SET’s College of Pharmacy, Dharwad, Karnataka 580002
Diabetes mellitus (DM) is a chronic metabolic disorder marked by persistent hyperglycaemia, arising from either autoimmune-mediated ?-cell destruction or impaired insulin action and secretion. Globally, DM prevalence has escalated, with type 2 diabetes mellitus (T2DM) accounting for 90–95% of cases, while type 1 diabetes mellitus (T1DM) and gestational diabetes mellitus (GDM) contribute smaller proportions but with significant health risks. Uncontrolled DM leads to severe microvascular and macrovascular complications, including neuropathy, nephropathy, retinopathy, and cardiovascular disease. Diagnosis is achieved through biochemical markers such as fasting blood glucose, HbA1c, and glucose tolerance tests. Management strategies encompass lifestyle modification, pharmacotherapy with oral hypoglycaemics and insulin, and self-monitoring of blood glucose. Recent therapeutic advances highlight nanotechnology, continuous glucose monitoring, gene therapy, stem cell therapy, and medical nutrition therapy as promising interventions to improve glycaemic control and reduce disease burden. This review provides an integrated overview of DM classification, pathophysiology, clinical presentation, complications, diagnostic approaches, conventional treatment, and emerging frontiers, underscoring the urgent need for early diagnosis and innovative strategies to curb the global diabetes epidemic.
Diabetes is characterized by elevated blood glucose levels, either in the fasting state or after meals. Persistent hyperglycaemia in diabetes mellitus (DM) contributes to progressive damage, dysfunction, and eventual failure of various organs and tissues, notably the retina, kidneys, peripheral nerves, heart, and vascular system1.
The pathogenesis of diabetes mellitus primarily involves two key mechanisms: autoimmune-mediated destruction of pancreatic β-cells, resulting in inadequate insulin production, and intrinsic cellular resistance to insulin action. These processes collectively contribute to the persistent hyperglycaemia characteristic of the disease2.
Diabetes mellitus (DM) is among the most prevalent metabolic disorders globally, with its incidence rising at an alarming pace. Between 1980 and 2014, the number of individuals diagnosed with DM surged from 108 million to 422 million. During the same period, the global prevalence of diabetes among adults aged 18 years and older increased from 4.7% to 8.5%. According to the World Health Organization (WHO), diabetes is projected to become the seventh leading cause of mortality by 2030.
Type 1 diabetes mellitus (T1DM), typically diagnosed during childhood or adolescence, accounts for approximately 5–10% of all diabetes cases and is primarily characterized by autoimmune destruction of pancreatic β-cells. In contrast, Type 2 diabetes mellitus (T2DM) represents the predominant form, comprising 90–95% of cases, and is commonly associated with insulin resistance and relative insulin deficiency.
Gestational diabetes mellitus (GDM) is a distinct subtype that manifests exclusively during pregnancy, affecting approximately 5–15% of pregnant women, with prevalence varying across ethnic groups and geographic regions. Notably, 40–60% of women diagnosed with GDM are at risk of developing overt diabetes within 5–10 years postpartum3.
TYPES OF DIABETES MELLITUS AND THEIR PATHOPHYSIOLOGY
Type 1 diabetes mellitus
Type 1 Diabetes Mellitus (T1DM), also known as autoimmune diabetes, insulin-dependent diabetes mellitus (IDDM), juvenile-onset, or ketosis-prone diabetes, is a chronic condition primarily affecting children and young adults. It is characterized by the autoimmune destruction of pancreatic β-cells, leading to an absolute deficiency of insulin. This destruction is mediated by CD4+ and CD8+ T cells and macrophages infiltrating the islets, and is often accompanied by the presence of autoantibodies such as anti-glutamic acid decarboxylase (GAD), islet cell antibodies, and insulin autoantibodies, which are detectable in 85–90% of individuals at the onset of fasting hyperglycaemia. The exact cause remains unknown, but strong evidence supports an autoimmune mechanism. Individuals with T1DM may also present with other autoimmune disorders like Graves’ disease, Hashimoto’s thyroiditis, and Addison’s disease. The disease disrupts normal glucose regulation not only due to insulin deficiency but also because of α-cell dysfunction, resulting in excessive glucagon secretion that exacerbates hyperglycaemia and contributes to metabolic imbalances. This dysregulation often leads to diabetic ketoacidosis in the absence of insulin therapy. Furthermore, insulin deficiency impairs peripheral glucose utilization by promoting uncontrolled lipolysis and elevating plasma free fatty acids, which inhibit glucose metabolism in tissues such as skeletal muscle. It also downregulates key insulin-responsive genes like glucokinase in the liver and GLUT4 transporters in adipose tissue, further compromising glucose uptake. Lifelong insulin administration remains the cornerstone of treatment to manage this life-threatening condition4-5.
