Amity university Lucknow campus, Uttar Pradesh 226010.
A major global health concern, Helicobacter pylori (H. pylori) infections are linked to a number of gastrointestinal disorders, including gastric cancer and peptic ulcer disease. Higher eradication failure rates have resulted from treatment strategies becoming more complex due to the growing prevalence of antibiotic resistance in H. pylori. The mechanisms of drug resistance in H. pylori are examined in this review, including biofilm formation, horizontal gene transfer, efflux pumps, and chromosomal mutations. Additionally, new approaches to treating resistance are explored, including customized therapy, drug delivery based on nanotechnology, and alternative treatment modalities. Combining targeted therapies with molecular diagnostics has the potential to enhance treatment results and reduce the emergence of resistance. Research, monitoring, and the creation of novel treatment approaches are all necessary to combat H. pylori resistance.
Peptic ulcer disease (PUD) is a worldwide issue with a 5- to 10% lifetime risk of developing. The incidence rate of PUD gets reduced globally (around 51%) as a result of improved sanitary and hygienic practices as well as the adoption of effective therapeutic methods and the judicious use of non- steroidal anti- inflammatory medication (NSAIDs). Consequently, the prevalence, hospital admission, and death rate associated with peptic ulcers have decreased, according to epidemiological studies; however, the case death rate has stabilized at 5-10%[1] The gastrointestinal tracts (GI) mucosal lining gets damaged or ruptured in PUD which causes excessive amount of gastric acid or the pepsin to be secreted. theses symptoms usually occur in the close section of the duodenum and the stomach area [1]. PUD can be caused by many different factors. In those suffering from peptic disease, mucosal disruption may be to a high level of acid secreted in addition to nutrients or anxiety. the use of nonsteroidal anti- inflammatory drugs (NSAIDs) and an infection with H. pylori are the primary risk factors for gastric or peptic ulcers [1] Approximately half of the population of this country suffers with helicobacter pylori (H. pylori) which is the roots of the most common and determined pathogenic bacteria in the world. It is thought that the H. pylori cause stomach cancer, gastritis, peptic ulcer disease and functional dyspepsia [1-3] The first successful isolation of h. pylori to the intestinal biospsies of patient aith choronic antral gastric ulcers occurred in 1983(Isaacson and Wright, 1983). H. pylori is a spiral shaped 2-4 m long, 0.5-1 m wide microaerophilic, gram-negative bacteria [19]. H. pylori employ a variety of methods to infect the gastric mucosa and suffer in the strong gastric environment. these approaches include 1] leaving the acidic stomach lumen 2] adhering to the stomach epithelial cells 3] buffering the pH in the vicinity 4] developing biofilm 5] changing into a stress- resistance morphology (coccoid) which is possible but impossible to cultivate state and 6] bypassing the immune system of the host [20,21]. Additionally, the development of carcinogenesis is linked to H. pylori toxins like vacuolating cytotoxin (VaCA) and the cytotoxin – associated gene A (CagA). the most prevalence characteristics of H. pylori linked to gastric infection
Routes of H.pylori infection
It is essential for gaining a deeper understanding of the pathways of transmission of infection with H.pylori with the goal for enhanced the protection of people against infection . there are three methods that H.pylori may infect people.
1 Individual to individual routes
2 Routes from animals to humans
3 Routes for food and water
Person to person contact may outcome in the spread of H.pylori , particularly in families where mother -child transmission is common (Yang et al., 2023) .Research has demonstrated that H. pylori infections can happen in families in cluster.
