Department of Pharmacy, Annamalai University, Tamilnadu, India.
Pain remains one of the most common clinical complaints, and its effective management represents a cornerstone of medical care. Among the most widely used analgesics worldwide are acetaminophen (paracetamol) and non-steroidal anti-inflammatory drugs (NSAIDs). Although both are frequently employed in clinical practice, their pharmacological mechanisms, therapeutic profiles, and adverse effect spectrums differ significantly. This review provides a comprehensive comparison of the pharmacological mechanisms of acetaminophen and NSAIDs in pain management, integrating current evidence from preclinical studies, clinical trials, and meta-analyses. Emphasis is placed on central and peripheral actions, molecular targets, efficacy across pain conditions, safety considerations, and evolving mechanistic insights. By systematically analyzing their similarities and differences, this review highlights the rational clinical use of each agent and their roles in multimodal pain management strategies.
Pain management remains a central concern in clinical medicine, with millions of patients globally seeking relief from both acute and chronic pain syndromes. Analgesic pharmacotherapy often relies on two major classes: acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs). Despite their widespread use, controversies persist regarding their exact mechanisms, comparative efficacy, and safety in diverse patient populations [1–3].
NSAIDs act primarily by inhibiting cyclooxygenase (COX) enzymes and subsequently reducing prostaglandin synthesis, thereby exerting both analgesic and anti-inflammatory effects [4,5]. In contrast, acetaminophen, although traditionally grouped with NSAIDs for its analgesic and antipyretic properties, displays minimal peripheral anti-inflammatory activity and its precise mechanism remains incompletely elucidated [6–8]. Increasing evidence suggests involvement of central COX inhibition, serotonergic modulation, endocannabinoid pathways, and transient receptor potential (TRP) channels in acetaminophen’s analgesic profile [9–12].
Given the enormous clinical and economic implications of pain therapy, a detailed comparative evaluation of acetaminophen and NSAIDs is warranted. This review synthesizes mechanistic, pharmacological, and clinical data, providing a framework for understanding their roles in pain management.
2. HISTORICAL PERSPECTIVE
The historical development of acetaminophen and NSAIDs reveals both convergence and divergence in their clinical adoption. NSAIDs trace their origins to the discovery of salicylates in willow bark, later leading to the synthesis of aspirin by Bayer in 1897 [13,14]. Subsequent decades saw the introduction of various non-selective NSAIDs, followed by selective COX-2 inhibitors [15,16].
Acetaminophen, on the other hand, was first synthesized in the late 19th century but gained widespread use only in the mid-20th century after recognition of its favorable safety profile compared to phenacetin [17,18]. Today, acetaminophen is considered a first-line agent for mild to moderate pain and fever, while NSAIDs are reserved for conditions requiring additional anti-inflammatory action [19,20].
The differing developmental trajectories of these agents underscore the importance of mechanistic distinctions in shaping clinical practice.
3. BASIC PHARMACOLOGY OF NSAIDs
NSAIDs exert their effects by targeting the cyclooxygenase enzymes COX-1 and COX-2, which catalyze the conversion of arachidonic acid into prostaglandins and thromboxanes [21,22]. COX-1 is constitutively expressed in most tissues, regulating physiological processes such as gastric mucosal protection, platelet aggregation, and renal blood flow [23]. In contrast, COX-2 is inducible and upregulated in inflammatory states, driving pain and fever responses [24].
Most traditional NSAIDs are non-selective, inhibiting both isoforms to varying degrees. Selective COX-2 inhibitors, developed to minimize gastrointestinal toxicity, demonstrated reduced ulcerogenic potential but were later linked to increased cardiovascular risk [25–27]. This duality highlights the delicate balance between efficacy and safety in NSAID pharmacology.
Additionally, NSAIDs may influence ion channels, oxidative stress, and apoptotic pathways, broadening their pharmacodynamic spectrum beyond COX inhibition [28,29].