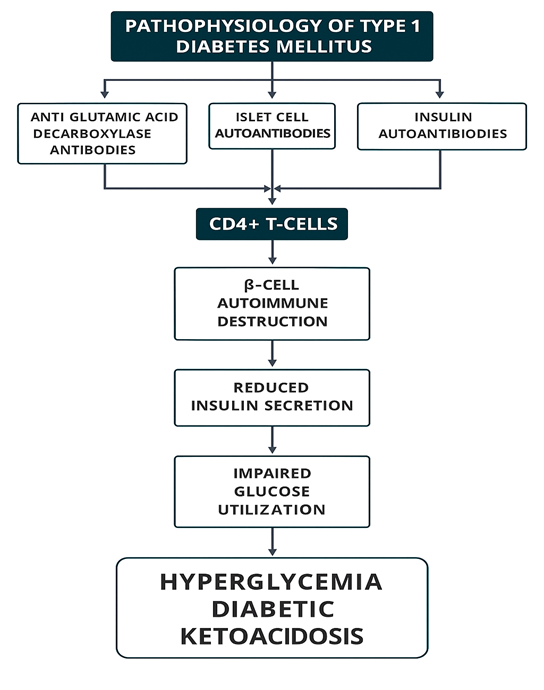
Figure 1. Pathophysiology of T1DM
Type 2 diabetes mellitus
Type 2 Diabetes Mellitus (T2DM) is a prevalent metabolic disorder caused by defective insulin secretion from pancreatic β-cells and impaired insulin response in target tissues. Proper insulin synthesis, release, and action are essential for metabolic balance; disruptions in these mechanisms lead to T2DM.
According to the WHO, diabetes is a chronic condition marked by elevated blood glucose, which over time damages the heart, blood vessels, eyes, kidneys, and nerves. Over 90% of cases are T2DM, characterized by insulin resistance (IR), β-cell dysfunction, and inadequate compensatory insulin secretion, resulting in hyperglycaemia.
T2DM is commonly associated with obesity, especially abdominal fat, which contributes to IR via inflammatory pathways, increased free fatty acids, and adipokine imbalance. Key drivers of the global T2DM epidemic include rising obesity, sedentary behaviour, high-calorie diets, and aging populations.
Pathogenesis centres on two mechanisms:
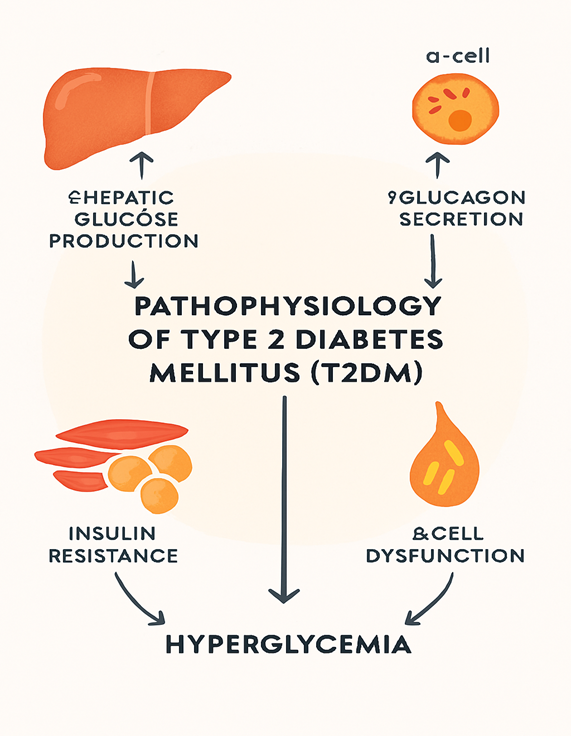
Figure 2. Pathophysiology of T2DM
Gestational Diabetes Mellitus
Gestational diabetes mellitus (GDM) is a metabolic disorder affecting 14% of pregnancies worldwide, or 18–20 million births annually. It arises from insufficient insulin secretion during pregnancy, leading to hyperglycaemia. Risk factors include obesity, poor diet, sedentary lifestyle, and family history of diabetes. In obese women, GDM results from amplified insulin resistance due to pre-existing metabolic dysfunction. In lean women, impaired first-phase insulin response plays a larger role. Maternal hyperglycaemia causes excess glucose transfer to the foetus, triggering foetal hyperinsulinemia and resulting in macrosomia (birth weight >4000 g)7-8.
