1,3Department of Pharmaceutical and Medicinal Chemistry, Faculty of Pharmacy, Niger Delta University, Wilberforce Island, Bayelsa, Nigeria.
2,4Drug Analysis and Research Center, Ebisamdex Global Ventures Ltd, Yenagoa, Bayelsa, Nigeria.
This study evaluates the bioequivalence of five ciprofloxacin tablets produced by different manufacturers through an in vitro quality assessment. The physical properties of pharmaceutical formulations are crucial in ensuring product quality, bioavailability, and optimal therapeutic effectiveness. Ciprofloxacin, a commonly prescribed oral and intravenous antibiotic for bacterial infections, was analyzed for weight uniformity, hardness, friability, disintegration, dissolution, and assay following standard methods to verify compliance with USP and BP standards. All tested brands met the official requirements for weight uniformity, hardness (ranging from 7.5 to 10.4 kg), disintegration time (2.67 to 4.6 minutes), and friability (0.031 to 0.45%). The assay results indicated a potency of 94.7% to 105%, and dissolution testing showed 77.7% to 84.7% drug release within 45 minutes, adhering to BP and USP guidelines. The findings confirm that all brands satisfy the quality control criteria set by both pharmacopeias.
Antibiotics represent a crucial class of antimicrobial agents specifically targeting bacterial pathogens, playing a vital role in treating and preventing bacterial infections through either bactericidal (killing) or bacteriostatic (growth-inhibiting) mechanisms [1]. Beyond their primary antibacterial effects, certain antibiotics demonstrate additional antiprotozoal properties [2]. These therapeutic agents are systematically categorized according to their mode of action, chemical composition, or activity spectrum, with most antibiotics functioning by disrupting critical bacterial processes [3]. Bactericidal antibiotics typically attack bacterial cell walls (penicillins, cephalosporins) or cell membranes (polymyxins), or disrupt essential bacterial enzymes (rifamycins, lipiarmycins, quinolones, sulfonamides) [4]. In contrast, protein synthesis inhibitors (macrolides, lincosamides, tetracyclines) generally exhibit bacteriostatic activity, with the notable exception of bactericidal aminoglycosides [5,6]. Ciprofloxacin, chemically known as 1-cyclopropyl-6-fluoro-1,4-dihydro-4-oxo-7-(piperazinyl)-quinolone-3-carboxylic acid, belongs to the quinolones, which are synthetic antibiotics, chemically related to nalidixic acid [7]. Almost all clinically useful quinolones bear a fluorine atom in the C-6 position and thus, these antibacterial agents are called fluoroquinolones [7,8].
Figure 1. Structure Ciprofloxacin.
Quinolones demonstrate broad-spectrum antibacterial activity against both gram-positive and gram-negative organisms by specifically targeting DNA gyrase, an essential enzyme for bacterial DNA replication [10]. Ciprofloxacin, a prominent quinolone antibiotic, exhibits clinical efficacy against diverse infections, including gastrointestinal, urinary tract, respiratory, ocular, skin, and intra-abdominal infections (when combined with anti-anaerobic agents) [11,12]. This versatile agent is formulated in multiple dosage forms, including