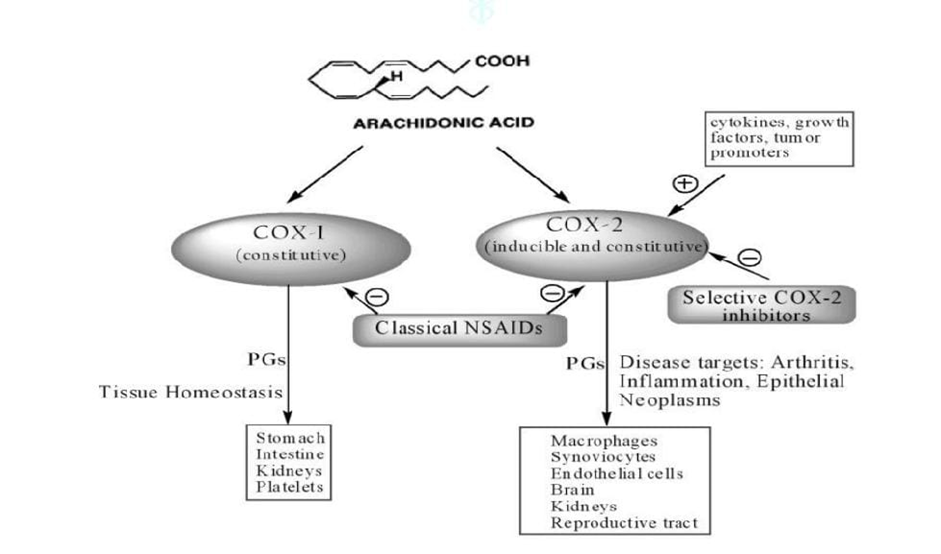
Figure 1: General mechanism of NSAIDs.
4. BASIC PHARMACOLOGY OF ACETAMINOPHEN
Unlike NSAIDs, acetaminophen demonstrates minimal peripheral COX inhibition at therapeutic concentrations, suggesting a primarily central mechanism of action [30,31]. Studies indicate preferential inhibition of COX activity in the brain, contributing to its analgesic and antipyretic effects [32].
Acetaminophen is rapidly absorbed after oral administration, undergoes hepatic metabolism primarily via glucuronidation and sulfation, and produces a small fraction of the reactive metabolite N-acetyl-p-benzoquinone imine (NAPQI). Under normal conditions, NAPQI is detoxified by glutathione conjugation, but in overdose it accumulates, leading to hepatotoxicity [33–35].
Emerging evidence implicates descending serotonergic pathways, cannabinoid receptor activation via its metabolite AM404, and TRPV1 modulation in acetaminophen’s analgesic profile [36–39]. These insights position acetaminophen as a centrally acting analgesic distinct from peripherally acting NSAIDs.
5. MECHANISMS OF ACTION: MOLECULAR PATHWAYS
Cyclooxygenase (COX) Inhibition as a Core Mechanism
The central pharmacological effect of NSAIDs arises from inhibition of cyclooxygenase (COX) enzymes, reducing the biosynthesis of prostaglandins and thromboxanes from arachidonic acid [4,13]. Prostaglandins play pivotal roles in peripheral sensitization, inflammatory hyperalgesia, and fever [20]. By suppressing prostaglandin formation, NSAIDs provide both analgesia and anti-inflammatory effects [4,24].
Acetaminophen’s mechanism is more complex. Although traditionally considered a weak peripheral COX inhibitor, evidence indicates preferential inhibition of prostaglandin synthesis within the central nervous system (CNS) [5,27,33]. Studies have proposed that acetaminophen’s selectivity may relate to peroxidase activity levels: in inflamed peripheral tissues with high peroxide tone, acetaminophen is ineffective, whereas in the CNS with lower peroxide concentrations, inhibition is possible [5,14].
This fundamental distinction explains the lack of anti-inflammatory activity of acetaminophen compared with NSAIDs.
The COX-3 Hypothesis
A major mechanistic debate in acetaminophen pharmacology emerged with the discovery of COX-3, a splice variant of the COX-1 gene expressed in the canine cerebral cortex [21]. Initial studies suggested that acetaminophen selectively inhibited COX-3, potentially accounting for its central analgesic and antipyretic effects [26].