Human-to-animal transmission is considered to be a significant pathway for H.pylori infection. An organism called H.pylori can infect both people and animals. (Duan et al., 2023). Additionally evidence suggesting that milk and sheep milk may act as a vector for H.pylori infection in humans is provided by detection of the bacteria in milk, meat (beef, mutton) and other fresh foods (Hemmatinezhad et al., 2016; Shaaban et al., 2023)
3 . Routes for food and water
Finally research indicates the food and water based infection H.pylori infection .H. pylori feces can contaminate lake, river and ground water , all of which are crucial origins of drinking water therefore its probable that absorbing water is how people obtained H.pylori
Pathogenesis of Helicobacter pylori
Three distinct stages of the h. pylori pathogenesis can be studied the attachment with and colonization in the gastrointestinal tract, the induction and envasion of the hosts immune response, and the eventual establishment of the disease.[19]
1 Dispersal and route of infection
H.pylori infections are typically acquired during childhood and frequently asymptomatic .however , about 30% of infected individual may exhibit symptoms of digestive disorders, including moderate- to- sever gastritis, peptic ulcer, and even stomach cancer. MALT lymphoma because H. pylori infections occur within a limited host range, horizontal as well as vertical transmission are common mode of transmission. The four main routes of H.pylori infection are the fecal-oral, gastric oral, oral-oral, and gastric routes, which can happen through ingesting of contaminated food, water, or during endoscopic procedures, even through the precise way of transmission remain unidentified.[20]
2.2.1 Attachment and colonization
The cellular process coordinating H.pylori infection has been advanced method essential for the bacteria beneficial the development in the stomach mucosa ,at the top during disease. Starting in h. pylori attachment and colonization strategies. The bacterial cells chemotaxis to the target site, that is mediated be a specific receptor available on the host cells- mostly members of the Tlp family [22] – is what is initially initiates the pathogens colonization. these receptors have been shown to be activated by an abundance of the chemical signals, such as urea, lactic acid, ROS species, and gastric juice, which facilitates chemical reaction epithelium[22]. Flagellar motility enables H.pylori to get around via the mucus the layer as well as come to stomach epithelium , contributing towards its capacity to strongly hold to while expand the mucosa [23]. Additionally, H.pylori can form biofilms, structured bacterial communities embedded in an exterior matrix, developing dedication and delivering defence towards the host defence’s and treatment therapies [24].
2.2.2 Production of virulence factor
This bacterium’s the causes depends upon a number of virulence factors, such as those that contribute in motility, adhesion, urease, and the production of cytotoxins [26].
2.2.3. CagA and VacA
Enhances patient compliance by lowering the frequency of dosing their smaller size and spherical shape allow them to be added into the body. after attaching itself, h. pylori interact with the host in a complex way by using a variety of virulence factors to control host cell signalling. the primary coordinator of these is the pathogenicity island known as CagA (cytotoxin associated gene A) [27], if CagA is injected into host cells through the type 4 secretion system (T4SS), it sets if a series of events that impair cellular processes and aid in the emergence of gastric pathologies [28]. Numerous pathways of cell signalling are activated as a result of the tyrosine phosphorylation of CagA [29]. This involves the phosphatidylinositol 3-Kinase (PI3K) mitogen activated protein kinase (MAPK) pathways being abnormally activated [30,31]. These pathways are dysregulated, which leads to alterations, in cellular morphology, loss of cell polarity, and the start of carcinogenic process. A defining characteristic of the pathogenesis caused by H. pylori is this cellular taking control of host cell signalling [32]. Another important virulence factor that has different impact on the host cells in the vacuolating toxin VacA[32]. As its name implies VacA forms and compromises the functioning of the gastric epithelial barrier. Channels or pores that cause the cell membrane to become more permeable [26]. In the VacA alters the apoptotic pathways in host cells, resulting in pro – and antiapoptotic impact that vary based on the type of cell and related circumstances. Additionally, VacA toxin influences the structure and function of the host cells by aiding in the establishment of vacuoles with them [34]. Additionally, this toxin thwarts and subverts immune Reponses by influencing T cell and other unaffected cell function.
Urease production and survival at low PH
Approximately 15% of all the proteins in the bacterium are made up of urease, one of the most frequently expressed proteins by the pathogen [42]. One of H. pylori distinguishing characteristics is the urease production, which is frequently utilized in the identification of additionally the infection [43]. Additionally, H. pylori demonstrate chemotactic activity towards specific chemoattractant, like urea and carbonates, which draw the bacterial cells to the areas of the stomach lining that have a greater pH. The family of H. pylori chemical receptors play a critical role in the desired chemotactic activity that encourages survival in an acidic stress environment [50].