immediate/extended-release tablets, oral suspension, and intravenous solution. While IV administration achieves rapid tissue distribution, cerebrospinal fluid penetration remains limited (<10% of serum concentrations) [13]. The drug exhibits a moderate elimination half-life of 4-6 hours, with 50-70% excreted renally as unchanged drug. Despite relatively low protein binding (20-40%), ciprofloxacin demonstrates significant CYP1A2 inhibition, potentially leading to clinically relevant drug interactions [14]. Oral formulations show approximately 70% bioavailability, necessitating slightly higher dosing compared to intravenous administration to achieve equivalent therapeutic effects [15]. Extended-release (XR) tablets (35% immediate, 65% slow-release) allow once-daily dosing, achieving peak levels in 1–4 hours. The 500mg/1000mg XR tablets yield higher Cmax but equivalent AUC to 250mg/500mg immediate-release tablets. Both formulations use ciprofloxacin hydrochloride, with XR tablets also containing the free base. Urinary excretion is nearly complete within 24 hours [16]. Substandard drugs pose serious global health risks as they contain incorrect ingredients or dosages, rendering them ineffective or dangerous. Counterfeit drugs may have fake packaging, incorrect ingredients, or insufficient active compounds, often causing greater harm than substandard ones. These drugs contribute to several illnesses, death, and eroded trust in healthcare systems [17]. According to the World Health Organization (WHO), around 10% of pharmaceuticals worldwide are counterfeit, with the figure rising to 25% in developing countries and surpassing 50% in certain areas [18]. The U.S. Food and Drug Administration [19] similarly notes that up to a quarter of drugs in low-income nations are either fake or of poor quality, often originating from countries like China and India. Instances of drug-related poisoning have been reported, including a 2009 case in Bangladesh where contaminated paracetamol syrup led to the deaths of 25 children, and an incident in the U.S. between 2007 and 2008 where adulterated heparin was linked to 149 fatalities [20]. The WHO also found that 28% of antibiotics and 20–90% of antimalarials failed quality tests [18]. Despite these risks, generic drugs remain crucial for affordable healthcare. Generics must meet strict regulatory standards, ensuring therapeutic equivalence to brand-name drugs to balance safety, efficacy, and accessibility in global medicine. Bioequivalence indicates that a generic drug and its reference counterpart or innovator brand are absorbed into the bloodstream at a comparable rate and extent [21,22,23]. Bioequivalence studies are typically conducted to confirm that the generic drug is absorbed at the same rate as the reference product [24,25]. Several studies on ciprofloxacin HCl have evaluated compliance with the Pharmacopoeial standards to confirm that tested brands of ciprofloxacin HCL met required specifications. These studies reported that most leading brands satisfied quality control parameters, though 4 brands were reported to fail dissolution tests [26]. In vitro testing allows for precise and detailed analysis of drug characteristics that cannot be easily studied in whole organisms [27,28,29]. Such studies on ciprofloxacin help determine its in vivo behavior, safety, efficacy, and overall quality. The current study aims to ascertain the in vitro pharma-equivalence of 4 different generic brands of ciprofloxacin tablets and compare them with an innovator brand.