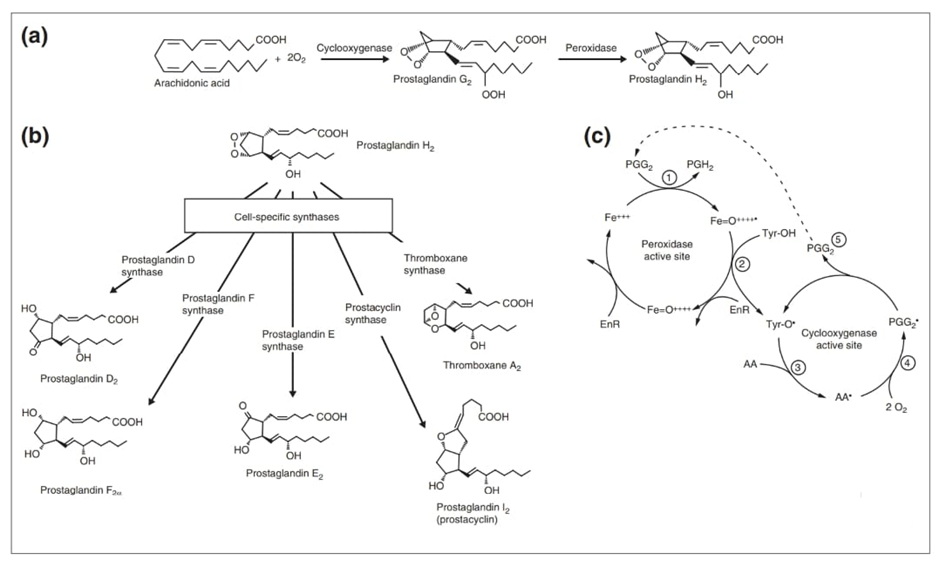
Figure 2: Production of prostaglandins by COXs. (a) The two reactions performed by cyclooxygenases: the conversion of arachidonic acid to prostaglandin G2 by the cyclooxygenase activity and the conversion of prostaglandin G2 to prostaglandin H2 by the peroxidase activity. (b) The cell-specific synthases that are involved in the conversion of prostaglandin H2 to the five principal prostaglandins. (c) The reaction mechanism of COX-1.
(1) First, a ferryl-oxo (FeIV) protoporphyrin radical in the heme in the peroxidase active site is produced when endogenous oxidant(s) oxidizes ferric heme (FeIII) to ferryl-oxo (FeIV) protoporphyrin radical through a two-electron oxidation. (2) The Tyr384 residue in the cyclooxygenase active site is activated, through a single-electron reduction reaction with the FeIV protoporphyrin radical, to produce a tyrosyl radical. In the first step of the oxygenation process (3), the 13-pro(S) hydrogen of arachidonic acid in the COX site is abstracted by the tyrosyl radical to produce the arachidonyl radical. (4) This is followed by the reaction of the arachidonyl radical with two molecules of oxygen, to yield prostaglandin G2. (5) Prostaglandin G2 then diffuses (dotted line) to the peroxidase active site and is reduced to prostaglandin H2 by the peroxidase activity (1). AA, arachidonic acid; EnR, an endogenous reductant; Fe+++, ferric heme; Fe=O ++++, Ferryl-oxo FeIV porphyrin radical; Tyr-OH, active site tyrosine; Tyr-O, tyrosyl radical.
However, subsequent work questioned the physiological relevance of COX-3 in humans, as splice variants do not appear to yield functional enzymes in human tissues [33]. Current consensus maintains that while COX-3 inhibition may contribute in certain species, acetaminophen’s mechanism in humans likely involves alternative pathways [27].
Serotonergic Descending Pain Pathways
Accumulating evidence implicates descending serotonergic pathways in the analgesic activity of acetaminophen [14]. Preclinical studies demonstrated that serotonin receptor antagonists attenuate acetaminophen-induced analgesia, suggesting that spinal 5-HT transmission plays a critical role [27]. This pathway may amplify central pain inhibition, differentiating acetaminophen from NSAIDs, which primarily act peripherally [4].
NSAIDs, by contrast, influence descending modulation indirectly through reduced peripheral nociceptive input [13]. The serotonergic involvement thus highlights a fundamental mechanistic divergence between the two drug classes.
Endocannabinoid System and AM404
A breakthrough in acetaminophen pharmacology was the identification of its active metabolite, AM404, generated via fatty acid amide hydrolase (FAAH)-mediated conjugation of p-aminophenol with arachidonic acid [6,28]. AM404 inhibits the reuptake of endogenous cannabinoids such as anandamide, thereby enhancing cannabinoid receptor (CB1 and CB2) signaling [6].
This mechanism provides a strong rationale for acetaminophen’s central analgesic activity and underscores its distinctiveness from NSAIDs. Indeed, NSAIDs do not modulate the endocannabinoid system directly, although interactions with cannabinoid pathways have been reported in experimental models [27].
TRPV1 Receptor Activation
Another mechanistic insight is acetaminophen’s modulation of the transient receptor potential vanilloid 1 (TRPV1) channel, anociceptive receptor involved in thermosensation and hyperalgesia. AM404 acts as a TRPV1 agonist, and studies confirm that blockade of TRPV1 attenuates acetaminophen-induced analgesia [22]. This link reinforces the concept of acetaminophen as a centrally acting analgesic with multimodal molecular targets.
