Department Of Pharmaceutics, St. Joseph’s College of Pharmacy, Cherthala, Alappuzha 688524
Solid lipid nanoparticles (SLNs) are advanced colloidal drug carriers consisting of a biocompatible lipid core stabilized with surfactants, developed to enhance drug stability, skin penetration, and controlled release in topical applications. Compared to traditional dosage forms, SLNs offer benefits such as improved bioavailability, protection of unstable drugs, minimized systemic side effects, and compatibility with both hydrophilic and lipophilic agents. They have been extensively explored for managing infectious, inflammatory, and cosmetic skin disorders, as well as in cosmeceutical formulations. Various preparation strategies, including high-pressure homogenization, solvent emulsification, and microemulsion methods, have been established, each presenting unique strengths and limitations. However, issues like restricted drug loading and possible drug leakage during storage remain. Recent progress in nanostructured lipid carriers (NLCs) and hybrid systems helps overcome these drawbacks by providing better stability and drug incorporation. Looking ahead, combining SLNs with innovative approaches such as microneedle delivery, intelligent wound dressings, and sustainable large-scale manufacturing techniques could further broaden their utility. In summary, SLNs hold great promise as next-generation platforms for topical and transdermal drug delivery, with broad pharmaceutical and cosmeceutical potential.
Solid lipid nanoparticles (SLNs) are innovative colloidal delivery systems composed of a biocompatible lipid core surrounded by an amphiphilic surfactant shell, with particle sizes typically ranging from 50 to 1,000 nm. They serve as promising alternatives to conventional colloidal carriers such as emulsions, liposomes, and polymeric micro- or nanoparticles. First introduced in the 1980s by Speiser and colleagues for drug delivery, SLNs are aqueous colloidal dispersions whose matrix is made of solid biodegradable lipids. Replacing liquid oils with solid lipids provides a major advantage for controlled drug release, since drug mobility within a solid matrix is significantly lower than in liquid oils. Solid lipids, already used in pellet formulations for sustained drug release in oral delivery, further support this concept. Unlike conventional dosage forms, colloidal carriers like SLNs offer superior performance due to their nanoscale dimensions and ability to control drug release. This not only protects the drug but also allows administration through both parenteral and non-parenteral routes, highlighting the versatility of SLNs as a drug delivery system.
Different classes of solid lipid nanoparticles (SLNs) are commercially available, each defining the formulation characteristics and corresponding drug release profile. SLNs combine the advantages of both conventional and novel drug delivery systems while overcoming many drawbacks of traditional carriers. Key benefits include controlled drug release, enhanced bioavailability, protection of unstable molecules such as retinol and peptides from degradation, cost-effective excipients, higher drug incorporation, and broad applicability. Despite these merits, SLNs face limitations such as restricted drug loading and possible drug expulsion during storage. These challenges are addressed by the next generation carriers, known as nanostructured lipid carriers (NLCs), which possess a tailored nanostructure that increases drug loading capacity and ensures stable drug incorporation over time. Thanks to their size-dependent properties, lipid nanoparticles open new opportunities in therapeutic development. With their distinct advantages, both SLNs and NLCs hold great promise for topical, oral, and parenteral delivery of pharmaceutical and cosmetic agents. Among these, cosmeceuticals are emerging as the leading area of application. Importantly, carrier systems like SLNs and NLCs have been designed to align with industrial requirements such as scalability, standardization, validation, simple processing, and cost-effectiveness.
