Caritas College of Pharmacy, Ettumanoor, Kottayam, Kerala
Peptic ulcer disease results from erosion of the gastrointestinal mucosa due to an imbalance between protective factors and aggressive agents such as gastric acid and pepsin. This study evaluated the anti-ulcer potential of Spondias pinnata leaves extracted using ethanol by maceration. The extract (ESP) was assessed through in vitro methods, including acid neutralisation capacity (ANC) and H?/K?-ATPase inhibition. The ESP exhibited significant concentration-dependent anti-ulcer activity, showing ANC values of 15.87 ± 0.09 at 50 mg (p< 0.001)and 20.17 ± 0.09 at 200 mg compared with the standard (P< 0.001) (AH MH, 500 mg). The percentage inhibition of H+K+ ATPase activity increased from 22.50 ± 1.00 at 50 mg to 72.47 ± 0.09 at 200 mg when compared with omeprazole. Maximum activity was observed at 200 mg, indicating a positive dose-response relationship, though the standard drug remained more potent. These findings suggest that Spondias pinnata possesses promising anti-ulcer activity and may serve as a potential plant-based alternative to conventional anti-ulcer agents. Further isolation and characterisation of active constituents are required to elucidate the mechanism of action.
The World Health Organisation (WHO) defines Peptic Ulcer Disease (PUD) as an erosion or ulcer in the lining of the gastrointestinal tract, primarily the stomach or duodenum, caused by the corrosive action of gastric acid or pepsin on the damaged mucosal layer. Peptic ulcer disease (PUD) refers to the breakdown of the mucosal lining in the upper gastrointestinal tract due to the corrosive action of gastric acid and pepsin. [1] Peptic ulcers develop when there is an imbalance between the stomach’s protective mechanisms, such as mucus and bicarbonate secretion, sufficient blood flow, prostaglandin E2, nitric oxide, sulfhydryl compounds, and antioxidant enzymes, and harmful elements like acid and pepsin. This chronic condition is also associated with environmental and lifestyle factors, including Helicobacter pylori infection, alcohol intake, smoking, unhealthy diet, and prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs). [2,3]Peptic ulcers are generally categorised into 2 types: gastric (stomach) ulcers and duodenal ulcers. Gastric ulcers primarily affect elderly individuals and are usually located along the lesser curvature of the stomach.[4] Duodenal ulcers are 4 times more common than gastric ulcers. A common symptom of a duodenal ulcer is epigastric pain that typically occurs before meals or at night, and this pain is often relieved by eating or drinking milk.[5]Peptic ulcer disease remains a significant global health problem, affecting a substantial proportion of the population worldwide. Ulcers affect approximately 10% of the global population, with gastric ulcers accounting for about 5% of this. Moreover, peptic ulcers are more common in males than in females.[6] The lifetime prevalence of peptic ulcer disease is estimated to be between 5 and 10%, with an incidence rate of 0.1 to 0.3% [7]. Epidemiological studies have established that the prevalence of PU is a reflection of Helicobacter pylori (H. pylori) infection and increases with the use of non-steroidal anti-inflammatory drugs (NSAIDs), aspirin (ASA), and ageing. Until the late 20th century, peptic ulcer disease (PUD) caused significant morbidity and mortality, but its incidence declined due to environmental changes and improved hygiene, which reduced childhood H. pylori infections, especially in developed countries [8]. Peptic ulcers may remain asymptomatic in many individuals, and in some cases, the initial clinical presentation is a serious complication such as gastrointestinal haemorrhage. At present, the most frequent clinical manifestation of peptic ulcer disease is epigastric pain. [6]Additional clinical features include nausea, vomiting, anorexia, unintended weight loss, and signs of gastrointestinal bleeding such as hematemesis and melena.[8,12]