NSAIDs, in contrast, exhibit no direct TRPV1 modulation, although prostaglandins influence TRPV1 sensitization peripherally [20].
Nitric Oxide and Oxidative Stress Pathways
NSAIDs modulate nitric oxide (NO) synthesis indirectly by suppressing prostaglandins that regulate endothelial function [48]. Some NSAIDs also exert redox effects that contribute to both therapeutic efficacy and toxicity [29].
Acetaminophen may interact with NO synthase pathways under oxidative stress conditions, although the clinical relevance remains debated [33]. Hepatic injury induced by acetaminophen overdose involves nitrosative stress and mitochondrial dysfunction, linking mechanistic pathways to toxicity rather than analgesia [15,67].
Ion Channels and Beyond
Emerging evidence suggests that both NSAIDs and acetaminophen interact with ion channels beyond COX inhibition. Certain NSAIDs modulate voltage-gated sodium and potassium channels, contributing to analgesic activity independent of prostaglandin suppression [29].
Acetaminophen’s interactions with TRP channels (notably TRPV1 and TRPA1) are increasingly recognized, broadening its pharmacological landscape [22]. These multimodal effects highlight that acetaminophen is not merely a "weak NSAID," but instead represents a distinct analgesic entity.
6. COMPARATIVE MOLECULAR INSIGHTS
Taken together, NSAIDs primarily act peripherally by reducing prostaglandin synthesis through COX inhibition, while acetaminophen exerts centrally mediated effects involving serotonergic, cannabinoid, and TRP pathways [4–6,14,22,27].
The mechanistic complementarity of these two drug classes explains the rationale for their combined use in multimodal analgesia, which often provides superior pain relief compared with monotherapy [40,81].
7. PHARMACOKINETICS OF NSAIDS
Absorption and Bioavailability NSAIDs are generally well absorbed after oral administration, with bioavailability typically exceeding 80% [10,17]. Peak plasma concentrations occur within 1–3 hours, depending on the specific compound and formulation [17]. Food delays absorption but does not significantly alter the extent of absorption for most NSAIDs [10].
Ibuprofen, for example, demonstrates rapid absorption and an elimination half-life of approximately 2 hours, contributing to its frequent dosing requirement [10,17]. Naproxen exhibits slower absorption but a longer half-life, allowing for twice-daily dosing [17]. Selective COX-2 inhibitors, such as celecoxib, display variable bioavailability and are influenced by food intake [18].
Distribution
NSAIDs are highly protein-bound (>95%), primarily to albumin [10]. This high binding capacity influences drug interactions, as displacement by other agents may increase free drug concentrations. NSAIDs are widely distributed in tissues, with high concentrations in inflamed synovial fluid, correlating with their efficacy in arthritic conditions [17,20].
Metabolism and Elimination
Most NSAIDs undergo extensive hepatic metabolism through cytochrome P450 isoenzymes, followed by renal excretion of metabolites [17,19]. Variability in metabolic pathways contributes to inter-individual differences in drug response and adverse effect risk. For instance, polymorphisms in CYP2C9 affect clearance of diclofenac and celecoxib [18].
Renal elimination is clinically relevant, as accumulation of NSAIDs in patients with impaired kidney function may exacerbate nephrotoxicity [2,19,60].
8. PHARMACOKINETICS OF ACETAMINOPHEN
Absorption and Bioavailability
Acetaminophen is rapidly and almost completely absorbed from the gastrointestinal tract, with peak plasma levels occurring within 30–60 minutes after oral dosing [11,12]. Bioavailability ranges from 70–90% due to first-pass metabolism [11]. Intravenous formulations achieve higher and more predictable plasma concentrations, which is advantageous in perioperative settings [79].
Distribution
The drug is moderately protein-bound (<20%) and widely distributed across tissues, including the central nervous system, consistent with its central mechanism of action [27]. Placental transfer occurs readily, but therapeutic use in pregnancy is generally considered safe, though controversies regarding developmental outcomes persist [39].
Metabolism and Elimination
Acetaminophen undergoes extensive hepatic conjugation via glucuronidation and sulfation pathways [15,27]. A minor but clinically significant pathway involves oxidation by CYP2E1, producing the reactive metabolite N-acetyl-p-benzoquinone imine (NAPQI) [15,16,66]. Under normal conditions, NAPQI is detoxified by glutathione conjugation. However, in overdose or glutathione depletion, hepatocellular necrosis occurs [16,67,71]. Renal excretion of conjugated metabolites represents the primary elimination route, with a half-life of 2–3 hours in healthy adults [11].