Immune system modulation and induction of inflammatory responses
The hosts immune system and bacterial factors interact dynamically to produce an immune reaction to an infection with H.pylori [51] . The development of H. pylori infections is caused by an immune system response that is complicated and multifaceted [52]. H. pylori cause chronic inflammation in the stomach mucosa during the innate immune phase. This response is mediated by lipids and the peptidoglycan component of the cell wall and is characterized by the recruitment of immune cells, neutrophils, macrophages, lymphocytes, and pro- inflammatory cytokines (like interleukin -1beta, interleukin- 6, and tumour – necrosis factor -alpha) as well as the release of neutrophils, macrophages and lymphocytes [53,54]. Via pattern recognition receptors like toll-like receptors, innate immune activation triggered by bacterial components such as lipopolysaccharides and peptidoglycan intensify the inflammatory cascade [55]. This prepares the body for the immune systems adaptive response, in which CD4+T-helper cells are essential for fostering a Th1 response that secretes interferon -gamma. while B Cells create antibodies against H. pylori, regulatory cells are enlisted and help suppress the immune system [56,57].
Modulation of mucin production
The protective mucous layer in the stomach mucosa is impacted by H. pylori influence on mucin production. The mucins carbohydrate components function as a ligand to facilitate the bacterium’s attachment to the stomach mucosal lining [63]. The microorganism can change the production of the mucin genes and directly affected mucins such as MUC5A and MUC1. Causing mucin turnover to be blocked or hampered [64]. The modifications to mucin production have an impact on the mucosal glycocalyx’s composition, which influences adherence. And H.pylori colonization Additionally , this regulation of mucin synthesis helps to the capacity of the bacteria to overcome the hosts defences and causes enduring infections [65]. In the continuous efforts to manage the related diseases, understanding the subtleties of immune system control in infection by H.pylori is essential for developing treatments and preventive measures . The intricacies of this host – pathogen interaction are still being discovered by the ongoings research.
How it develops resistance in resistance H. pylori
There are multiples ways that the organism helicobacter pylori have become resistance to antibiotics, but mutation in genes and horizontal transfer of genes are the main culprit, essentially H. pylori develop antibiotic resistance in the following ways
An overwhelming amount of research suggest that chromosomal changes [1]. have been the primary cause for H. pylori immunity to antibiotics. this mutation happens in particular genes linked to obstruction to various classes of antibiotics.
In H. pylori, small changes in those genes are a highly prevalence mechanism of resistance [1][2]. Resistance is conferred by the mutations lower capacity to bind antibiotics to their targets.
Transfer of antibiotics resistance may arise about genetic provides among district strains of H. pylori [1], through these are less frequent, studies conducted in vitro have demonstrated resistance genes can spread through transformation. [1]
Multidrug resistance (MDR) may occur compare to H. pylori efflux pump system triggering because they force antimicrobial agents out of the bacterial cells [5]. Gene mutation and efflux pump combine to increase resistance.
Because it can create biofilm, H. pylori is shielded from its hosts immune system and antibiotics [4], In addition to acting as a physical barrier, bio films cause bacteria to go dormant, which reduces their susceptibility to antibiotics. Chromosome mutation, horizontal transfer of genes, pumps for efflux, and biofilm creation have all performed together to give H, pylori resistance to the vast majority of first- line antibiotics used to eradicate the infection.[3][4]. To counter this growing g threat ongoing surveillance along with studies into novel treatment approaches are essential.
Resistance strains
Clarithromycin resistance
Globally clarithromycin resistance is a major concern, According to recent studies , resistance rates have gone up in a number of nations, including Australia ,Talwan , Belgium , Bulgaria , Italy , and Iran, for example, a study found that rates of antibiotics resistance ranged from 25% to 36% across different parts of Europe , and that resistance has been steadily rising over time, conversely[1][3] , stable resistance rates under 15% have been demonstrated in nations like France , Spain, and Russian .[1]. The bacterium Helicobacter pylori (H, pylori), which is well known for its involvement in gastrointestinal disorders, is the main cause of clarithromycin Aresistance. usually, the 23S ribosomal RNA gene has the particular mutations confer this resistance, specially at positions A2142G, A2142C, and A2143G theses mutations significantly decrease the binding efficacy of clarithromycin, which results in treatment failures.[1]
Specific bacteria and species
Bacteria name; Helicobacter pylori
Species; the primary species exhibiting clarithromycin resistance is helicobacter pylori
Common mutation associated with clarithromycin Resistance
Despite being less frequent, theses mutations might nevertheless be involved in resistance mechanism.[1][2][3]
Mechanism of resistance
The primary mechanism that these mutations confer resistance is via modification to the ribosomes RNAs clarithromycin binding site, The 23S rRNA peptidyl transferase region binds to clarithromycin, preventing the synthesis of new protein change in these areas cause the antibiotic binding affinity to be obstructed, which permitted H, pylori to persist in spite of these presence. [2][4]
Metronidazole Resistance
Different regions demonstrate varying trends in metronidazole resistance. According to specific research, resistance levels in some populations- most especially those in Latin American and some parts of Asia – have reached 93.2%.[2] [3]. On the conjunction, resistance rates have decreased in other areas, emphasizing the need for specific monitoring to inform treatment choices.[3] one of the problems with treating infections brought on by different bacterial species is metronidazole resistance. An extensive summary of particular bacteria linked to metronidazole resistance along with an explanation of the resistance mechanisms, is provided below.