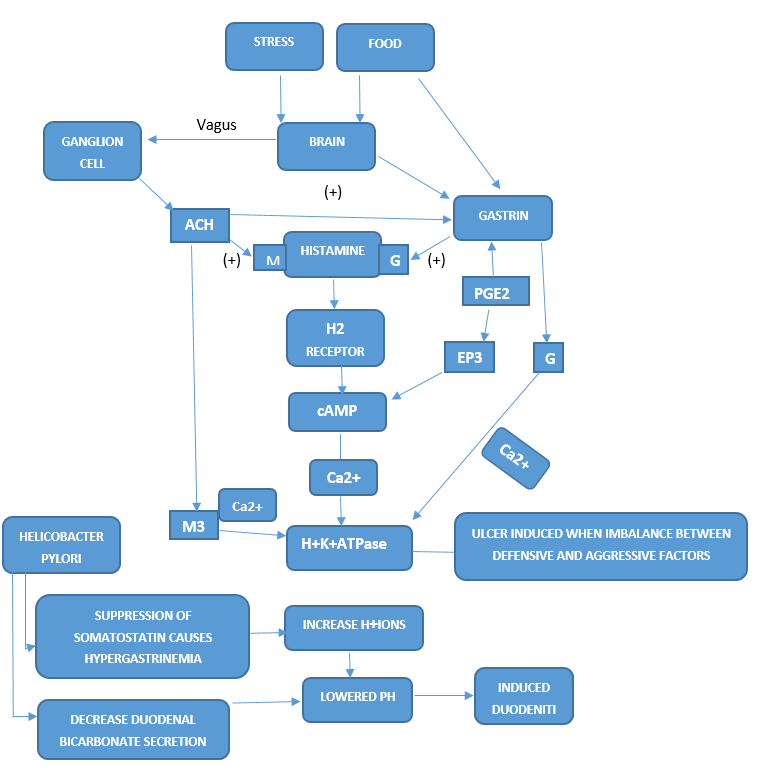
Figure 1: Pathogenesis of ulcer [10, 12]
Management of the condition involves both pharmacological therapy and eradication of Helicobacter pylori infection.[13] Medical treatment includes the use of H2-receptor antagonists such as cimetidine and ranitidine, or proton pump inhibitors (PPIs) including omeprazole and lansoprazole.[11,13] Additional therapeutic options include prostaglandin analogues like misoprostol and antacids such as Maalox and Mylanta. Eradication of H. pylori is a key component of treatment and is commonly achieved through triple therapy. This regimen consists of a proton pump inhibitor (omeprazole or lansoprazole) combined with clarithromycin and either amoxicillin or metronidazole, administered for 14 days. Following this course, PPI therapy is continued for an additional 4–6 weeks. Shorter treatment regimens lasting 7–10 days are less effective. Alternatively, quadruple therapy may be employed, particularly in resistant cases. This regimen includes bismuth subsalicylate, tetracycline, metronidazole, and a proton pump Inhibitor such as omeprazole or lansoprazole, and is administered for a duration of two weeks. [14]
Plant-derived natural products are being used more frequently in medicine due to their low toxicity and minimal side effects. According to the WHO, 65-68% of people across the world use herbal products derived from plants, which help them to maintain good health and prevent illness [15,16]. Spondias pinnata shows various pharmacological properties like antihyperglycemic, anti-cancerous, anti-inflammatory, antioxidant, antimicrobial, hepatoprotective, etc. [17 ]
Ayurveda, the oldest medicinal system in the world, provides leads to find therapeutically useful compounds from plants. Therefore, Ayurvedic knowledge supported by modern medicine is necessary to isolate, characterise, and standardise the active constituents from the herbal source. This combination of traditional and modern knowledge can produce better antiulcer drugs with fewer side effects.[18] Synthetic drugs such as proton pump inhibitors, H2 receptors, cytoprotectants, demulcents, anticholinergics, antacids and prostaglandin analogues are used for the treatment of ulceration, but these drugs produce several side effects. For example, PP inhibitors may cause nausea, abdominal pain, constipation, diarrhoea, and H2 receptor antagonists may cause gynecomastia and loss of libido[19,20]. Due to the occurrence of many side effects from the use of synthetic drugs for many diseases, medicinal plants are considered the main source of new drugs, as they have fewer side effects. As herbal drugs are considered safe for the treatment of ulcers with fewer side effects, economical, effective, and relatively less toxic, extensive research is carried out in search of potential antiulcer agents of plant origin. Herbs are widely available in India and other countries. The wide spectrum makes them an attractive candidate for further research.[21,22]
Table 1: List of herbal plants with anti-ulcer activity
|
Sl.No |
Medicinal Plant |
Family |
Phytoconstituent |
Plant Part & Solvent |