9. COMPARATIVE PHARMACOKINETICS
The contrasting pharmacokinetics of acetaminophen and NSAIDs underscore their distinct clinical profiles. NSAIDs’ high protein binding and peripheral tissue accumulation enhance anti-inflammatory efficacy but also increase the risk of renal and gastrointestinal adverse effects [2,19,48]. Acetaminophen’s lower protein binding, rapid CNS penetration, and reliance on hepatic conjugation explain both its central action and hepatotoxic potential [27,66].
The short half-life of acetaminophen necessitates frequent dosing, although extended-release preparations improve compliance. In contrast, long-acting NSAIDs (e.g., naproxen, meloxicam) offer dosing convenience but may increase adverse event risks in vulnerable populations [17].
10. PHARMACODYNAMICS OF NSAIDs
Analgesic Effects
NSAIDs reduce peripheral sensitization by lowering prostaglandin-mediated nociceptor activation, particularly at sites of tissue injury and inflammation [4,13]. Clinical trials demonstrate significant efficacy in musculoskeletal pain, osteoarthritis, rheumatoid arthritis, and acute postoperative pain [3,23,43,44].
Anti-inflammatory Effects
The hallmark of NSAID pharmacodynamics is their anti-inflammatory capacity. Suppression of COX-2–derived prostaglandins reduces vasodilation, edema, and leukocyte recruitment at inflamed sites [24,20]. This property differentiates NSAIDs from acetaminophen in conditions where inflammation is a major contributor to pain.
Antipyretic Effects
NSAIDs lower fever by inhibiting prostaglandin E2 synthesis in the hypothalamus, thereby reducing the set-point for body temperature regulation [13].
Adverse Pharmacodynamic Consequences
COX-1 inhibition underlies NSAID-associated gastrointestinal bleeding, while COX-2 inhibition has been linked to cardiovascular risk [25,49,55,57]. Renal impairment results from reduced prostaglandin-mediated renal vasodilation [2,60,65].
11. PHARMACODYNAMICS OF ACETAMINOPHEN
Analgesic Effects
Acetaminophen’s analgesia is mediated centrally via inhibition of prostaglandin synthesis, modulation of serotonergic descending pathways, and cannabinoid/TRPV1 interactions [5,6,22,27]. Clinical evidence supports efficacy in headache, postoperative pain, and osteoarthritis, though often with smaller effect sizes compared to NSAIDs [7,29,38,42,45].
Antipyretic Effects
Similar to NSAIDs, acetaminophen exerts antipyresis by lowering hypothalamic prostaglandin synthesis, making it the drug of choice for fever in children [12,72].
Lack of Anti-inflammatory Activity
Unlike NSAIDs, acetaminophen demonstrates negligible anti-inflammatory action in peripheral tissues, which limits its utility in inflammatory conditions such as rheumatoid arthritis [46].
Adverse Pharmacodynamic Consequences
The principal pharmacodynamic risk of acetaminophen is hepatotoxicity, resulting from accumulation of NAPQI under overdose or chronic alcohol consumption [15,66,71]. Unlike NSAIDs, gastrointestinal and renal adverse effects are minimal at therapeutic doses [52,64].
12. COMPARATIVE PHARMACODYNAMIC INSIGHTS
Acetaminophen’s pharmacodynamics position it as an effective analgesic and antipyretic with minimal anti-inflammatory capacity and a favorable gastrointestinal profile. NSAIDs provide stronger analgesia in inflammation-driven pain states but are burdened by GI, renal, and cardiovascular risks [2,48,49,54,56].
These differences explain clinical guidelines recommending acetaminophen as a first-line option for mild to moderate pain and fever, while reserving NSAIDs for cases where anti-inflammatory efficacy is necessary [23,31,35].
13. CLINICAL APPLICATIONS IN PAIN MANAGEMENT: ACUTE VS. CHRONIC PAIN
Acute Pain: General Considerations
Acute pain, often associated with surgery, trauma, or dental procedures, is commonly managed using NSAIDs and acetaminophen either as monotherapy or in combination. The goals of therapy include rapid onset, effective analgesia, and minimal adverse effects [37,38,41].
NSAIDs are frequently preferred when inflammation is a dominant contributor to nociception, while acetaminophen is selected when gastrointestinal or bleeding risks preclude NSAID use [41].
