-
SLNs based technologies can increase bioavailability, particularly when administered orally. Generally, intravenous injection the main administration routes of chemotherapy. It has the advantage of dose control and cytotoxicity; however, it can cause side effects, such as venous thrombosis and normal cell attack. In contrast , the use of SLNs offers improved bioavailability as well as multi-route administration, particularly via the oral route .Using LNPs, numerous drugcan overcome low oral bioavailability resulting from a lack of absorption. Chemical and enzymatic barrier to drug passage through the gastrointestinal tract make it difficult for some drug to function properly because of poor permeability, instability, and poor water solubility. Nevertheless, the larger surface area of insoluble compound with smaller particle size Improve resistance to extreme condition in the GI tract and increase the efficacy of drug absorption. For instance, the oral bioavailability of simvastatin, which is known to be 5% can be improved with SLNs according to one study. Furthermore, parenteral administration can be enhanced by overcoming the above-mentioned issues. Particularly in anticancer treatment, drug delivery using
SLNs can be favorable for patient in terms of convenience and the potential for self-administration. As such, SLNs provide a wide range of administration routes, including non-parenteral and parenteral routes.
Nanotechnology attenuates toxicity, enable different routes of administration, and control drug delivery and release. It also specific the target tissue, allow large scale production in cost effective ways, and co- delivery of more effective therapeutic strategies. The advantages of SLNs offers pivotal capabilities, especially in drug delivery systems. Thus, enhanced drug delivery systems have been focused on the use of SLNs achieve improved therapeutic effects.
4.4 Nucleic Acid Delivery Systems :-
Since the COVID -19 pandemic, mRNA vaccine have attracted the attention of many researchers. Accordingly , methods to improve the efficacy of gene therapies, such as mRNA and DNA vaccine, which refers to the delivery systems, have followed. Moreover, a codelivery mechanism of SLNs related to small interfering RNA (siRNA) and microRNAs (miRNAs) offers a trailblazing cancer treatment that addresses drug resistance. The advantages of SLNs, including controlled and targeted drug release, reduced side effects, and improved bioavailability, are related to improve nucleic acid delivery. Nucleic acid delivery is key in terms of efficiency and safety.
A. mRNA Vaccine :-
To bind negatively charged nucleic acids, SLNs must be oppositely charged. This charge is determined by both cationic lipid and solid lipid cationic lipid interactions that can cooperate well with cationic lipids and simultaneously retain a solid structure for stability. The electrostatic interaction between SLNs and nucleic acids causes encapsulation of nucleic acids, preventing enzymatic degradation and promoting mobility. Moreover, mRNA is a meaningful non-viral transfection vector because of its unnecessary access to the genome, resulting in a decreased risk of mutation and cancer. mRNA based treatment is considered a promising therapy for several applications, such as vaccines, anticancer treatment, and genome editing. It also renders safer and fast expression, prolonged stability, and higher reproducibility, all of which are beneficial in regards to vaccine production.
mRNA vaccine delivery vehicle is mainly based on LNPs for the successful transportation and protection of mRNA . LNP based mRNA vaccination is currently used by BioNTech/ pfizer and moderna . Furthermore, an in vivo study conducted in TNBC cells presents significant synergistic functions of paclitaxel and p53 mRNA. It implied that nanocariers are considered innovative adjuvants in vaccine delivery systems in terms of encapsulation protection from the host milieu and long term immunostimulation . They are also expected to be useful in anticancer therapy. The entrapment of mRNA with nanocariers includes endosomal escape and cellular uptake, as well as mRNA delivery into immune cells which can promote both innate and adaptive immune responses. Using mRNA with LNPs can deliver encoded cytokines for a reinforced immune response and improved safety by targeting desired cells with less systemic toxicity.