Animal Used For Preclinical Study |
Refernce |
|
1 |
Aloe Vera |
Liliaceae |
Barbaloin ,isobarbaloin,, Alo- Emodin, aloesin, flavonoids, anthraquinone glycoside, tannins, saponins. |
Leaf |
Rats |
Widyastiwi et al; [23] |
|
2 |
Amala
|
Phyllantaceae |
Alkaloids, saponins, flavonoids, tannins, steroids carbohydrate |
Fruit, ethanolic extract |
Rats |
M.Madhavi Kumari et al; [24] |
|
3 |
Cassia fistula |
Leguminosa |
Flavonoids,sapnins, alkaloids, tannins, glycosides, terpenoids |
Leaf, ethanolic extract |
Rats |
S Karthikeyan et al; [25] |
|
4 |
Mentha |
Lamiceae |
Phenolic compounds, Carbohydrate, alkaloid, flavonoid, tannins |
Leaf alcoholic extract |
(in vitro) |
G. Kalyani et al; [26] |
|
5 |
Henna |
Lythraceae |
Tannins, flavonoids, alkaloids, saponins, lawsone |
Leaf Chloroform extract |
Rats |
Goswami M et al; [27] |
|
6 |
Custard apple |
Annonaceae |
Tannins, flavonoid saponins, phenolic compounds, carbohydrate |
Leaf Ethanolic extract |
Rats |
Palanisamy A et al; [28] |
|
7 |
Guava |
Myrtaceae |
Alkaloids, tannins, flavonoids, phenolic compounds, saponins |
Leaf Hydroalcoholic extract |
Rats |
Rameshwari K et al; [29] |
|
8 |
Tulsi |
Lamiaceae |
Flavonoids, terpenoids, essential oils, and phenolic compounds. |
Leaf Aqueous and ethanolic extract |
Rats |
Mohapatra Bharat et al; [30] |
|
9 |
Neem |
Meliaceae |
Alkaloids, flavonoids, carbohydrates, Terpenoids, Tannins, Saponins |
Aqueous leaf extract |
Rats |
Ndi Sirri Akwen [31,32] |
|
10 |
Morinda citrifolia |
Rubiaceae |
Terpenoids, alkaloids, glycosides, flavonoids, phenols |
ethyl acetate extract of the fruit |
Rats |
P. Muralidharan [33] |
|
11 |
Black seed |
Ranunculaceae |
Saponins, Tannins, Flavonoids, Alkaloids, Glycosides, Steroids |
Aqueous seed extract & oil |
Rats |
Nwafor, O.I [34] |
|
12 |
Thani |
Combretaceae |
Saponins, tannins, flavonoids, alkaloids, Terpenoids, Steroids |
methanolic extract of the leaf |
Rats |
Taslima Begum [35] |
|
13 |
Bael |
Rutaceae |
Alkaloids, flavonoids, Terpenoids, tannins, and phenolic acids, |
Leaf Aqueous extract |
Rats |
J. ILAVARASAN. R [36] |
Spondias pinnata (L.f.) Kurz belongs to the Kingdom Plantae, Subkingdom Tracheobionta, Superdivision Spermatophyta, Subclass Rosids, Order Sapindales, and Family Anacardiaceae. It is a deciduous ornamental tree attaining a height of approximately 12–18 m, characterised by an upright growth habit, soft-wooded stem, and a well-developed deep tap root system. Commonly known as Indian hog plum or wild mango, S. pinnata is native to the Malesian region and is widely distributed throughout India, Nepal, Bhutan, southern China, and Myanmar. Indigenous groups have traditionally used the plant's edible fruits, which can be eaten raw or pickled, for ethnomedical purposes. The bark is traditionally used in Ayurveda medicine to treat diabetes mellitus, muscular rheumatism, and dysentery. In Nepal's mountainous regions, bark juice is used to cure rheumatic illnesses, diarrhoea, and stomachaches. The latex is administered topically to heal wounds in far-western Nepal, while the blossoms are used as a flavouring in Illam, Nepal. Fruit pulp is applied to wounds and sores, leaves, stems, and bark are used to cure diarrhoea and dysentery, and bark is used to treat gonorrhoea. Pharmacological research has shown that the fruit extract has antidiabetic and antilipidemic properties in addition to the bark's hypoglycemic efficacy. Additionally, leaf extracts have strong antioxidant and free-radical-scavenging capability due to their high phenolic content and antibacterial and antiviral properties.