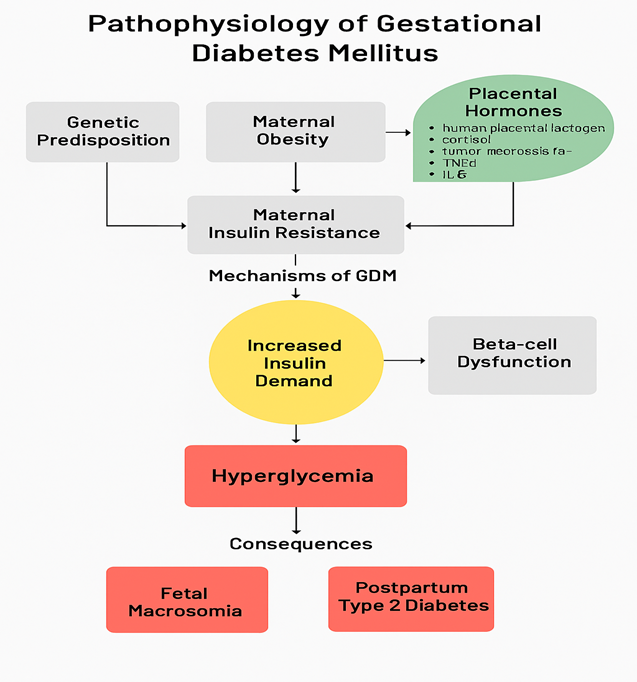
Figure 3. Pathophysiology of GDM
SYMPTOMS OF DM
Diabetes symptoms are caused by rising blood sugar.
Symptoms of type 1 diabetes can include
Symptoms of type 2 diabetes can include
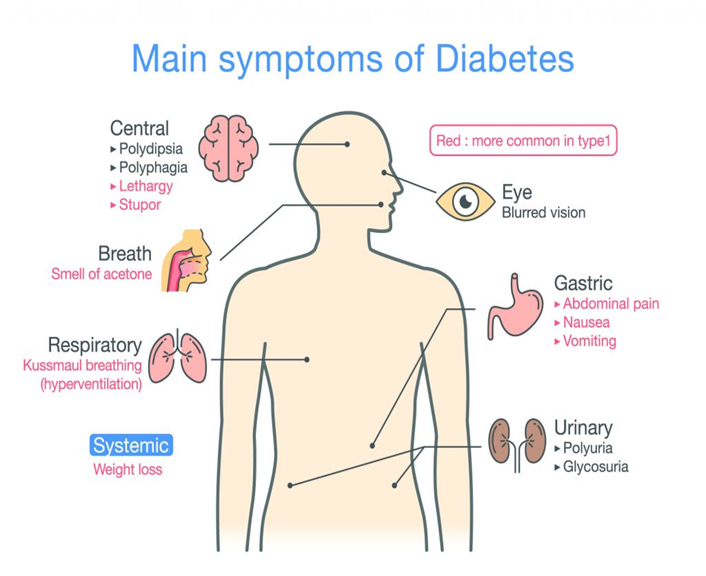
Figure 4. Main symptoms of Diabetes Mellitus
COMPLICATIONS OF DM
As diabetes progresses, tissue and vascular damage become more pronounced, leading to severe complications such as diabetic retinopathy, neuropathy, cardiovascular disorders, and ulceration. Patients with long-standing Type 1 diabetes mellitus (T1DM) are particularly vulnerable to microvascular complications, including damage to the retina, kidneys, and peripheral nerves. They may also develop macrovascular diseases affecting the coronary arteries, heart, and peripheral vasculature.