Postoperative Pain
Postoperative pain is among the most studied domains of analgesic efficacy. Systematic reviews confirm that both NSAIDs and acetaminophen significantly reduce postoperative pain scores, though NSAIDs tend to provide stronger analgesia in surgeries with high inflammatory response [37,38].
A landmark trial demonstrated that combined acetaminophen and ibuprofen was superior to either drug alone for postoperative dental pain, supporting a multimodal analgesic approach [40]. Similarly, guidelines recommend the concurrent use of acetaminophen and NSAIDs for enhanced efficacy and opioid-sparing effects [41,78,80].
Musculoskeletal and Low Back Pain
NSAIDs are widely prescribed for musculoskeletal pain, particularly acute low back pain, with substantial evidence supporting their efficacy [44]. In contrast, high-quality randomized controlled trials (RCTs) have failed to demonstrate significant benefit of acetaminophen in acute low back pain [45].
Meta-analyses suggest that NSAIDs outperform acetaminophen in musculoskeletal pain relief, although acetaminophen retains a role where NSAIDs are contraindicated [42,43].
Osteoarthritis
Osteoarthritis (OA) represents a major cause of chronic pain in aging populations. Historically, acetaminophen was considered a first-line therapy for OA due to its safety profile [7]. However, recent systematic reviews question its efficacy, showing limited clinical benefits compared with placebo [42,45].
In contrast, NSAIDs consistently provide superior analgesia and functional improvement in OA, though at the expense of gastrointestinal, cardiovascular, and renal toxicity [3,34,43]. Updated clinical guidelines now favor NSAIDs as primary pharmacological agents in OA, with acetaminophen recommended only in cases where NSAIDs are contraindicated [23,31,35].
Rheumatoid Arthritis
In rheumatoid arthritis (RA), where inflammation is a central pathological process, NSAIDs are preferred for symptomatic relief. They provide both analgesic and anti-inflammatory benefits but do not alter disease progression [46]. Disease-modifying antirheumatic drugs (DMARDs) remain essential for long-term disease control.
Acetaminophen, due to its lack of anti-inflammatory activity, has limited efficacy in RA management and is rarely recommended as a monotherapy [46].
Headache and Migraine
Both acetaminophen and NSAIDs are widely used in the management of primary headache disorders. Acetaminophen is effective for tension-type headaches, though NSAIDs often provide superior relief [84,87].
In migraine, NSAIDs such as ibuprofen and aspirin are more efficacious than acetaminophen, though acetaminophen remains an option for mild to moderate attacks and in patients with contraindications to NSAIDs [84,86,88]. Fixed-dose combinations of acetaminophen, aspirin, and caffeine have shown superior efficacy over monotherapy [85].
Pediatric Pain and Fever
Acetaminophen remains the most commonly used analgesic and antipyretic in pediatric populations due to its safety, efficacy, and favourable tolerability profile [12,72]. NSAIDs such as ibuprofen are also widely used and may offer longer-lasting antipyresis [10].
In children, acetaminophen is often preferred for simple fever management, while NSAIDs are reserved for inflammatory conditions [72].
Elderly Populations
Older adults are particularly vulnerable to adverse effects of NSAIDs, including gastrointestinal bleeding, renal impairment, and cardiovascular events [76,77]. Acetaminophen, with its superior safety profile, is often recommended as a first-line analgesic in elderly patients [77].
However, the reduced efficacy of acetaminophen in osteoarthritis and musculoskeletal pain in this population limits its utility, necessitating cautious NSAID use or multimodal strategies [31,35].
Cancer Pain and Palliative Care
NSAIDs and acetaminophen are both used as adjuvants in cancer pain management, particularly in mild-to-moderate cases or in combination with opioids [47]. NSAIDs may provide superior benefit in cancer-related bone pain due to their anti-inflammatory action [46].
Acetaminophen remains a valuable adjunct in multimodal regimens, though its ceiling effect in analgesia restricts its efficacy in severe cancer pain [80,82].
Multimodal and Balanced Analgesia
The complementary mechanisms of NSAIDs and acetaminophen provide the rationale for their combination in multimodal analgesia. Evidence demonstrates superior analgesia and reduced opioid consumption when both agents are co-administered [40,78,80,81].
Multimodal strategies are now widely endorsed in postoperative and chronic pain guidelines, reflecting the evolving understanding that no single analgesic can address all aspects of pain [41,82].