Specific bacteria associated with metronidazole resistance
Prevalence of resistance; A study carried out in Bangladesh found that 72.7% of the clinical isolates of H, pylori [4] were resistance of metronidazole, according to another study, about 40% of H, pylori strains were resistant to metronidazole, which made treatment plans more difficult and required the use of combination regimens or other antibiotics [5].
Mechanism of resistance
Plasmid- mediated resistance; C. difficile’s metronidazole resistance has been linked to the pCD-METRO plasmid, which confers resistance by means of genes that facilitate drug inactivation.[1] The fact that this plasmid has been found in both toxic and non-toxic strains emphasizes its significance in the emergence of resistance to therapy.
Clinical cases; A patient’s development of metronidazole- resistant strains during treatment was documented in a case study. Underscoring the resistances therapeutic consequences.[1]
Mechanism of resistance
Nim genes; The primary cause of Bacteroides fragilis metronidazole resistance among anaerobic bacteria is the presence of nim genes (e.g, nimA to nimK). The nitroimidazole reductases encoded by these genes have a capacity to inactivate metronidazole, resulting in various levels of resistance [2]. concerns concerning the effectiveness for treatment for infections brought on by this organism are raised by the rising frequency of resistance strains.
Mechanism of resistance
Because these species produce nitroeductase, which convert metronidazole into inactive compounds, they show metronidazole resistance. The drugs antibacterial properties suffer by this metabolic alteration.[2] This resistance mechanism has been demonstrated in isolates from patients receiving repeated metronidazole treatments, suggesting a clinical connection between exposure to antibiotics and the appearance of resistance strains.
Levofloxacin resistance
Levofloxacin resistance has also been observed to be rising, especially in Asia and Europe, where resistance rates have been found to be as high as 20% in certain studies,[1][2]. given the dependence on fluoroquinolones as second – line treatments for the eradication of H. pylori, this increase is cause for concern over levofloxacin resistance in the management of different bacterial infections is growing. An extensive summary of particular bacteria linked to levofloxacin resistance is provided below, along with the data on their mechanism, frequency.
Specific bacteria associate with levofloxacin resistance
Mechanism of resistance
Mutation in gyrA and gyrB genes; The main cause of resistance in H. Pylori is believed to be mutations in the gyrA gene, which produces a subunit of DNA gyrase, a Fluroquinone target. Specific mutations that have been strongly linked to levofloxacin resistance include N87K and D91N. [2] Additionally, there has been a strong correlation demonstrated between resistance and mutation in the gyrB gene, specifically at locus A343V. [2]
Prevalence of resistance; levofloxacin resistance rates among H. pylori isolates were found to be roughly 36% in some regions, according to a study [2]. Another study from Bangladesh found a significant correlation between levofloxacin resistance and mutations in gyrA underscoring the importance of susceptibility testing prior to starting treatment [2].
Mechanism of resistance;
levofloxacin resistance in E. coli is frequently linked to mutation in the gyrA and parC genes. In particular, gyrA mutation at codon 83 and 87 are frequent [5]. Reduced susceptibility may also result from the existence of plasmid- medicated quinolone resistance (PMQR) genes, such as qnrS, which shield target enzyme from fluoroquninolone action.[5]
Prevalence of resistance; Depending on the region and local antibiotic usage patterns, studies have shown that clinical strains of E. coli have varied rates of levofloxacin resistance, ranging from 10 % to over 50%.[5]
Mechanism of resistance; Klebsiella pneumoniae, like E, coli, primarily demonstrates levofloxacin resistance due to mutations in the gyrA in the gene. It has been determined that ser83Leu and Asp87Gly mutations are important causes of resistance [1]. Treatment options may become more complex when extended- spectrum beta-lactamases (ESBLs) are present.