B. DNA Vaccine:-
DNA vaccine has been introduced as prospective methods for inducing both cellular humoral immunological responses. For various diseases, including cancer, DNA vaccine with SLN- induced targeted therapies are based on immune responses. Reducing the side effects of a vaccine, while sustaining its desired effects, is one of the remaining issues that researchers are currently addressing. To maintain transfection longer, the combination of DNA vaccine with SLNs show a noticeable balance between containment and the regulated release of nucleic acids, which is crucial. SLNs act as gene carriers, enhancing the stability and delivery of DNA vaccine, and are able to protect drugs from degradable environments unlike RNA, DNA must pass through the nuclear membrane, requiring different delivery strategies for RNA and DNA . Conjugated with surface ligands, LNPs can easily bind to, and recognize, target cells and enhanced their cellular uptake. Moreover, cationic SLNs interact with negatively charged DNA at higher concentrations in a safer way .LNP formulation have developed thresholds by improving stability, overcoming physiological barriers, and the possibility of targeted therapy, similar to drug. To enhance the benefits SLNs and create more refined therapeutic delivery mechanisms, codelivery of drugs and genes has been developed. The efficacy of antitumour treatment has been improved through the use of SLNs that combine plasmid DNA anticancer drug. Advanced nanodelivery technology offers novel adjuvants benefits for medical platforms. (19,28)
5. SLNs IN BREAST CANCER TREATMENT
The challenges posed by conventional therapies, causing indiscriminate damage to body tissues, have been effectively addressed by the rapid advancements in nanotechnology. This technology provides distinct advantages by enhancing the efficacy of radiation therapy and medication while mitigating side effects. Multifunctional nanocariers leverage the difference between tumour and normal tissues, facilitating the selective transport of therapeutic medications and increasing drug permeability ahe retention. Moreover, the unique physical and chemical characteristics of the tumour microenvironment, including hypoxia , weak acidity, lower PH, unusual temperature gradient, and over expressed protein and enzyme, can be harnessed to control the release rate of pharmaceutical from nano carriers.
Nano material are broadly divided into two main subcategories nanostructured and nanocrystalline Within the classification of nanostructured material, lipid-based nanoparticles, along with both nano polymer and polymers-based nanoparticles, fall under this category. Polymers based nanoparticles encompass Dendrimers, micelles, nanogels , protein nanoparticles, metallic nanoparticles, quantum dots, carbon nanotubes, and nanodiamonds. Lipid based nanoparticles are categorised into two types liposomes and solid lipid Nanoparticles. The Nanoparticles clinically approved for therapeutic purposes predominantly consist of polymers or lipid based components.
In addition to nanostructured particle’s , based on polymers, nanomedicine, or lipids, specific therapeutic application also involve the use of nanocrystalline particles formed through the crystallization of medicine substance.
In the selection of therapeutic nanoparticles, the critical factors to consider include uptake, distribution, release, interaction with cells and molecules, modulation of the immune system, prolonged existence, and overall efficiency. The mechanism mentioned in this section are rootedin the inherent characteristics of nanoparticles. Refer to a visual representation of systemic drug delivery mechanism utilizing novel nanomaterial for breast cancer treatment.

Figure no. 6 :- Nanoparticles Breast Cancer
5.1. pH Responsive NPs :-
The acidic microenvironment induced by intense anaerobic glycolysis is a key characteristics of malignant tumors and therapy resistance. In recent years, this acidic microenvironment has emerged as a novel target for both tumour detection and treatment. This recognition holds significant importance in the progress of pH responsive nanomedicine and nanodiagnostic approaches. A recent study focused on the intracellular delivery of DOC and pH responsive drug release observed 76% of drug release under acidic conditions using bimetallic Prussian blue analogs with cobalt iron and polyethylene glycol methacrylate as an intermediate, AS1411aptamer . The bimetallic Prussian blue analogs and cobalt iron acted as a carrier of doxorubicin. The biocompability of these bimetallic materialwas found to be pH dependent, showcasing excellent survival at a responsive pH . ZnO nanoparticles with pH responsive properties were developed by kundu et al. These nanoparticles with conjugated with phenylboronic acid, enhancing the absorption of drug molecules in tumour tissue through interaction with sialic acid. In acidic environment ZnO undergoes degradation, leading to a higher release of curcumins in tumour cells compared to normal cell. This innovative approach present a targeted treatment for breast cancer, with the goal of minimizing systemic toxicity. The study sheds light on how PBA functionalization precisely targets tumour cells. The anticancer efficacy of curcumins loaded, pH sensitive nanohybrids arises from the unique oxidative stress triggering capabilities of both curcumins and Zn+2 ions. Liu et al. Also developed pH responsive nanohybrids, where they designed a dual pH responsive nanoparticles system to specifically target BC by merging immunotherapy and chemotherapy treatment. While the combination of these treatments shows promise as a potential breakthrough in cancer therapy, a significant challenge lies in simultaneously and accurately targeting both cancerous and immune cells. This inventive system employe poly( L- histidine) and hyaluronic acid, coencapsulating an immune regulator (R848) and chemotherapy drug (doxorubicin) using distinct encapsulation techniques Exploring the acidic pH level within the tumors environment and specific intracellular structure, the nanoparticles system release R848 externally while precisely guiding doxorubicin to breast cancer cell. This strategy opens up possibilities for a synergistc and enhanced therapeutic impact against breast cancer. (29,32)
5.2 Drug Encapsulation And Loading Efficacy
Drug encapsulation efficiency (EE)andloading efficacy/capacity (LE/LC) are key parameters in drug delivery systems, quantifying how much drug is associated with a carrier material.