14. COMPARATIVE CLINICAL INSIGHTS
Across clinical contexts, NSAIDs generally demonstrate superior efficacy in inflammation-driven pain states such as osteoarthritis, rheumatoid arthritis, and postoperative pain [3,43,46]. Acetaminophen, while less potent, remains indispensable in populations at risk of NSAID-related adverse events, particularly children, the elderly, and patients with gastrointestinal, renal, or cardiovascular comorbidities [12,31,52,72,77].
Combination therapy maximizes efficacy and minimizes opioid requirements, representing a modern standard in pain management [40,78,81].
15. ADVERSE EFFECTS AND SAFETY PROFILES: COMPARATIVE TOXICOLOGY
Gastrointestinal Toxicity
NSAIDs
NSAIDs are strongly associated with gastrointestinal (GI) injury due to inhibition of COX-1–mediated prostaglandin synthesis, which normally protects the gastric mucosa [48]. Adverse effects include dyspepsia, gastric erosions, peptic ulcers, and life-threatening upper GI bleeding [36,49].
Large trials such as the Class Study demonstrated that even selective COX-2 inhibitors, initially marketed as GI-sparing, still carry significant GI risks, though at lower levels compared to nonselective NSAIDs [50]. The risk is dose-dependent and increases with age, Helicobacter pylori infection, alcohol, and concomitant corticosteroid or anticoagulant therapy [36,53].
Acetaminophen
Unlike NSAIDs, acetaminophen does not inhibit gastric prostaglandins and has a much lower incidence of GI adverse effects [52]. Epidemiological studies confirm that acetaminophen users have substantially lower risk of peptic ulcer disease and bleeding compared with NSAID users [36,52].
Cardiovascular Risks
Selective COX-2 inhibitors were developed to reduce GI complications, but their use uncovered significant cardiovascular (CV) risks. The VIGOR and APPROVe trials linked rofecoxib with increased myocardial infarction and stroke risk, ultimately leading to its market withdrawal [25,55]. Other NSAIDs, including diclofenac and high-dose ibuprofen, also increase CV risk, with naproxen considered the safest option [54,56,57].
Mechanistically, inhibition of COX-2–derived prostacyclin without corresponding suppression of thromboxane A2 favors thrombosis and hypertension [54].
Acetaminophen was traditionally considered CV-neutral, but observational studies suggest possible associations with hypertension and coronary disease, particularly at high doses [58,59]. However, the magnitude of risk is generally lower than that of NSAIDs [58].
Renal Toxicity
1.NSAIDs
NSAID nephrotoxicity arises from prostaglandin inhibition, which impairs renal autoregulation, especially in patients with hypovolemia, chronic kidney disease (CKD), or heart failure [2,19,60]. Clinical consequences include acute kidney injury, sodium retention, hypertension, and CKD progression [61–63,65].
2.Acetaminophen
Although less nephrotoxic, acetaminophen is not without renal risks. Chronic use has been linked to analgesic nephropathy and interstitial nephritis, particularly at supratherapeutic doses [64]. Compared to NSAIDs, however, the renal burden of acetaminophen is markedly lower [64].
Hepatotoxicity
1.NSAIDs
Hepatic injury from NSAIDs is relatively rare but documented, with diclofenac among the most hepatotoxic [69,70]. The mechanism involves idiosyncratic immune-mediated reactions and oxidative stress.
2.Acetaminophen
Hepatotoxicity represents the most significant adverse effect of acetaminophen. Overdose leads to saturation of glucuronidation and sulfation pathways, with excess metabolism via CYP2E1 generating NAPQI, a reactive metabolite that depletes glutathione and induces hepatocellular necrosis [15,16,66,67].
Clinical risk factors include fasting, chronic alcohol intake (which induces CYP2E1), and use of enzyme-inducing drugs [66,71]. Acetaminophen toxicity is the leading cause of acute liver failure in many countries [66,73].
Respiratory and Allergic Reactions
1.NSAIDs
NSAIDs may precipitate aspirin-exacerbated respiratory disease (AERD), characterized by asthma, nasal polyps, and rhinosinusitis due to shunting of arachidonic acid metabolism toward leukotriene synthesis [83]. Hypersensitivity reactions, including urticaria and anaphylaxis, are also reported [83].
2.Acetaminophen
Acetaminophen is less commonly associated with allergic or respiratory reactions, though recent epidemiological data suggest an association between early-life acetaminophen exposure and increased asthma risk in children [39]. The mechanism remains uncertain but may involve oxidative stress and immune modulation.