Prevalence of resistance; levofloxacin resistance rates in pneumonia have been reported to exceed 40% especially in infections linked to healthcare facilities.[1]
Mechanism of resistance; Levofloxacin resistance in pseudomonas aeruginosa is frequently caused by mutations in the gyrA, gyrB, and parC genes. These genes can be mutated to change DNA gyrase and topoisomerase 4, two important targets of fluoroquinolones [6]. Moreover, efflux pumps are important in lowering drug concentration inside cells.
Prevalence of resistance; it has been estimated that 30% of patients have pseudomonas aeruginosa strains that are resistance to levofloxacin; patients who have chronic infection tend to have higher prevalence rates.[6]
Mechanism of resistance; levofloxacin resistance in Enterobacteriaceae is associated with particular mutation in the gyrA genes quinolone resistance -determining regions (QRDR). for example, mutations like Asp87Asn and Ser83Tyr have been linked to higher resistance levels [1] by shielding target enzymes, PMQR genes like qnr can also promote higher-level resistance.
Prevalence of resistance; According to a study, the percentage of clinical isolates of Enterobacteriaceae that were resist to levofloxacin varied greatly, with some regions reporting as high as 50%.[1]
Multidrug resistance
Concern over the rise in resistance to drugs H. pylori strains is growing, Numerous studies have stated cases of triple resistance to Levofloxacin, metronidazole, and clarithromycin as well as dual resistance to these three drugs, certain populations rates of triple resistance exceed 15% and dual resistance has reached 15% [1][2][3]. Due to their resistance to three or more classes of antimicrobial medication, multidrug- resistant (MDR) bacteria pose a serious threat public health. This summary offers comprehensive details on particular bacterial species linked to multidrug resistance, including their mechanisms, prevalence.
Specific bacteria and associated with multidrug resistance
Mechanism of resistance; A baumannii produces beta- lactamases, especially carbapenemases, which hydrolyse carbapenems and other beta- lactam, as one of its many antibiotic resistance strategies. Additionally, it has changes in outer permeability of the membrane that prevent drug uptake and uses efflux pumps to expel several classes of antibiotics.[1][2]
Prevalence of resistance; studies suggests that A. baumannii demonstrates elevated levels of resistance to multiple drugs. In fact, more than 70% of clinical isolates have been found to be resistant to multiple antibiotics, such as carbapenems and fluroquinolones.[3][4]
Mechanism of resistance; Resistance in Escherichia coli is frequently linked with the synthesis of plasmid- mediated quinolones resistance (PMQR) genes such as qnrS and extended-spectrum beta- lactamases (ESBLs). Fluoroquinolones resistance can be caused by mutations in the gyrA and parC genes.[5][6]
Prevalence of resistance; multidrug- resistant E. coli strains are growing more common, according to systematic review, with resistance rates for commonly used antibiotics reaching 50% in some areas.[7][8]
Strategies to overcome resistance H. pylori
Treatment strategies
Bismuth based Regimens
These regimens are advised as first -line treatments, particularly in areas with high rates of metronidazole and clarithromycin as resistance. They consist of a bismuth as compound, a proton pump inhibitor (PPI), two types of antibiotics (typically metronidazole and tetracycline or amoxicillin), They demonstrated high removal rates (over 90%) if properly administered.[1][2][4].