Encapsulation Efficiency (EE)
Definition: Encapsulation efficiency is the percentage of the initial amount of drug added during the formulation process that is successfully entrapped within or associated with the carrier (e.g., nanoparticles, liposomes).
Purpose: It primarily judges the effectiveness of the encapsulation protocol and helps minimize the loss of the active compound during preparation.
Loading Efficacy
Drug loading efficacy measures the utilization of the drug during the formulation process. It essentially indicates how effective the chosen method is at preventing drug loss (e.g., in the supernatant or external phase).
5.3 Targeted delivery mechanism of breast cancer
A. Passive Drug Targeting:-
Passive drug targeting is widely used for nanomedicine-based delivery system. It uses unmodified NPs, which exploit their surface properties, such as size, shape, charge, and stiffness. Owing to their leaking blood arteries and inadequate lymphatic drainage, tumors are more likely to accumulate minute particles .The enhanced permeability and retention (EPR) can improve the precision of medication delivery to BC Anticancer drugs such as doxorubicin, paclitaxel, and RNA can penetrate tumor cells and increase the potency of non-receptor-dependent medications via passive targeting, such as macro-pinocytosis. Although, this is not the most effective or selective approach, it is frequently used in cancer therapy.
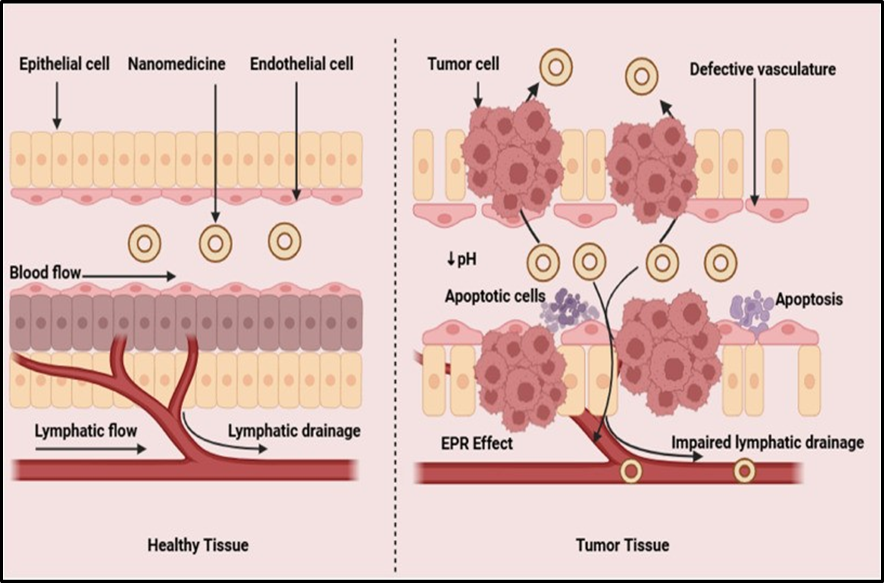
Figure no.7:-Nanomedicine delivery through passive drug targeting
B. Active Drug Targeting:-
Active drug targeting, also known as the second generation of drug targeting, involves loading therapeutic compounds by surface modification and delivery of these compounds to the targeted region. The three primary components of active targeting drugs are ligands, linkers, and cargoes. Numerous therapeutic compounds, including nucleic acids, therapeutic peptides, and small molecule medications are included in the cargo. Moreover, ligands include small molecules, aptamers, targeted peptides, antibodies or antibody fragments, and cells. In contrast, the linker ensures the stability of the peptide drug conjugate during circulation and enhances the efficiency of cytotoxic drugs in killing tumor cells. Targeted therapy delivers monoclonal antibodies and anticancer medications via the receptors. The best delivery to the target tissue must satisfy two criteria: (i) the concentration at tumor site must be greater than normal tissues, and (ii) the concentration must be sufficient for efficient targeting. The overexpression of epidermal growth factor receptors (EGFRs) has been observed in approximately 30 % of solid tumors. Docetaxel (DTX)-loaded immune-based nanoparticles demonstrated reduced toxicity, specifically affecting EGFRs and releasing drugs intracellularly. Similarly, folate receptors (FR), estrogenic receptor-negative, and HER2-negative metastatic progesterone receptor are expressed in 50-85%of patient .the benzoporphyrin derivatives and liposome conjugated with folate have shows MDA-MB-231 cell selectivity. (33,36)