2. MATERIALS AND METHODS
2.1 Collection of Spondias pinnata
Fresh leaves of Spondias pinnata were collected from local areas of Ettumanoor, Kottayam district, and authenticated by Dr Vargheese M.C (HOD Botany department), Devamatha College, Kuravilangad. The collected plant parts were sorted to remove any undesirable material or plant sections. They were shade-dried for three weeks and powdered to a coarse form.
2.2 Extraction of Spondias pinnata
The extraction process of Spondias pinnata was done by maceration. Macerate the dry powder of the plant in 400ml 80% ethanol at room temperature for 2 days, and the filtrate was collected, concentrated and dried the filtrate using a heating mantle. The percentage yield was calculated for the plant extract by using the formula
Percentage yield = (Weight in grams of extract obtained / Weight in grams of plant material taken) x 100 [43]
2.3 In vitro anti-ulcer screening methods
2.3.1Acid Neutralisation Method
Take 2 mL of the ethanolic extract of Spondias pinnata at four different concentrations (50, 100, 150, and 200 mg/mL), make up the volume to 50 mL with sufficient water and mix for 2 minutes, then add 30 mL of 1 N HCl to the test solution; prepare the standard solution in the same manner using aluminium hydroxide and magnesium hydroxide (100 mg), stir each mixture for 15 minutes, add a few drops of phenolphthalein and mix gently, and finally titrate the excess HCl with 0.5 N NaOH added drop wise until a persistent light pink colour appears.[44,45]
Acid neutralising capacity (ANC) per gram of antacid = (Vol. of HCl ×Normality of HCl) - (Vol. Of NaOH × Normality of NaOH) [46]
2.3.2 H+K+ATPase Inhibition Method
Fresh sheep stomach was obtained from a slaughterhouse, the fundus region was opened and the mucosa removed, the inner layer was scraped to collect parietal cells, which were homogenized in 16 mM Tris buffer (pH 7.4) containing 10% Triton X-100, centrifuged at 6000 g for 10 minutes, and the supernatant was collected as the enzyme preparation for H?/K?-ATPase.The H?/K?-ATPase inhibition assay was carried out by incubating 0.1 mL of enzyme extract with plant extract (50, 100, 150, and 200 mg/mL) at 37 °C for 60 minutes, initiating the reaction with 2 mM ATP, 2 mM MgCl?, and 10 mM KCl (200 µL each), further incubating for 30 minutes at 37 °C, stopping the reaction with 4.5% ammonium molybdate and 60% perchloric acid, and centrifuging the mixture at 2000 g for 10 minutes. From the centrifuged mixture, 1 mL of supernatant was collected and mixed with 4 mL of Millipore water, 1 mL of 2.5% ammonium molybdate, and 0.4 mL of ANSA reagent, allowed to stand for 10 minutes at room temperature, the absorbance was measured at 660 nm, and enzyme activity was expressed as µmol of inorganic phosphate released per hour at different extract doses and compared with the standard drug omeprazole. [48, 49]
Absorbance of standard - absorbance of test sample
Percentage inhibition = ---------------------------------------------------------------- × 100 [47, 50]
Absorbance of standard
3. RESULTS
Percentage Yield of the Plant Extracts
The Spondias pinnata leaves were extracted by the simple maceration method, and the percentage yield of extract was found to be 11.66% w/w.
|
Part used |
Method of extraction |
Solvent |
|
|
Spondias pinnata |
Leaf |
Maceration |
Ethanol |
Percentage yield = 6.4955.66×100

Evaluation of Anti-ulcer activity by the acid neutralisation method
Anti-ulcer activity of Spondias pinnata was evaluated by measuring the Acid Neutralization Capacity (ANC) of the plant extract. (Table.)