Hematological Effects
1. NSAIDs
By inhibiting platelet thromboxane A2 synthesis, nonselective NSAIDs impair platelet aggregation, prolonging bleeding time [9,20]. This effect is particularly significant with aspirin, which irreversibly acetylates COX-1 and is widely used for antiplatelet therapy [9].
2. Acetaminophen
Acetaminophen does not significantly affect platelet function and is therefore preferred in patients with bleeding risk or perioperative contexts [27].
Special Populations
1.Elderly: NSAID-related GI and renal complications are particularly common; acetaminophen is safer but less effective in osteoarthritis [31,76,77].
2.Pregnancy: Acetaminophen is generally considered safe, though concerns about fetal neurodevelopment persist [39]. NSAIDs, particularly in the third trimester, are contraindicated due to risk of premature ductus arteriosus closure [76].
3. Pediatrics: Acetaminophen is the mainstay of antipyresis, while ibuprofen is safe and effective in selected cases [12,72]. Aspirin is avoided due to risk of Reye’s syndrome [72].
16. COMPARATIVE TOXICOLOGICAL INSIGHTS
The safety profiles of acetaminophen and NSAIDs diverge markedly. NSAIDs carry substantial GI, renal, and cardiovascular risks, particularly in long-term use, while acetaminophen’s major limitation is hepatotoxicity in overdose or chronic misuse [2,36,52,66].
Clinicians must weigh these distinct risks when tailoring therapy to individual patients. Acetaminophen is safer in GI, renal, and hematologic contexts, whereas NSAIDs provide stronger efficacy in inflammatory pain but require vigilant monitoring for adverse effects.
17. CONCLUSION
Acetaminophen and NSAIDs remain cornerstones of pain management worldwide, yet their pharmacological profiles, mechanisms of action, and safety considerations are strikingly different. NSAIDs act primarily by inhibiting COX-1 and COX-2, thereby reducing peripheral prostaglandin synthesis and offering both analgesic and anti-inflammatory benefits. Their utility is maximized in conditions with strong inflammatory components, such as osteoarthritis, rheumatoid arthritis, and postoperative pain. However, NSAIDs carry substantial risks, particularly gastrointestinal, cardiovascular, and renal toxicities.
In contrast, acetaminophen functions mainly as a centrally acting analgesic and antipyretic, exerting its effects through weak central COX inhibition, serotonergic pathway modulation, endocannabinoid reuptake inhibition, and TRPV1 activation. Its lack of peripheral anti-inflammatory action limits its role in inflammatory conditions, but its favorable gastrointestinal and renal safety profile makes it especially valuable in populations where NSAIDs are contraindicated, including children, older adults, and those with cardiovascular comorbidities. Its primary limitation remains hepatotoxicity, particularly in overdose situations.
The complementary nature of these agents underpins the rationale for multimodal analgesia, combining acetaminophen and NSAIDs to maximize efficacy while minimizing opioid reliance. Clinical guidelines now emphasize such strategies, recognizing that no single agent can adequately address all dimensions of pain.
18. FUTURE DIRECTIONS
Future research on acetaminophen and NSAIDs should focus on:
Mechanistic Elucidation of Acetaminophen: Despite decades of use, the precise molecular basis of acetaminophen’s analgesic action remains incompletely understood. Advances in neuropharmacology may clarify the interplay between serotonergic, cannabinoid, and TRP pathways.
Personalized Pain Management: Genetic polymorphisms in drug-metabolizing enzymes (e.g., CYP2C9 for NSAIDs, CYP2E1 for acetaminophen) affect efficacy and toxicity. Pharmacogenomic approaches could refine patient selection and dosing.
Safer Formulations: Development of NSAID formulations with reduced GI and cardiovascular risks (e.g., topical agents, nitric oxide–donating NSAIDs) and acetaminophen derivatives with diminished hepatotoxicity are promising avenues.
Long-term Safety Surveillance: Continued pharmacovigilance is essential, particularly regarding emerging evidence linking acetaminophen with asthma and neurodevelopmental risks, and NSAIDs with cardiovascular morbidity.
Integration into Multimodal Analgesia: Further randomized controlled trials are needed to optimize combination regimens, balancing efficacy with safety across diverse clinical populations.
REFERENCES




Mubitha M., Thamizharasi S., Vaanvizhi S., Veerajothi N., Pandian P.*, Comparative Pharmacological Mechanisms of Acetaminophen and NSAIDs in Pain Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 2014-2023 https://doi.org/10.5281/zenodo.17597790
 10.5281/zenodo.17597790
10.5281/zenodo.17597790