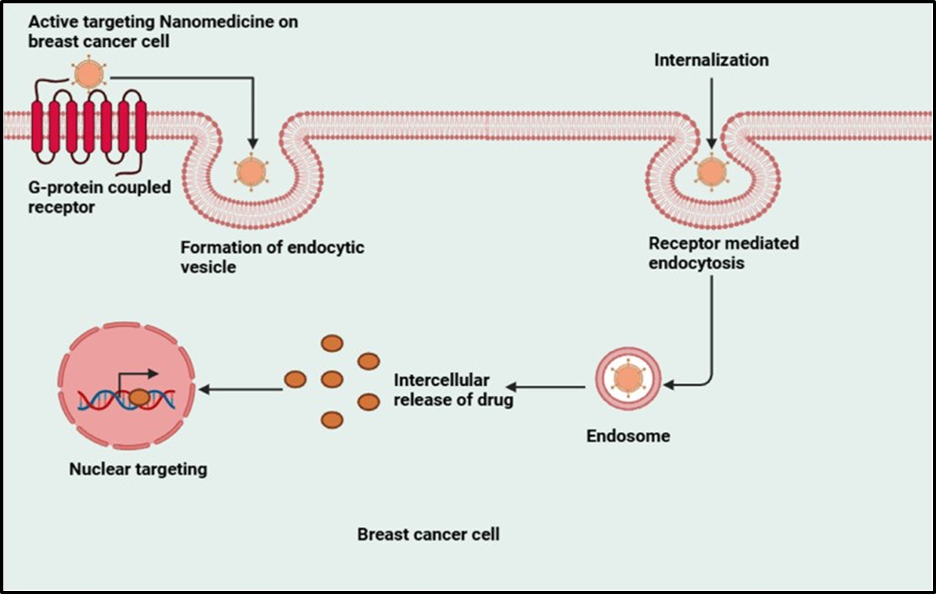
Figure no.8: Nanomedicine delivery through active drug targeting
5.4 Drug Resistance In Breast Cancer:-
A significant number of cancer patients show resistance to treatment.In triple-negative breast cancer, resistance to first-line therapy is particularly high, impeding further treatment efforts. Common breast cancer drugs work through various mechanisms: hormonal treatments like tamoxifen, estradiol, and letrozole modulate hormone activity involved in cell proliferation; monoclonal antibodies such as trastuzumab target HER2-positive cancer; and chemotherapeutic agents like taxanes (e.g., paclitaxel and docetaxel) and anthracyclines (e.g., doxorubicin and daunorubicin) address different aspects of cancer growth. Breast cancer cells can become resistant to chemotherapeutic drugs with different mechanisms.

Figure no.9: Drug resistance mechanism in breast cancer
A. Increased drug efflux :-
A primary problem associated with chemotherapy resistance is decreased net drug accumulation within the cells caused by the upregulation of drug efflux pumps.The ATP-binding cassette (ABC) transporter superfamily is central to the drug efflux in these cells. There are nine ABC genes in seven subfamilies: ABCA, ABCD, ABCE, ABCB, ABCC, ABCF, and ABCG, and three particular ABC transporters, i.e., ABCB1, ABCC1, and ABCG2, have been implicated in MDR. ABCB1, MDR1/P-glycoprotein (P-gp), is expressed in normal tissues but its higher expression in various cancers has been reported. The expression of ABCB1 in breast tumors varies among individuals and has been observed in cancers of the breast, kidneys, colon, adrenals, pancreas, liver, prostate, and ovaries. The overexpression of ABCB1 is associated with chemo-resistance. For instance, when ABCB1 is silenced, its protein expression doubles in drugresistant SKBR3 and MCF-7 breast cancer cells.
Epigenetic regulation affects both the expression and transport of ABCB1. CpG islands in the proximal promoter region of ABCB1 are often hyper-methylated, which may be linked to decreased transcription of ABCB1 and improved overall survival in individuals with ovarian and breast cancer. ABCG2, also known as breast cancer resistance protein (BCRP), contributes to anticancer therapy resistance and is a marker of cancer stem cells (CSCs). ABCG2 is a drug transporter capable of expelling both positively and negatively charged drugs. The overexpression of ABCC1 and ABCG2 is notably documented in triple-negativebreast cancer (TNBC) compared to other breast cancer subtypes.