Type 2 diabetes mellitus (T2DM), on the other hand, carries a significantly higher risk of large vessel disease. It is commonly associated with comorbid conditions such as hypertension and dyslipidaemia. Consequently, most patients with T2DM are predisposed to cardiovascular complications, which remain the leading cause of morbidity and mortality in this population10.
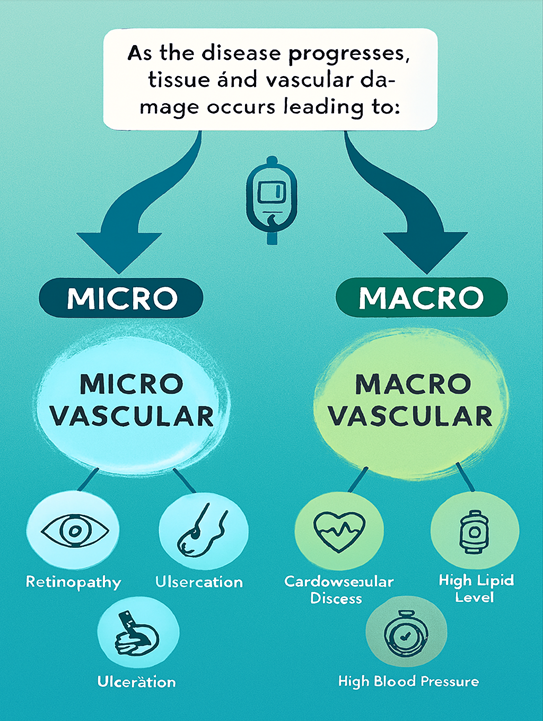
Figure 5. Complications of DM
DIAGNOSIS OF DM
A1C test. This blood test, which doesn't require not eating for a period of time (fasting), shows your average blood sugar level for the past 2 to 3 months. It measures the percentage of blood sugar attached to hemoglobin, the oxygen-carrying protein in red blood cells. It's also called a glycated hemoglobin test. The higher your blood sugar levels, the more hemoglobin you'll have with sugar attached. An A1C level of 6.5% or higher on two separate tests means that you have diabetes. An A1C between 5.7% and 6.4% means that you have prediabetes. Below 5.7% is considered normal.
Random blood sugar test. A blood sample will be taken at a random time. No matter when you last ate, a blood sugar level of 200 milligrams per deciliter (mg/dL), 11.1 millimoles per liter (mmol/L) or higher suggests diabetes.
Fasting blood sugar test. A blood sample will be taken after you haven't eaten anything the night before (fast). A fasting blood sugar level less than 100 mg/dL (5.6 mmol/L) is normal. A fasting blood sugar level from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) is considered prediabetes. If it's 126 mg/dL (7 mmol/L) or higher on two separate tests, you have diabetes.
Glucose tolerance test. For this test, you fast overnight. Then, the fasting blood sugar level is measured. Then you drink a sugary liquid, and blood sugar levels are tested regularly for the next two hours. A blood sugar level less than 140 mg/dL (7.8 mmol/L) is normal. A reading of more than 200 mg/dL (11.1 mmol/L) after two hours means you have diabetes. A reading between 140 and 199 mg/dL (7.8 mmol/L and 11.0 mmol/L) means you have prediabetes11.
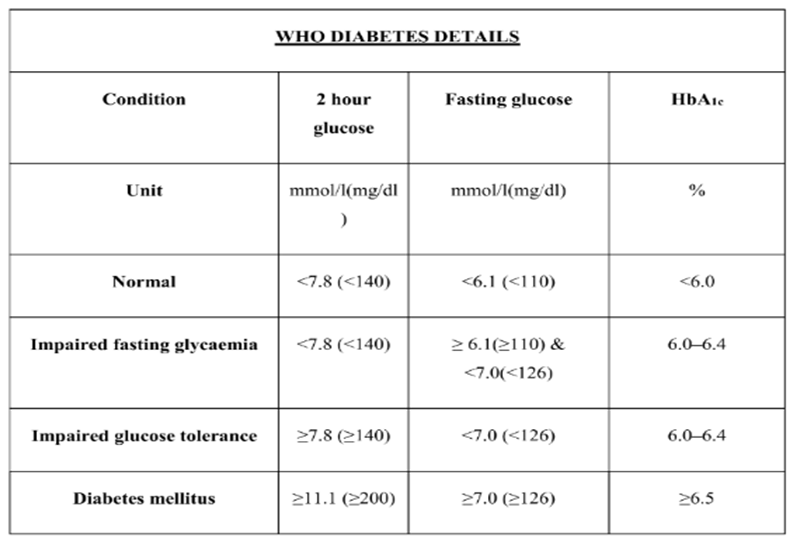
Figure 6. WHO Diabetes information chart of DM
TREATMENT OF DIABETES MELLITUS
Self-monitoring of blood glucose (SMBG) is a critical component in the management of type 1 diabetes mellitus (DM) and insulin-dependent type 2 DM. It enables patients to adjust insulin doses effectively, thereby minimizing the risk of both hypoglycaemia and hyperglycaemia.