METHODS
Sample collection
Both the generic and innovator brands of ciprofloxacin HCl were procured from registered pharmacies in Yenagoa District, Bayelsa, Nigeria.
Physicochemical Analysis
|
Test |
Procedure |
|
Weight Variation
|
Twenty tablets from each brand were weighed using an analytical balance to determine the average tablet weight, which was then compared with the individual tablet weights. |
|
Hardness |
Tablet hardness was assessed using the standard compression method with a Monsanto hardness tester, where each tablet was placed between two jaws and crushed to measure its resistance. |
|
Friability |
Friability testing involved placing 20 tablets from each brand in a friabilator, where they were subjected to rolling and repeated drops of 6 inches per rotation for four minutes. The tablets were weighed before and after the test to assess weight loss. |
|
Disintegration
|
Disintegration time was measured using a Veego disintegration tester. Tablets were placed in individual tubes, and the basket rack was immersed in 400 mL of 0.1N hydrochloric acid at 37°C. The time taken for each tablet to fully disintegrate was recorded for each brand. |
Serial dilution and in vitro dissolution
Assessing drug potency in tablets is vital to confirm the strength and amount of the active ingredient in each dosage form. In this study, a standard ciprofloxacin HCl stock solution was prepared by dissolving 100 mg of the pure compound in 0.1N HCl and diluting it to 100 mL to obtain a 1000 µg/mL concentration. A secondary stock solution (100 µg/mL) was made by diluting 10 mL of the primary solution to 100 mL, followed by further dilutions to create calibration standards at concentrations of 0.5, 1, 2, 5, and 10 µg/mL. The absorbance of each standard was measured at 276 nm using a UV spectrophotometer, and a calibration curve was plotted with absorbance on the Y-axis and concentration on the X-axis. For tablet evaluation, samples from different brands were finely ground, and a portion equivalent to 100 mg of ciprofloxacin was dissolved in 100 mL of 0.1N HCl to produce a 100 µg/mL solution. This solution was further diluted by taking 4 mL and making it up to 100 mL with 0.1N HCl. The absorbance of each sample was measured at 276 nm against a blank. According to Pharmacopeial guidelines, ciprofloxacin HCl content must fall within 90–110% of the labeled amount per the USP-NF, and 95–105% as per the British Pharmacopoeia [30]. Dissolution testing for all ciprofloxacin generic formulations was conducted using a basket-type dissolution apparatus (Veego), set at 37 ± 0.5°C with a rotation speed of 100 rpm. The dissolution medium consisted of 1000 mL of 0.1N HCl, maintained for one hour. At specified intervals, 5 mL samples were withdrawn through a 0.8 µm syringe filter and replaced with an equal volume of fresh medium. The concentration of the dissolved drug was analyzed on a UV/Visible spectrophotometer at 276 nm.