B. Epigenetic modification :
Epigenetic mechanisms can contribute to chemotherapy drug resistance, including methylation at cytosine-guanine sites, which enhance gene silencing, hypomethylation that upregulates oncogenes, histone modifications, and non-coding RNA alterations..Resistance can also develop against target-directed therapies due to mutations in the causative proteins or epigenetic modifications that may change the proteins' expression levels. The demethylation of an oncogene's promoter region can lead to a pharmacological response by upregulating the gene. Conversely, hyper-methylation of genes related to DNA repair can result in cell cycle arrest. Some miRs, such as miR-21, target the PTEN gene, promoting cancer cell proliferation; miR-10 modulates the PTEN/AKT pathway, indicating positive progression of breast cancer; and miR-27b-3p acts as a tumor suppressor targeting the PPARG gene, which is responsible for promoting TNBC metastasis. The Food and Drug Administration (FDA) has approved epigenetic drugs, such as DNA methylation inhibitors (DNA methyltransferase inhibitors) like AD-738, which is made from azacitidine (decitabine; DAC), and histone deacetylase inhibitors (HDACi), including vorinostat. 5-Azacitidine and entinostat were put together as an epigenetic duo in a phase II clinical test for women with advanced breast cancer. On the other hand, doxorubicin administration to breast cancer tumors was shown to possibly be connected to an increase in the risk of metastasis through an increase of SIPA1 expression that can facilitate the epithelial-mesenchymal transition in cancer cells.(38,41)
6. EXAMPLES OF SLNs FORMULATED FOR BREAST CANCER :-
6.1 Paclitaxel :-
Paclitaxel injection is used to treat advanced cancer of the ovaries, breast, non-small cell lung cancer, and Kaposi sarcoma. Kaposi sarcoma is a cancer of the skin and mucous membranes that is commonly found in patients with acquired immunodeficiency syndrome (AIDS).

Figure no. 10:-Paclitaxel
Mechanism Of Action :-
Stabilizing microtubules and disrupting mitotic spindle formation, paclitaxel specifically targets cancer cells and reduces their ability to proliferate. The pharmacokinetics of paclitaxel involve rapid intravenous (IV) administration, extensive plasma protein binding, hepatic metabolism, and biliary excretion.

Figure no. 11 :- Mechanism of action in Paclitaxel
Side Effects :-
Uses :-
Paclitaxel injection is used to treat advance cancer of the ovaries, breast, non small cell lung cancer and kaposi sarcoma.
6.2 Doxorubicin :-
Doxorubicin is part of the anthracycline group of chemotherapeutic agents. Doxorubicin may be used to treat soft tissue and bone sarcomas and cancers of the breast, ovary, bladder, and thyroid.

Figure no.12:-Doxorubicin
Mechanism Of Action :-
There are two proposed mechanisms by which doxorubicin acts in the cancer cell (i) intercalation into DNA and disruption of topoisomerase-II-mediated DNA repair and (ii) generation of free radicals and their damage to cellular membranes, DNA and proteins.

Figure no.13: Mechanism of action in Doxorubicin
Side Effects :-
Uses :-
Doxorubicin injection is used together with other medicines to treat cancer of the blood, lymph system, bladder, breast, stomach, lungs, ovaries, thyroid, nerves, kidneys, bones, and soft tissues, including muscles and tendons.
6.3 Tamoxifen :-
Tamoxifen is a hormone therapy used to treat hormone receptor-positive breast cancer. It can greatly reduce the risk of cancer recurrence (return) and invasive cancer. Some people take tamoxifen to lower the risk of developing breast cancer.

Figure no.14:- Tamoxifen
Mechanism Of Action :-
Tamoxifen exerts both estrogenic and anti-estrogenic effects depending on the tissue. The drug inhibits tumor growth in breast tissue while acting as an estrogen agonist in bone, which may help prevent osteoporosis in postmenopausal women.