According to the American Diabetes Association (ADA) guidelines, individuals with type 1 DM should monitor their blood glucose levels at the following times:
Patients must be educated on interpreting real-time glucose readings to make informed decisions about dietary intake and medication adjustments.
While SMBG is commonly advised for patients with type 2 DM, especially those on insulin therapy, its standalone effectiveness remains uncertain. Although early studies indicated improvements in HbA1c levels, confounding factors such as concurrent lifestyle modifications (e.g., diet and exercise) complicate the evaluation of SMBG’s direct impact.
The ADA recommends the following glycaemic targets:
Table 1. Oral Agents with Mechanism of Action and Side Effects13
|
Oral Antidiabetics |
Mechanism of Action |
Side Effects |
|
Sulfonylureas Glimiperide(Amaryl) Glipizide (Glucotrol) Glipizide-gits (GlucotrolXL) Glibenclamide Glyburide (Diabeta,Micronase) Glyburide-micronized (Glynase) Tolbutamide (Orinase) Chlorpropamide (Diabinese) Tolazamide (Tolinase) Acetoheximide (Dymelor) |
Stimulate first-phase insulin secretion by blocking K+ channel in ß- cells. |
Late hyperinsulinemia and hypoglycemia Weight gain. |
|
Meglitinides Repaglinide (Prandin) Nateglinide (Starlix) |
Stimulate first- phase insulin secretion by blocking K+ channel in ß-cells |
Hypoglycemia Weight gain. |
|
Biguanides Metformin (Glucophage,Riomet) Metformin-XR(Glucophage-XR) |
Decrease hepatic glucose production Increase muscle glucose uptake and utilization |
Nausea, Diarrhea Anorexia, Lactic acidosis. |
|
Thiazolidinedinediones Rosiglitazone (Avandia) Pioglitazone (Actos) |
Increase insulin sensitivity via Activation of PPAR-g receptors |
Fluid retention and weight gain. |
|
α-Glucoside Inhibitors Acarbose (Precose) Miglitol (Glyset) |
Decrease hepatic glucose production Delays glucose absorption |
Flatulence Abdominal bloating |
RECENT THERAPIES FOR TREATMENT OF DIABETES MELLITUS14
Here are several modern approaches involved in the management of diabetes. However, early diagnosis is central to achieving any targets set in DM management:
Lifestyle modification is a cornerstone of diabetes management, recommended for both pre-diabetic and diabetic individuals. Key changes include increasing physical activity, and adopting a healthy diet rich in vegetables, fruits, whole grains, lean meats, and non-fat dairy, while limiting sugary and fatty foods. Patients are also encouraged to quit smoking and reduce alcohol consumption.
Nanotechnology involves the use of nanoparticles (<100 nm). This has opened new frontiers in diabetes care. In medicine, this approach—known as nanomedicine—enhances the delivery and targeting of drugs and diagnostic agents. In diabetes, nanotechnology has enabled the development of advanced glucose monitoring systems and non-invasive insulin delivery methods. It also supports innovative therapies like cell-based and gene-based treatments for type 1 diabetes. Importantly, nanotech tools can detect immune cell activity, monitor beta-cell mass, and improve early diagnosis, which is crucial for preventing disease progression. Alternative non-invasive delivery routes, including oral, transdermal, and inhalation methods, are also under exploration to improve patient compliance and therapeutic outcomes.