STRUCTURE OF SOLID LIPID NANOPARTICLE
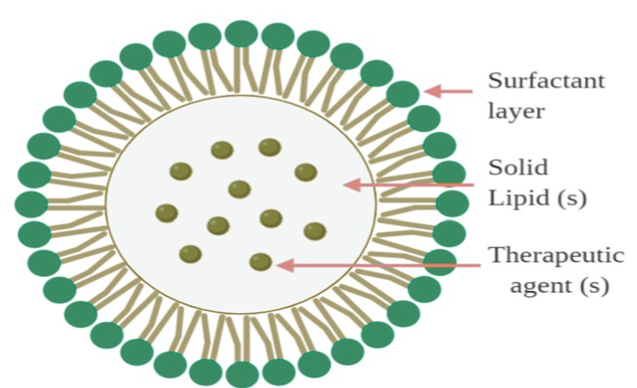
COMPONENTS OF SOLID LIPID NANOPARTICLE
Solid lipid nanoparticles (SLNs) are spherical carriers composed of a solid lipid matrix that encapsulates drug molecules, surrounded by a surfactant layer to maintain stability in aqueous media. The primary distinction between SLNs and nanostructured lipid carriers (NLCs) lies in their lipid composition: SLNs are formulated solely from solid lipids, whereas NLCs incorporate a blend of solid and liquid lipids. Upon preparation, SLN matrices typically exist in α and β′ polymorphic forms, which are high-energy states. Over time, these rearrange into the more stable β form, leading to reduced space within the matrix and possible drug expulsion during storage. This limitation arises because SLNs consist of similar lipid molecules with limited accommodation capacity. In contrast, NLCs are composed of mixed lipid molecules, forming imperfect or amorphous matrices that provide greater capacity for stable drug incorporation.
The essential components for SLN preparation include solid lipids, liquid lipids (oils), and emulsifiers. The lipids commonly employed are generally recognized as safe and approved by both American and European regulatory authorities for clinical use. Drug solubility in different lipid types is often assessed to identify the most suitable lipid for maximum drug loading. Emulsifiers are equally critical for nanoparticle stabilization. In SLNs, the majority are hydrophilic surfactants such as polysorbate 80 (Tween 80), lecithin, poloxamer 407, poloxamer 188 (Pluronic F68), phosphatidylcholine, PEG-40 castor oil (Cremophor® RH40), sodium deoxycholate, and sodium dodecyl sulphate. The choice and concentration of emulsifier are optimized through screening, with typical usage levels ranging between 0.1% and 5% (w/v).
PRINCIPLE OF DRUG RELEASE FROM SOLID LIPID NANOPARTICLE
There are 3 drug incorporation models which describe drug release from SLN

COMPOSITION OF SOLID LIPID NANOPARTICLE
LIPIDS:
Lipids are the fundamental constituents of lipid nanoparticles and greatly influence their drug loading potential, stability, and sustained release properties.
SELECTION OF CRITERIA FOR LIPIDS:
The primary considerations when selecting a lipid carrier are its drug-loading capacity and the intended therapeutic purpose. Lipids that form highly crystalline particles with a perfect lattice often lead to drug expulsion. In contrast, complex lipids containing fatty acids of varying chain lengths create imperfect crystalline structures with more voids, allowing greater drug entrapment.
ROLE OF AN CO EMULSIFIER:
Because phospholipid molecules have limited mobility, a sudden deficiency of emulsifier on the particle surface can result in aggregation and increased particle size of SLNs. To counter this, co-emulsifiers are incorporated to maintain stability and prevent particle growth.
CLINICAL APPLICATION OF LIPID NANOSYSTEMS FOR SKIN DELIVERY
The prevalence and types of skin disorders are largely shaped by infectious diseases and environmental factors. Commonly observed conditions within communities include infections, eczema, dermatitis, pigmentation disorders, and acne [246]. Effective treatment requires not only the right therapeutic approach but also a suitable carrier system for drug delivery. Applying medications topically at the affected site helps limit systemic exposure and lowers the risk of adverse effects [139]. Both topical and transdermal drug delivery offer significant benefits, including improved patient compliance, bypassing hepatic first-pass metabolism, and enabling self-administration.