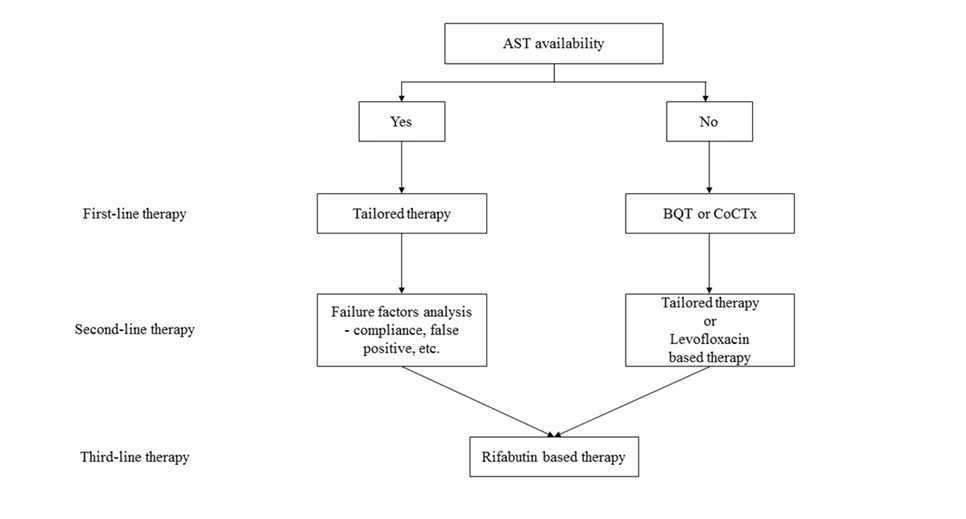
AST, antibacterial susceptibility test; BQT, bismuth quadruple therapy; CoCTx, concomitant therapy
Figure 1. Simplified H. pylori treatment strategy.
Antimicrobial susceptibility test (AST)
Eradication rates are significantly increased by customised therapy based on AST results these approaches involves changing treatment according to with patients unique H. Pylori strain resistance patterns.[2][5]. For example, additional antibiotics can be applied if clarithromycin resistance is found.
These techniques involve using several antibiotics concurrently or with a particular order to increase efficacy and lower the risk of resistance developing sequential treatments usually starts with one antibiotics and progress to another’s, whereas parallel therapy makes use of several antibiotics from the same.[5]
4.1 Nano/Microparticle conjugation the prevent bacteria from adhering to the stomach mucosa, conjugating nanoparticles with H, pylori binding particles like lectin and glycan antigen is effective strategies. This tactic seeks to stop H, pylori from attaching itself to the cell of the stomach in the first place in order to avoid infection.[1]
4.2 Urea coated Nanoparticles by taking advantages of H, pylori’s urel channel, these nanoparticles are intended to enhance the drug delivery by enabling the exact release of therapeutic agents into the bacteria.[1]
5. Metal based Nanoparticles
Silver and copper nanoparticles, among other metal- based nanoparticle (NPs), have demonstrated noteworthy antibacterial capabilities against helicobacter pylori, Reactive oxygen compounds (ROS), which can impair bacteria cell functions and cause cell death, and the release of metal ions are two of the ways that these nanoparticles functions. crucially, metal-based NPs are non-specifically toxic to bacteria, which makes it harder for H, pylori to become resistant to them.[3] because of their special physicochemical characteristics, which enable high reactivity and a large surface area, they have the potential to be useful drugs or substitutes for conventional antibiotics therapies.
5.1 Antibacterial properties If applied to H, pylori, metal nanoparticle like copper (CU) and silver (Ag) have potential antibacterial properties. They function by producing reactive oxygen species (ROS) and releasing metal ions, which can interfere with bacterial cellular processes.[3]. These nanoparticles can be used as useful supplements or substitute for conventional antibiotic treatments.
5.2 Antibiotic-free strategies using metal- based nanoparticle offers a non- antibiotic strategy that keeps high antibacterial activity against H, pylori while lowering the possibility of resistance developing. [3]
6, Sonodynamic Therapy
Sonodynamic therapy (SDT), that treats H,pylori infections by using ultrasound and specifically engineered nanoparticles, is another cutting – edge method. To effectively inactivate H, pylori without the need for antibiotics, lecithin – coated poly (lactic-co-glycolic acid (PLGA) nanoparticles preloaded with verteporfin have been demonstrated to produce ROS upon ultrasound exposure. These approaches reduce changes to the gut microbiota, a common site effect of traditional antibiotic treatments, while simultaneously reducing the bacteria load.[5] this nanoparticle dual function enable them to neutralize important virulence factor generated H, pylori, providing a cutting-edge therapeutic approaches that treat both infection and resistance.