RESULT
The results obtained from the analysis are presented in frequency, percentage tables, and charts.
Table 1. Weight, percentage deviation, and standard deviation of the various Ciprofloxacin HCl brands
|
Tablets |
A |
B |
C |
D |
E |
|||||
|
Kg |
% D |
Kg |
% D |
Kg |
% D |
Kg |
% D |
Kg |
% D |
|
|
1 |
0.784 |
0.8 |
0.735 |
1.8 |
0.716 |
7.5 |
0.746 |
0.5 |
0.677 |
0 |
|
2 |
0.772 |
0.8 |
0.727 |
0.7 |
0.675 |
1.5 |
0.754 |
0.5 |
0.674 |
0.4 |
|
3 |
0.773 |
0.6 |
0.682 |
5.5 |
0.661 |
0.6 |
0.755 |
0.6 |
0.681 |
0.6 |
|
4 |
0.777 |
0.1 |
0.725 |
0.1 |
0.646 |
2.9 |
0.750 |
0 |
0.670 |
1.0 |
|
5 |
0.776 |
0.3 |
0.740 |
2.5 |
0.665 |
0 |
0.745 |
0.6 |
0.681 |
0.6 |
|
6 |
0.776 |
0.3 |
0.724 |
0.3 |
0.647 |
2.7 |
0.749 |
0.1 |
0.683 |
0.9 |
|
7 |
0.781 |
0.4 |
0.740 |
2.5 |
0.682 |
2.4 |
0.748 |
0.3 |
0.673 |
0.5 |
|
8 |
0.781 |
0.4 |
0.721 |
2.5 |
0.666 |
0.2 |
0.750 |
0 |
0.670 |
1.0 |
|
9 |
0.779 |
0.1 |
0.709 |
0.1 |
0.649 |
2.4 |
0.758 |
1.1 |
0.676 |
0.1 |
|
10 |
0.775 |
0.4 |
0.722 |
1.8 |
0.633 |
4.8 |
0.742 |
0.8 |
0.672 |
0.1 |
|
11 |
0.782 |
0.5 |
0.689 |
0 |
0.672 |
1.1 |
0.744 |
0.1 |
0.670 |
0.7 |
|
12 |
0.771 |
0.9 |
0.723 |
4.6 |
0.650 |
2.3 |
0.742 |
1.3 |
0.684 |
1.0 |
|
13 |
0.783 |
0.6 |
0.717 |
0.1 |
0.664 |
0.2 |
0.749 |
0.9 |
0.675 |
1.0 |
|
14 |
0.780 |
0.3 |
0.727 |
0.9 |
0.679 |
2.1 |
0.740 |
1.1 |
0.669 |
0.3 |
|
15 |
0.770 |
1.0 |
0.739 |
0.7 |
0.665 |
0 |
0.743 |
1.3 |
0.682 |
1.2 |
|
16 |
0.781 |
0.4 |
0.720 |
0.4 |
0.667 |
0.3 |
0.742 |
0.1 |
0.679 |
0.7 |
|
17 |
0.782 |
0.5 |
0.737 |
0.3 |
0.681 |
2.4 |
0.740 |
0.4 |
0.677 |
0.3 |
|
18 |
0.779 |
0.1 |
0.735 |
2.0 |
0.658 |
1.1 |
0.743 |
0.9 |
0.683 |
0 |
|
19 |
0.787 |
1.1 |
0.710 |
1.8 |
0.647 |
2.8 |
0.747 |
1.0 |
0.674 |
0.9 |
|
20 |
0.776 |
0.3 |
0.709 |
0.9 |
0.069 |
0.6 |
0.746 |
0.5 |
0.686 |
0.4 |
|
Mean ± SD |
0.778±0.3 |
0.7212±1.3 |
0.665±1.8 |
0.750±0.4 |
0.677±0.4 |
|||||
SD = Standard Deviation, % D = Percentage Deviation

Figure 2. Hardness of Various Brands, Mean & Standard Deviation. The ANOVA of the Hardness of Various Brands was statistically significant with a p-value of <0.0001. Data are presented as mean and standard deviation from 10 different runs.

Figure 3. Percentage (%) Friability. Samples A to E.
Table 2. Disintegration Time
|
S/N |
A |
B |
C |
D |
E |
|
1 |
1.28 |
1.33 |
2.27 |
1.30 |
3.30 |
|
2 |
1.34 |
1.39 |
2.56 |
1.36 |
4.12 |
|
3 |
1.38 |
2.04 |
3.04 |
1.43 |
4.25 |
|
4 |
1.42 |
2.07 |
3.04 |
1.58 |
4.25 |
|
5 |
1.50 |
2.13 |
3.20 |
2.00 |
5.16 |
|
6 |
1.50 |
2.44 |
3.20 |
2.02 |
5.47 |
|
Mean ± SD |
1.38±0.3 |
1.87±1.0 |
3.12±0.3 |
1.26±0.2 |
5.29±0.7 |
Table 3. Percentage Drug Release
|
S/N |
Time (mins) |
A (%) |
B (%) |
C (%) |
D (%) |
E (%) |
|
1 |
5 |
28.25 |
23.40 |
29.55 |
5.80 |
26.13 |
|
2 |
10 |
34.76 |
24.232 |
52.54 |
38.48 |
42.75 |
|
3 |
15 |
40.85 |
30.784 |
55.58 |
40.57 |
45.98 |
|
4 |
20 |
63.11 |
33.591 |
76.00 |
44.94 |
53.11 |
|
5 |
30 |
85.31 |
47.22 |
82.94 |
53.39 |
83.70 |
|
6 |
45 |
77.70 |
83.51 |
84.65 |
87.31 |
9.58 |
|
7 |
60 |
89.36 |
97.87 |
91.00 |
87.78 |
92.44 |
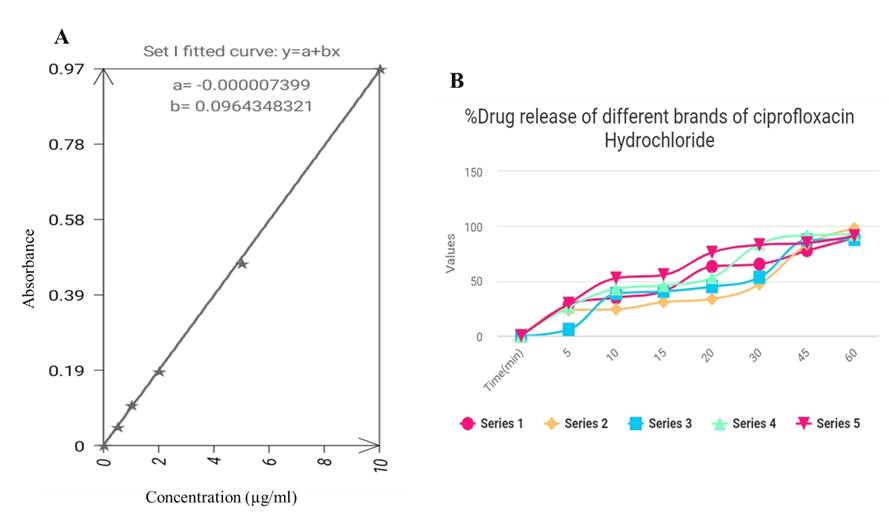
Figure 5. (A) Calibration curve of ciprofloxacin HCl powder. (B) Dissolution rate.