Table: Acid Neutralisation Capacity of the Spondias pinnata leaf extract
|
Sl.no |
Concentration |
ANC |
|
1 |
500mg (Standard) |
|
|
2 |
50mg (Extract) |
15.87 ± 0.09*** |
|
3 |
100mg (Extract) |
17.87± 0.09*** |
|
4 |
150mg (Extract) |
19.60 ± 0.06*** |
|
5 |
200mg (Extract) |
20.17 ± 0.09*** |
All the values are in Mean±SEM. *P<0.05, **P<0.01, ***P<0.001 when compared to control.
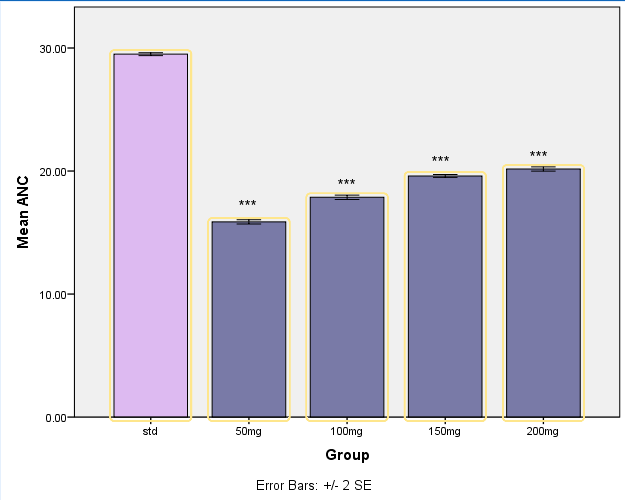
Figure 2: Evaluation of Spondias pinnata using ANC
The test samples used in this method is 50,100,150 and 200 mg/ml of the ethanolic extracts of Spondias pinnata, and aluminium hydroxide and magnesium hydroxide (500mg) are used as a standard drug. The standard drug in the concentration of 500mg/ml shows significant anti-ulcer activity when compared to the test samples with 29.50 ±0.12 as ANC (P<0.001)
One-way ANOVA demonstrated a significant difference in ANC among the experimental groups. Dunnett’s post-hoc analysis was used to compare each treatment dose with the standard control. Evaluation of Anti-ulcer activity by the H+K+ATPase inhibition method
Evaluation of anti-ulcer activity of Spondias pinnata leaf extract using H+K+ATPase inhibition in-vitro technique by measuring the percentage inhibition.
|
Concentration |
% inhibition (Standard) |
%inhibition (extract) |
|
50mg |
59.12 ± 0.76 |
22.50 ± 1.00 |
|
100mg |
68.90 ± 0.89 |
62.32 + 0.25 |
|
150mg |
74.47 ±0.71 |
68.14 ± 0.32 |
|
200mg |
79.35 ± 0.66 |
72.47 ± 0.09 |
All the values are in Mean±SEM. *P<0.05, **P<0.01, ***P<0.001 when compared to control.