6.1 Ultrasound -medicated treatment using lecithin- coated poly (lactic-co-glycolic acid) (PLGA)nanoparticle loaded with verteporfin in conjunction with ultrasound exposure is a novel technique. This process produces reactive oxygen species (ROS)that can inactivate H, pylori providing a non- antibiotic treatment option with minimal disruption to the gut microbiota [5] Without harming healthy gut flora, this therapy has demonstrated efficacy on par with conventional antibiotic treatment.
Rifabutin based Regimens
The approval of combination treatments based on rifabutin signifies a important progression in the management of helicobacter pylori. These regimens are useful option in regions where there is a high prevalence of clarithromycin resistance because they have demonstrated excellent efficacy towards strains that are resistant and simplify treatment protocols, because of its district mode of action, rifabutin is especially useful in avoiding common resistance pathways liked to other antibiotics [1]
Potassium-competitive Acid Blocker (P-CABs)
Vonoprazan and other potassium – competitive acid blockers are being considered as potential substitutes for conventional proton pump inhibitor (PPI) P-CABs have been shown to be more effective in treating patients with H, pylori infection resistance to clarithromycin. Because they are better at maintaining stomach PH levels than proton pump inhibitors (PPIs), co administered antibiotics are more stable and effective, which increases the rate of eradication.[3][4]
Molecular based Genotypic Testing
PCR and other molecular testing techniques enables the quick detection of antibiotics resistant mutations in H, pylori with this method therapy can be customized based on individual resistance of profiles, greatly enhancing the effectiveness of treatments, there are also plans to develop pre treatment stool based genetic tests that could allow a patient to switch form empirical therapies to resistance guided treatment without requiring invasive procedures like endoscopy.[1][4]
Antimicrobial stewardship
For successful management of H, pylori infections a shift from trial-and-error methods to antimicrobial management is imperative. To prevent the emergence of resistance and enhance patience outcomes, the approaches to builds a strong emphasis on using antibiotics as efficiently as possible according with clinical guidelines and susceptibility testing.[4]. Effective treatment choice can be further aided by the implementation of surveillance registers for resistance patterns.
Probiotics as Adjunct Therapy
Adding multi-strain probiotics to common antibiotic regimens has become a popular adjunct therapy to increase antibiotic treatment eradication rates and reduce side effects. Probiotics may improve patience compliance and treatment outcomes by balancing the gut microbiota and reducing gastrointestinal side effects.
Recent Advancements
A significant advance in the management of H, pylori infections has been the advent of rifabutin- based combination therapies, especially in populations where the prevalence of clarithromycin resistance is high. it has been demonstrated that rifabutin is a very effective medication that reduce treatment protocols and offers a substitute when conventional regimen doesn’t work.[1]
Furthermore, the efficacy potassium competitive acid blockers (P-CABs) like vonoprazan are dual or triple therapy regimen is being evaluated; these patient with clarithromycin resistant strains have shown improved outcomes. [1][4]
The use of genotypic testing based on molecules is becoming more popular as a fast and accurate way to detect resistance to antibiotics. Method like polymerase chain reaction (PCR) make it possible to identify specific mutation linked to resistance, allowing for specific therapy regimens that can greatly increase eradication rates.[4]
By generating reactive oxygen compound and releasing metal ions, metal-based nanoparticle like copper and silver have strong antibacterial effect on H. pylori, These nanoparticle offers a viable substitute for conventional antibiotics have the potential to reduce resistance.[4] By binding to the urel means for example, targeted nanotherapeutics, such as nanoparticle, such as nanoparticles conjugated with H.pylori, binding molecules, can deliver drugs directly to the bacteria and prevent them from adhering to the gastric mucosa .[4]
Treatment regimens that include multi-strain probiotics have demonstrated promise in improving antibiotic therapy side effect rates and eradication rates. Probiotics may improve the balance of gut microbiota that antibiotics have upset and enhance the effectiveness of treatment as a whole. [4]
REFERENCES


Gulafroz*, Dr Manoj Kumar Sarangi, Strategies in Overcoming Drug Resistances in H. Pylori Infection, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 3096-3111 https://doi.org/10.5281/zenodo.15108515
 10.5281/zenodo.15108515
10.5281/zenodo.15108515