TOPICAL DRUG DELIVERY OF SOLID LIPID NANOPARTICLES
INFECTIOUS DISEASES
Both superficial and deep skin infections caused by bacteria, fungi, and viruses contribute to a wide range of dermatological conditions. Common bacterial infections include cellulitis, impetigo, and erysipelas, most often linked to Group A streptococci and Staphylococcus aureus, with the former responsible for a significant proportion of cases. Superficial fungal infections are typically caused by dermatophytes, Candida, and Malassezia species, while viral skin infections are frequently associated with herpes simplex virus.
Some bacterial infections are particularly difficult to manage due to factors such as intracellular persistence, involvement of deeper skin layers, and the emergence of antimicrobial-resistant strains. These challenges highlight the need for innovative treatment strategies, including the use of broad-spectrum bactericidal agents incorporated into specialized delivery systems designed to improve skin and cellular penetration.
Fungal infections affecting the epidermis and dermis are generally treated with oral or topical antifungal agents. However, oral therapy often leads to side effects and drug interactions, while conventional topical treatments suffer from poor skin retention and rising resistance. These limitations have driven the development of nanostructured drug delivery systems as alternative therapeutic approaches.
Incorporating antimicrobial agents into lipid-based nanosystems has demonstrated controlled release, improved penetration, and enhanced therapeutic efficacy. Such systems are particularly advantageous in maintaining effective drug concentrations for extended periods, thereby reducing the risk of resistance development.
INFLAMMATORY DISEASES
Psoriasis and atopic dermatitis are among the most prevalent inflammatory skin disorders. Psoriasis typically presents as red, sharply bordered plaques covered with thick silvery scales, whereas atopic dermatitis is recognized by dry, itchy, eczematous lesions. The presence of microbes or chemical agents in the skin can activate different T-cell subgroups in the immune system. Under normal conditions, this activation triggers inflammatory responses that either defend against or regulate chemical and microbial threats. However, in autoimmune-related inflammatory skin diseases, Th1 and Th2 cells generate inappropriate immune responses against the body’s own tissues. In allergic reactions, such as allergic contact dermatitis, Th2-driven inflammation occurs after exposure to environmental or chemical allergens. Both autoimmune skin diseases and dermatitis are marked by a deficiency of regulatory T cells, which normally suppress immune overactivity, prevent autoimmunity, and reduce inflammation.
Genetic, hormonal, and environmental influences often underlie these inflammatory processes. Skin disorders arise when the skin’s defence mechanisms are overwhelmed, leading to an excess of proinflammatory mediators and reactive oxygen species (ROS). To counteract this, therapies involving immunomodulators and antioxidants are commonly employed. Topical administration of anti-inflammatory drugs is particularly advantageous, as it achieves high local drug concentrations while minimizing systemic side effects compared to oral or injectable routes. Agents such as glucocorticoids, retinoids, nonsteroidal anti-inflammatory drugs (NSAIDs), and COX-2 inhibitors are widely used. When incorporated into lipid nanosystems, these drugs demonstrate improved skin penetration, targeted delivery to deeper skin layers, and an overall enhanced therapeutic profile.
Psoriasis, in particular, has a strong genetic basis and is characterized by abnormal keratinocyte proliferation and differentiation. Treatment using psoralens in combination with long-wavelength ultraviolet radiation (PUVA) has shown effectiveness by slowing keratinocyte replication and achieving significant lesion clearance. However, the hyperproliferative skin in psoriasis often restricts psoralen penetration, making solid lipid nanoparticles (SLNs) especially beneficial for delivering lipophilic psoralens.
Corticosteroids remain a cornerstone therapy due to their strong anti-inflammatory and antiproliferative properties. Their potency ranges from mild to super-potent, and selection depends on the severity and location of lesions. For example, mild to moderate corticosteroids are preferred for acute lesions on sensitive areas such as the face and intertriginous regions, while potent corticosteroids are recommended for thickened, chronic lesions on the palms and soles. Despite their efficacy, corticosteroids are associated with side effects including skin atrophy, masking of infections, tachyphylaxis, and pigmentation changes.