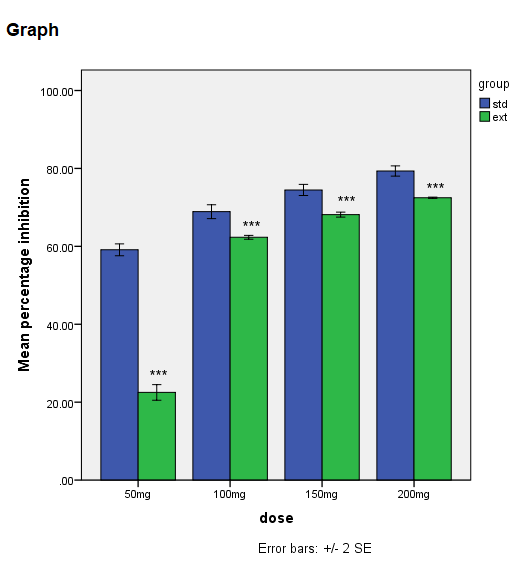
Figure 11: Evaluation of Spondias pinnata using H+K+ATPase inhibition method
The percentage inhibition produced by the standard and the extract at different dose levels (50, 100, 150, and 200 mg) was analysed using one-way analysis of variance (ANOVA) in SPSS. Comparisons were performed dose-wise, i.e., standard versus extract at the same dose level. Results are expressed as mean ± standard deviation (SD). At 50 mg, one-way ANOVA revealed a statistically significant difference in percentage inhibition between the standard and the extract (p < 0.001). The standard exhibited a significantly higher inhibitory effect compared to the extract at this dose. Similarly, at 100 mg, a significant difference was observed between the standard and the extract (p < 0.01), indicating that the inhibitory activity of the standard remained significantly greater than that of the extract. At 150 mg, the analysis demonstrated a statistically significant difference between the two groups (p < 0.05). Although the extract showed increased inhibition compared to lower doses, its effect was still significantly lower than that of the standard. At the highest dose tested, 200 mg, one-way ANOVA again indicated a highly significant difference between the standard and the extract (p < 0.001). Both treatments exhibited increased inhibition; however, the standard consistently produced greater inhibition than the extract. Overall, the statistical analysis confirmed that the percentage inhibition differed significantly between the standard and extract at all tested dose levels.
4. DISCUSSION
The main objective of the present study is to evaluate the anti-ulcer activity of the leaf extract of Spondias pinnata using in-vitro screening technique, such as determination of acid neutralisation capacity and H+K+ATPase inhibition method. This study evaluated the impact of escalating treatment doses on ANC in comparison with a standard control group. Statistical analysis revealed a highly significant decrease in ANC across all treated groups. Notably, a substantial reduction was evident even at the lowest dose of 50 mg, indicating a strong treatment effect. Although ANC levels showed a dose-dependent increase at higher concentrations, they remained significantly lower than those observed in the standard group. These results suggest that the treatment markedly influences neutrophil levels, possibly by affecting neutrophil production or survival. Further investigations are required to clarify the underlying mechanisms responsible for this effect.One-way ANOVA demonstrated that the standard exhibited significantly greater inhibitory activity than the extract at all evaluated doses (50–200 mg). The extract exhibited inhibition at 50 mg, 100 and 150 mg, and showed a dose-dependent increase in inhibitory action; nevertheless, efficacy was still much lower than the standard. Both treatments reached maximum inhibition at 200 mg, indicating a positive dose-response relationship, while the standard remained more potent. Overall, the dose-dependent increase in inhibition observed with the extract suggests the presence of bioactive constituents, although their effectiveness may be limited by lower concentration or reduced bioavailability compared with the standard.
CONCLUSION
The pharmacological evaluation of Spondias pinnata leaf extract demonstrated significant gastroprotective and antiulcerogenic activity, supporting its potential as an effective herbal remedy in the management of peptic ulcer disease. The plant exhibits antiulcer activity due to major constituents including carbohydrates, alkaloids, flavonoids, phenols, tannins, and terpenoids. But flavonoids act as the major constituent responsible for antiulcer activity. The leaves were extracted by a simple maceration process using ethanol as the solvent. The antiulcer activity was evaluated by the acid neutralisation method and the H+K+ATPase inhibition method. On the basis of statistical analysis, we may conclude that the leaf extract of Spondias pinnata may possess an antiulcer property. However, further studies are required to establish its exact mode of action.
REFERENCES

Fatima Mehrin, Avani Santhosh, Vrinda R, Rynu Tom Thykkaden, Evaluation Of In Vitro Anti-Ulcer Activity of Spondias Pinnata Leaf Extract, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2859-2869. https://doi.org/10.5281/zenodo.18683579
 10.5281/zenodo.18683579
10.5281/zenodo.18683579