Traditional glucose monitoring methods, involving frequent finger pricks, often suffer from poor compliance and limited temporal coverage (e.g., during sleep or driving). This can lead to dangerous glycaemic fluctuations and increased risk of complications. CGM systems, especially those using subcutaneous biosensors like amperometric sensors, offer a more consistent monitoring approach.
Medical Nutrition Therapy (MNT), delivered by registered dietitian nutritionists, is a cornerstone of diabetes management. It involves personalized nutrition diagnosis and counselling aimed at achieving glycaemic control and preventing complications. MNT is especially vital in gestational diabetes mellitus (GDM), where carbohydrate intake plays a central role. While low-carbohydrate diets have traditionally been used, emerging evidence supports the efficacy of low-glycaemic index diets in managing GDM.
Gene therapy is an innovative technique aimed at correcting disease symptoms caused by defective genes through the introduction or manipulation of functional genetic material.
Types of gene therapy:
In diabetes mellitus (DM), particularly type 1 diabetes mellitus (T1DM), gene therapy is emerging as a promising alternative to conventional treatments. T1DM is an autoimmune condition characterized by T-cell-mediated destruction of insulin-producing beta cells. Its multifactorial etiology involves both genetic and environmental factors. Recent research has identified several genes implicated in T1DM pathogenesis, making them potential targets for gene-based interventions.
In type 2 diabetes mellitus (T2DM) One notable target is NLRP3, a gene whose inhibition reduces inflammation and protects beta cells from apoptosis, thereby preventing T2DM onset in animal models.
Conventional diabetes treatments often fail to address the root causes and may carry adverse effects. Stem cell therapy offers a regenerative alternative by aiming to restore insulin-producing beta cells. While pancreas or islet-cell transplantation has shown promise, it’s limited by donor organ scarcity. Stem cells, with their unique ability to differentiate and regenerate, present a viable solution to this challenge.
Table 2. Stem cells drugs in the Pipeline
|
Drug Candidate |
Developer |
Mechanism Of Action |
Target Condition |
|
LY3502970 |
Eli Lilly |
Partial GLP-1R agonist (G-protein biased) |
Type 2 Diabetes (T2DM) |
|
SCO-094 |
SCOHIA |
Dual GIP and GLP-1receptor agonist |
Type 2 diabetes (T2DM) |
|
Ladarixin (LD) |
Dompé Farmacei |
CXCR1/ CXCR2 inhibitor |
New-onset Type 1 Diabetes (T1DM) |
CONCLUSION
Diabetes mellitus continues to pose a significant global health challenge, driven by lifestyle transitions, genetic susceptibility, and environmental factors. Despite advances in diagnosis and treatment, the burden of complications such as cardiovascular disease, neuropathy, nephropathy, and retinopathy remains high, highlighting the importance of early detection and effective management strategies. Conventional therapies, including lifestyle modification, insulin, and oral hypoglycaemics, form the cornerstone of treatment, yet emerging approaches—such as nanotechnology, continuous glucose monitoring, gene therapy, and stem cell-based interventions—offer promising avenues for more precise and personalized care. A multidisciplinary strategy integrating prevention, patient education, pharmacological innovations, and cutting-edge biomedical technologies is essential to reduce morbidity and mortality associated with diabetes. Ultimately, ongoing research and innovation hold the key to transforming diabetes management and mitigating its impact on individuals and healthcare systems worldwide.
ACKNOWLEDGEMENT
I would like to express my sincere gratitude to SET’s College of Pharmacy, Dharwad for providing the necessary infrastructure and academic support throughout the course. I am deeply thankful to my guide—her expertise and mentorship have been instrumental in shaping the direction and quality of this work. I also extend my appreciation to the faculty and staff for offering excellent facilities and fostering a stimulating academic environment. Finally, I am immensely grateful to my family, friends and Amrut Khavi for their constant encouragement and patience, which kept me motivated during the most challenging phases of this journey.
REFERENCES


Neelamma Koganuramath, Mahananda Uppin, Diabetes Mellitus Decoded: Classification, Diagnosis, Therapeutics, and Emerging Drug Frontiers, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 528-537. https://doi.org/10.5281/zenodo.17278455
 10.5281/zenodo.17278455
10.5281/zenodo.17278455