NSAIDs are also widely applied topically for inflammatory and painful skin conditions. Owing to their analgesic, antipyretic, and anti-inflammatory properties, they are commonly used in managing diseases such as osteoarthritis and rheumatoid arthritis. For chronic conditions, controlled-release delivery systems are especially important as they maintain effective drug levels over extended periods, helping to relieve pain and inflammation, slow disease progression, and minimize adverse effects.
ANTI AGING AND COSMETICS
Cosmetic formulations are primarily developed to nourish the skin while serving aesthetic and personal hygiene purposes. In certain cases, disruptions in skin function caused by systemic conditions—such as vitamin deficiencies or endocrine disorders—necessitate cosmetic products containing pharmacologically active agents.
Lipid-based nano systems have been reported to provide protective benefits to the skin through mechanisms such as occlusion, adhesion, and lubrication. Their nanoscale size allows them to form a thin monolayer film on the skin surface, which reduces moisture loss through evaporation due to their hydrophobic character. This hydration effect improves skin elasticity, making them particularly suitable for anti-aging applications. Additionally, their lubricating and mechanical properties may lessen the urge to scratch, helping to prevent skin damage linked to irritation and allergic reactions. Beyond their functional role, the appearance and elegance of cosmetic products are also important; solid lipid nanoparticles (SLNs) enhance this aspect owing to their pearl-like sheen, submicron size, and protective lipid-based composition.
Compared with conventional formulations, lipid nano systems demonstrate enhanced drug penetration, sustained release, reduced degradation of active ingredients, and improved therapeutic performance. Their occlusive, hydrating, and adhesive properties further support their use as effective cosmetic bases. Moreover, their appealing pearl-like appearance and fine particle size contribute to product elegance, which can enhance patient satisfaction and compliance.
PREPARATION OF SOLID LIPID NANOPARTICLES
SOLVENT EMULSIFICATION EVAPOURATION METHOD
This method is carried out in two steps: first, preparing an oil-in-water nano emulsion, and second, evaporating the solvent. To begin with, the drug and lipids are dissolved in a suitable organic solvent or a mixture of solvents, which forms the oil phase. This is then emulsified into an aqueous phase. Typical solvents used are water-immiscible organics such as dichloromethane, chloroform, cyclohexane, and toluene. After the nano emulsion is formed, the solvent is removed—commonly by rotary evaporation or mechanical stirring. As evaporation progresses, the lipid concentration in the droplets increases, leading to lipid precipitation and the production of solid lipid nanoparticles (SLNs).
Because the process employs toxic organic solvents, additional steps are needed to eliminate residual solvent and to evaluate formulation safety through in vitro and in vivo testing. The SLNs obtained are usually dispersed in large volumes of water, so concentration by ultrafiltration or evaporation is often required. Nevertheless, this method is particularly suitable for thermo-labile drugs since it avoids the high temperatures and mechanical forces associated with high-pressure homogenization or high-speed stirring. The SLNs produced generally display a narrow particle size distribution with an average diameter of about 100 nm.
SOLVENT EMULSIFICATION DIFFUSION METHOD
This technique involves four key steps: (i) mutual saturation of water and an organic solvent, (ii) formation of an oil-in-water Nano emulsion, (iii) dilution with water, and (iv) removal of the solvent. Initially, water and the chosen organic solvent are saturated with each other to establish thermodynamic equilibrium between the two phases. Partially water-miscible solvents such as benzyl alcohol, butyl lactate, methyl acetate, ethyl acetate, and isopropyl acetate are commonly used. In the next step, the drug and lipids are dissolved in the organic solvent, after which emulsification with the aqueous phase generates an oil-in-water emulsion. This emulsion is then diluted 5–10 times with water, which facilitates diffusion of the solvent into the aqueous phase, causing lipid precipitation and the subsequent formation of solid lipid nanoparticles (SLNs). Finally, the solvent is removed, usually by lyophilization or vacuum drying.