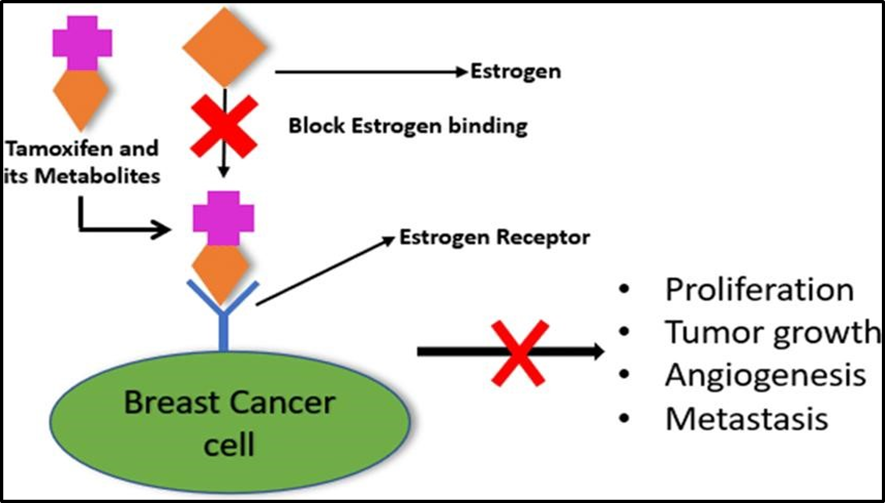
Figure no.15: Mechanism of action in Tamoxifen
Side Effects :-
Uses
Tamoxifen is used to treat breast cancer that has spread to other parts of the body in men and women
6.4 5-Fluorouracil :-
Fluorouracil, sold under the brand name Adrucil among others, is a cytotoxic chemotherapy medication used to treat cancer. By intravenousinjection it is used fortreatment of colorectal cancer, oesophageal cancer, stomach cancer, pancreatic cancer, breast cancer, and cervical cancer.

Figure no.16:- 5- Fluorouracil
Mechanism Of Action :-
In mammalian cells, 5-FU is converted to fluorodeoxyuridine monophosphate (FdUMP), which forms a stable complex with thymidylate synthase (TS), and thus inhibits deoxythymidine mono-phosphate (dTMP) production.

Figure no.17 :- Mechanism of action in 5- Fluorouracil
Side Effects:-
Uses :-
Fluorouracil (5-FU, 5-fluorouracil), sold under the brand name Adrucil among others, is a cytotoxic chemotherapy medication used to treat cancer.
7. FUTURE PROSPECTS FOR BREAST CANCER :-
ADCs are transforming breast cancer (BC) treatment with unprecedented precision. ADCs are expanding the therapeutic potential to HER2-low, ultra-low, and negative BC. ADCs are poised to become a standard of care across various stages of BC. Personalized ADC treatment strategies represent the future of BC therapy.
CONCLUSIONS:-
Mammography, in conjunction with physical examination, is the method of choice for early detection of breast cancer. Other methods should not be substituted for mammographyin diagnosis or screening, but may be useful adjuncts in specific diagnostic situations.
Diagnostic mammography of symptomatic women should always be performed when indicated, utilizing recom-mended equipment and techniques and well-trained, knowledgeable personnel.
Screen-film mammography requires dedicated x-ray units, firm compression, and an x-ray spectrum produced by an appropriate combination of x-ray tube target, tube window,filtration, operating potential, screen-film combination, film processors, technique, and viewing conditions. The CC and MLO views are recommended as the standard views for all types of mammography.
Mammographic equipment should be chosen to provide acceptable image quality at a typical mean glandular dose(for a two-view examination) of 6 mGy, or less for screen-film image receptor with grid for a patient having4.5 cm thick-compressed breasts of 50 percent adipose and50 percent glandular tissue composition.
Image quality and appropriate dose level should be maintained by a QA program conducted by a QA technologist and medical physicist, involving specified periodic measurements and readjustment of all aspects of the imaging and viewing system.
Mean glandular dose should be determined at least annually at each installation for the techniques used at representative breast thicknesses. This dose can be calculated from data supplied in this Report by measuring beam quality andin-air exposure at the entrance surface of the breast.
A quality administration program (medical audit) should be used to compare the facility’s clinical outcomes with established guidelines.
Annual mammographic screening examinations appear to provide favorable benefit/risk ratios in terms of breast cancer mortality in women age 50 or above, if acceptable image quality and dose are maintained.
Results of randomized clinical trials of screening mammography for women age 40 to 49, for which 10 or more years of follow-up is available, have shown evidence of a substantial benefit in reducing mortality which exceeds any risk of radiation-induced breast cancer.
REFERENCES


Vaishnavi Biradar, Ahankari Shripad, Fabrication of Solid Lipid Nanoparticle Formulation for Breast Cancer Management, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3571-3593. https://doi.org/10.5281/zenodo.18724407
 10.5281/zenodo.18724407
10.5281/zenodo.18724407