DISCUSSION
This study demonstrates that consistent quality in pharmaceutical dosage forms results from rigorous quality control measures rather than chance occurrences. The concept of bioequivalence is essential for determining therapeutic interchangeability between drug products, particularly in developing countries where pharmaceutical quality may be inconsistent [26]. All tested ciprofloxacin brands complied with the Pharmacopoeial standards for weight uniformity. The USP permits up to 10% deviation from average tablet weight, while BP standards allow only 5% variation [30,31]. The highest observed standard deviation was 1.8 (Brand C), confirming manufacturing consistency. Friability testing, which assesses tablet durability during production and handling, yielded values between 0.031% and 0.45%—well below the USP's 1% limit (Figure 3). This is critical because excessive friability can lead to weight variations and potential therapeutic inconsistencies [26]. Tablet hardness, an indicator of structural integrity, ranged from 7.2 to 10.4 kg (SD: 0.21–1.01), meeting compendial requirements (Figure 2). These findings align with previous bioequivalence studies on ciprofloxacin brands in the Nigerian market [31]. Disintegration times (1.80–4.6 minutes) were significantly faster than BP recommended 5-minute limits and that of the USP 30-minute standards (Table 2). Dissolution profiles showed 77.7%–82.9% drug release within 45 minutes, satisfying both BP (≥80%) and USP-NF (≥75%) criteria (Table 3). UV spectrophotometric analysis confirmed drug content uniformity (94.7%–105%) (Figure 5A), complying with Pharmacopeial specifications. These in vitro results suggest pharmaceutical equivalence between generic and innovator ciprofloxacin products. While the data support interchangeability, in vivo studies are recommended to confirm bioequivalence conclusively (Ebeshi et al., 2025). The findings affirm that these generics meet quality standards for proper drug release, absorption, and therapeutic efficacy.
CONCLUSION
All tested tablets demonstrated consistent hardness, uniform weight, and compliance with USP standards for friability, dissolution, and disintegration. These results confirm that the various brands of Ciprofloxacin HCl meet established Pharmacopeial specifications, indicating their structural stability, pharmaceutical integrity, and potential bioequivalence. The findings suggest that these formulations will disintegrate effectively in the gastrointestinal tract (GIT), ensuring adequate drug release and subsequent absorption to achieve the intended therapeutic response. While the study confirms that the generic ciprofloxacin hydrochloride brands evaluated exhibit comparable in vitro performance to the innovator product, further in vivo studies are necessary to definitively establish their bioequivalence. Nevertheless, the current data support the possibility of interchangeability among these brands in clinical practice.
REFERENCES


Adesegun J. Kashimawo*, Betty O. Abraham, Samuel J. Bunu, Ciprofloxacin Hydrochloride Oral Formulations In Vitro Evaluation for Pharmaceutical Equivalence, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 21-29 https://doi.org/10.5281/zenodo.17015605
 10.5281/zenodo.17015605
10.5281/zenodo.17015605