A major limitation of this approach is the use of organic solvents, which necessitates further purification to eliminate solvent residues. In addition, the dilution step produces a dispersion with high water content and a relatively low SLN concentration. Despite these drawbacks, the method is scalable and, like the solvent emulsification–evaporation technique, offers the advantage of avoiding high temperatures and mechanical stress, making it suitable for thermo-sensitive drugs.
SOLVENT INJECTION METHOD
The solvent injection method, first applied for SLN preparation in 2003, consists of three steps: (i) preparation of the aqueous and oil phases, (ii) injection of the solvent, and (iii) solvent removal. In this process, the oil phase is obtained by dissolving the lipid and drug in a water-miscible solvent such as ethanol, methanol, isopropanol, acetone, or a mixture of these solvents. The aqueous phase is prepared as a water-based solution containing an emulsifier or a combination of emulsifiers. During the second step, the organic solution is drawn into a syringe and rapidly injected into the aqueous phase under constant stirring. This leads to the immediate formation of oil droplets at the injection site. As the solvent diffuses, lipid concentration within the droplets increases, resulting in the formation of solid lipid nanoparticles (SLNs), which are stabilized by the emulsifier. The final step involves eliminating the solvent. Variations of this method include the use of micro-channels with cross-shaped junctions and co-flowing micro-channel systems to improve efficiency and control.
HIGH PRESSURE HOMOGENIZATION METHOD
High-pressure homogenization (HPH) is widely used to reduce the size of droplets and solid particles under extreme pressure. This technique offers several advantages, including being free of organic solvents, requiring relatively short processing times, and being feasible for large-scale production. HPH is generally categorized into two types: hot and cold homogenization.
Hot HPH involves three main steps: (i) preparation of a coarse emulsion, (ii) high-pressure homogenization, and (iii) cooling. First, the drug and lipids are melted at a temperature 5–10 °C above the lipid’s melting point, while the aqueous emulsifier solution is preheated to the same temperature. The two phases are then mixed to form a hot coarse emulsion. Next, the emulsion undergoes homogenization at the same temperature using a high-pressure homogenizer (500–1500 bar for 3–5 cycles). During this process, the mixture is forced through a narrow gap at extremely high velocity (~1000 km/h), creating intense shear and cavitation forces that reduce droplet size. Finally, the Nano emulsion is cooled, resulting in the formation of solid lipid nanoparticles (SLNs).
Cold HPH consists of two steps: (i) preparation of lipid microparticles and (ii) high-pressure homogenization at low temperature. In the first step, the drug and lipids are melted and blended to form a uniform drug-lipid mixture, which is then rapidly cooled with liquid nitrogen or dry ice and ground (e.g., using a mortar or ball mill) to obtain lipid microparticles of ~50–100 μm. These microparticles are dispersed in a cold aqueous surfactant solution and subjected to homogenization at 0–4 °C for 5–10 cycles at ~500 bar. This approach is especially suitable for hydrophilic drugs, as it minimizes drug loss during processing. Strategies such as adjusting the pH of the aqueous phase (for drugs with pH-dependent solubility) or preparing drug–lipid conjugates have also been applied to further reduce drug loss. However, limitations of cold HPH include larger particle sizes and more labour-intensive processing.
HIGH SPEED STIRRING AND ULTRA SONICATION METHODS
High-speed stirring, also called high-shear homogenization, is a simple and cost-effective technique for producing solid lipid nanoparticles (SLNs). The process involves three steps: (i) preparation of aqueous and lipid phases, (ii) homogenization, and (iii) cooling. First, the drug and lipids are dispersed uniformly at a temperature 5–10 °C above the lipid’s melting point, while the aqueous surfactant solution is prepared at the same temperature. Next, the two phases are blended using a high-shear mixer, generating a hot oil-in-water emulsion. Finally, cooling the emulsion results in SLN formation. Often, this method is combined with ultrasonication after homogenization to further decrease droplet size.
This approach offers advantages such as solvent-free processing and operational simplicity. However, it has drawbacks, including the need for high surfactant concentrations, exposure of drugs to elevated temperatures, and potential metal contamination from the sonicator probe.
MICRO EMULSION METHOD
The microemulsion method consists of two main steps: (i) preparation of a microemulsion and (ii) dilution. In the first step, drugs and lipids are melted and mixed at a temperature above the lipid’s melting point. A preheated aqueous surfactant solution is then slowly added under gentle stirring to form a microemulsion. In the second step, this hot microemulsion is poured into a cold aqueous solution while stirring, which induces lipid precipitation and results in SLN formation.
This method is attractive because it is simple, reproducible, solvent-free, and easily scalable. However, it requires large amounts of surfactants and water, creating the need for an additional water-removal step.
PHASE INVERSION TEMPERATURE (PIT) METHOD
The PIT method utilizes non-ionic polyoxyethylated surfactants, whose properties change with temperature. At lower temperatures, the ethoxy groups are strongly hydrated, giving the surfactants a high hydrophilic-lipophilic balance (HLB). As the temperature rises, these groups become dehydrated, reducing the HLB value and increasing the surfactant’s lipophilicity. The phase inversion temperature (PIT) is the point at which the surfactant shows equal affinity for both aqueous and lipid phases.
This method consists of three steps: (i) heating, (ii) cooling, and (iii) lipid precipitation. First, drugs, lipids, water, and surfactant are heated above the PIT, resulting in a water-in-oil emulsion. Next, rapid cooling converts this emulsion into an oil-in-water nano emulsion. The heating–cooling cycle can be repeated several times (e.g., between 60 °C and 90 °C) to enhance uniformity. Finally, further cooling of the nano emulsion induces lipid precipitation, leading to the formation of SLNs.
The PIT method is advantageous because it is solvent-free and requires minimal energy. However, the resulting nano emulsions tend to have low stability.
MEMBRANE CONTACTOR METHOD
This technique makes use of a specialized membrane contactor and involves two main steps: (i) formation of a hot nano emulsion and (ii) cooling. In the first step, drugs and lipids are heated above the melting point of solid lipids and then forced through the pores of a membrane at the same temperature, generating fine lipid droplets. On the opposite side of the membrane, an aqueous surfactant solution flows tangentially across the surface, carrying the lipid droplets away and forming a hot nano emulsion. In the second step, the nano emulsion is cooled to solidify the droplets, resulting in the formation of SLNs.
The membrane contactor method offers advantages such as scalability and precise control over particle size. However, it also has drawbacks, including the need for advanced equipment and the risk of membrane clogging. This approach has been successfully applied to prepare vitamin E–loaded SLNs.
COACERVATION METHOD
The coacervation technique involves three stages: (i) preparation of a micellar solution, (ii) addition of a coacervating agent, and (iii) cooling. In this method, alkaline salts of fatty acids, such as sodium behenate and sodium stearate, are used as lipid materials. Initially, lipids and drugs are dispersed in an aqueous solution containing a polymeric stabilizer and heated until a clear micellar solution of lipid salts is obtained. In the second stage, a coacervating solution is gradually added dropwise, leading to lipid precipitation. Finally, the suspension is cooled to ensure complete precipitation of the lipids.
OTHER METHODS
DOUBLE EMUSION METHOD
The double emulsion technique can be performed either with or without organic solvents and involves three main steps: (i) formation of a water/oil emulsion, (ii) development of a water/oil/water double emulsion, and (iii) lipid precipitation. In the first stage, an aqueous solution containing drugs and stabilizers is emulsified in a water-immiscible organic phase containing lipids, or alternatively in solvent-free molten lipids, to form a water/oil emulsion. This emulsion is then dispersed in an aqueous phase to generate a water/oil/water double emulsion. In the final stage, the double emulsion is cooled to allow SLN formation; if organic solvents are used, they are subsequently evaporated. This method is particularly effective for encapsulating hydrophilic drugs and biomolecules into SLNs.
SUPERCRITICAL-FLUID-BASED METHODS
Supercritical fluids, such as supercritical CO?, are also applied in SLN preparation. In the supercritical-assisted injection method, supercritical CO? is combined with an organic phase before being injected into an aqueous phase, where lipids rapidly precipitate to form SLNs. Alternatively, the organic phase–CO? mixture can be expanded through a nozzle, resulting in SLN formation. Another approach is the supercritical fluid extraction of emulsion method, where an oil/water emulsion and supercritical CO? are introduced into an extraction column from opposite directions. Here, the supercritical CO? efficiently extracts the solvent from the oil phase, leading to SLN formation.
CHARACTERIZATION OF SOLID LIPID NANOPARTICLE
PARTICLE SIZE AND DISTRIBUTION
2. ELECTRICAL SURFACE POTENTIAL AND pH
3. SHAPE AND SURFACE MORPHOLOGY
4. CRYSTANILLITY
5. SURFACE HYDROPHOBICITY
6. DENSITY
7. VISCOSITY
8. MOLECULAR WEIGHT
9. IN VITRO RELEASE STUDIES
FUTURE PERSPECTIVE
Solid lipid nanoparticles (SLNs) have demonstrated immense potential as novel carriers for topical drug delivery owing to their ability to enhance drug penetration, improve stability, and provide controlled release. Despite these advantages, certain challenges such as limited drug loading, drug expulsion during storage, and scale-up difficulties still hinder their wide clinical translation. Future research will likely focus on the design of next-generation lipid carriers, such as nanostructured lipid carriers (NLCs), lipid–polymer hybrids, and stimuli-responsive systems, which can overcome these limitations and ensure better stability and drug incorporation. With the growing emphasis on personalized medicine, SLNs may be tailored for patient-specific needs by incorporating targeting ligands, peptides, or antibodies to achieve site-specific delivery in dermatological disorders. Furthermore, integration with advanced technologies such as microneedle patches, smart wound dressings, and 3D-printed scaffolds is expected to revolutionize their role in chronic wound management and skin regeneration. On the manufacturing front, the development of green, solvent-free, and scalable methods such as supercritical fluid technology and membrane contactor systems will be vital for sustainable large-scale production. Importantly, clinical translation of SLN-based formulations will require rigorous long-term safety evaluations, standardized characterization protocols, and addressing of regulatory concerns. Beyond dermatology, SLNs are also expected to expand into cosmeceuticals, transdermal vaccination, pain management, and delivery of biomolecules such as peptides, proteins, and nucleic acids. Overall, with continued innovation in formulation design, production technologies, and clinical validation, SLNs are poised to become a mainstream platform for next-generation topical and transdermal therapies.
CONCLUSION
Solid lipid nanoparticles represent a promising and versatile carrier system for topical drug delivery, offering advantages such as improved drug stability, enhanced skin penetration, controlled release, and reduced systemic side effects. Their ability to incorporate both hydrophilic and lipophilic drugs makes them suitable for treating a wide range of dermatological conditions, from infections and inflammatory disorders to cosmetic and anti-aging applications. Although certain limitations such as limited drug loading capacity and potential drug expulsion during storage still exist, advances in nanostructured lipid carriers and hybrid systems are addressing these challenges. With continued research into eco-friendly production methods, targeted delivery strategies, and clinical validation, SLNs hold great potential to bridge the gap between conventional dosage forms and next-generation nanomedicine, ultimately improving therapeutic outcomes and patient compliance in topical and transdermal drug delivery.
REFERENCES


Arya Ashok, Praveen Raj R., Riya Marium Philip, Solid Lipid Nanoparticle for Topical Drug Delivery, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 178-191. https://doi.org/10.5281/zenodo.17036562
 10.5281/zenodo.17036562
10.5281/zenodo.17036562
