Shivajirao S. Jondhle college of pharmacy, Asangaon, India
Cancer vaccines represent a promising approach in cancer immunotherapy aimed at stimulating the immune system to recognize and eliminate tumor cells. Despite early challenges and limited clinical success, recent advances in tumor genomics, antigen discovery, and vaccine technologies have significantly improved their potential. Personalized vaccines, neoantigen targeting, and mRNA-based platforms offer improved specificity and adaptability to tumor heterogeneity. The use of cancer vaccines in combination with other therapies and in early-stage or adjuvant settings further enhances their effectiveness. Although challenges remain, ongoing research suggests that cancer vaccines may play a vital role in future precision cancer treatment strategies.
Cancer
Cancer is a mysterious and deadly disease of the genome. It is characterized by a genomic instability where a large number of point mutations accumulate and structural alterations occur as the tumour develops in. [1,2]The initial indications of cancer are genetic and epigenetic alterations in specific cells, some of which can spread and migrate to other organs. [3]
Inflammation is a key element of pathophysiology. Cancer can cause inflammation, and inflammation can encourage cancer growth. A malignant tumor is a colony of cells that can penetrate and spread, grow more often than normal tissue, and multiply uncontrollably. [4] Cancer has been present in multicellular species for more than 200 million years, and there is proof that our ancestors had the disease for more than a million years. [1]
There have been several instances of genetic anomalies that could alter normal human cells and I cad to the growth of tumors and cancer. [5]
The primary causes of cancer are mutations that result from anomalies in DNA replication, environmental factors, or inheritance. Aging is the main risk factor for carcinogenesis in humans and other multicellular animals.[6]
Globally cancer is second major cause of human mortality. In fact, cancer has become more common overall; by 2025 6,18,120 individuals had died from the disease in the United States alone. where it affected over 20,41,910 people. Cancer is therefore a severe issue that has an impact on the wellbeing of all human cultures. Nearly 10 million cancer deaths occurred worldwide in 2020, according to the World Health Organization, and these numbers are predicted to increase as the population ages and grows.
In men, the prostate, colon and rectum, lung and bronchus, and bladder have the largest percentage of cancer kinds. Among women, cancer is most prevalent in the breast, lung and bronchus, colon and rectum, uterine corpus, and thyroid regions. According to this data, a significant percentage of cancers in men and women are caused by prostate and breast cancer, respectively. [7] Blood cancer, brain cancer, and lymph node cancer are the three cancer kinds that affect youngsters the most frequently.[8,9]
Conventional methods for treatment of Cancer
A considerable portion of cancer cases can be avoided by taking steps including limiting tobacco use, immunization, early detection, and promoting healthy lifestyles[10]. The best source of anti-cancer medications is the kingdom of plants. Over 3.000 plant species have been used in cancer treatment and clinical studies to date, and about 30 distinct anti-cancer natural mixtures have been isolated from plants[6].
In recent decades, medical professionals have discovered more efficient ways to treat it as well as improved techniques for early identification of this terrible illness. However, a cancer cure is 1 years away, and many scientists believe it is unattainable. There are various methods for treating cancer, even though early identification is the best way to prevent it. Among these strategies are:
Overall, incidence and mortality rates for all four types of cancer in both men and women have steadily declined, with the exception of lung cancer in women. This is likely due to improvements in therapy and combination therapies (surgery, radiotherapy, chemotherapy, and, more recently, targeted therapy) as well as an increase in early diagnosis. However, despite these positive developments, cancer remains a significant global public health issue that calls for innovative approaches and therapeutic approaches to improve patient outcomes.
The need for more effective cancer treatment methods Is highlighted by the significant toxicity and limited applicability of conventional cancer therapies. [11]
Cancer Vaccines
When most people hear the phrase "vaccine," they think of shots that protect against bacteria and viruses in particular. These vaccines have been shielding humanity from deadly illnesses for a long time. [12] To prevent or lessen the severity of infectious diseases that can be fatal is the goal of a vaccination prophylactic vaccines). Vaccines frequently produce memory over extended periods of time. [13]. Monoclonal antibodies are currently used in the majority of authorized cancer immunotherapies, however anticancer vaccines are still gaining popularity.[14]
History of cancer vaccines
There are both therapeutic and preventive vaccinations as excellent cancer immunotherapy approaches. The former aims to prevent illness from a specific malignancy by vaccinating healthy individuals in order to induce immunological memory. Despite years of research and development efforts by numerous academics, the clinical application of cancer vaccines has encountered significant obstacles
The first record of cancer immunotherapy dates back to the 1890s, when Dr. William B. Coley used streptococcal organisms (Coley's toxin) as a therapeutic vaccine in sarcoma patients. [15]Further, Bacillus Calmette Guerin has long been used as a vaccine against tuberculosis and is being widely utilized as a therapeutic vaccination against bladder cancer. [16, 17]
Types of Cancer vaccines
Anticancer vaccinations can be both remedial and precuationary. The former type seeks to lower the chance of getting cancer. Vaccines against hepatitis B contagion (HBV) and mortal papillomavirus (HPV) are essential anticancer preventative measures. Remedial vaccinations increase vulnerable cells cytotoxic response by promoting their anticancer rates. Remedial vaccinations in discrepancy to the former group, seek to exclude cancer that formerly exists. Multitudinous remedial cancer vaccines have been created over time.

Figure 1. Different types of cancer vaccine
1) Cell based cancer vaccines
The basis of therapeutic cell based vaccines is the in vitro activation of APCs (such as DCs or NK cells) by genes, viral peptides, or genetically altered tumor cells (dead tumor cells). Tumor cell vaccines and immune cell vaccines are two categories of cell-based vaccines. [18] The entire tumor cell serves as the source of the vaccine in tumor cell vaccines, which include full TAAS, including the epitopes of CD4+ and Cd8-T lymphocytes. Clinical trials for whole-cell cancer vaccines are presently underway. In addition to removing the need to find the perfect target a antigen using whole tumor cells as a vaccine that contains all potential antigens rather than protein/peptide e tumor antigens also allows for the simultaneous targeting of multiple tumor antigens, which would subsequently trigger additional immune responses to more tumor cells. [19, 20] Vaccines utilizing autologous (patient-specific) or allogeneic (non-patient-specific) tumor cells are the first crucial distinction. Second, these cells can be left unaltered, altered to express MHC, costimulatory molecules, or cytokines, or combined with adjuvants like Bacille Calmette-Guerin (BCG) and GM-CSF. Third, these cells can be utilized to create tumor-cell lysates. [21] Since this vaccination makes use of tumor cells, it may be able to generate T cells that are specific to any antigen that the cells express. However, this strategy's drawback is that it might occasionally he challenging to gather a sufficient number of cells[22-25].
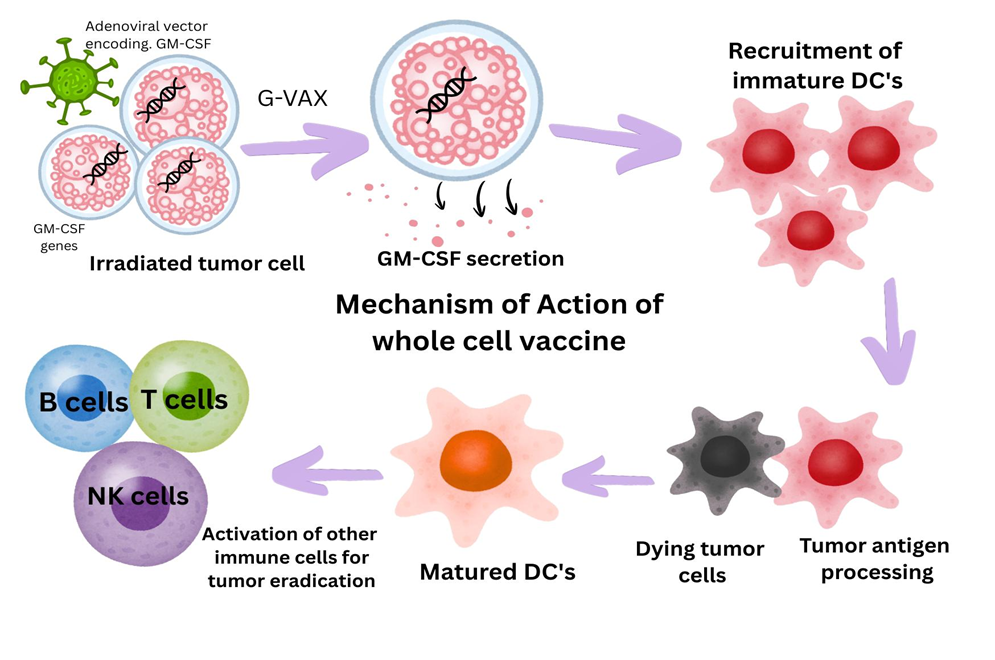
Figure 2: Mechanism of action of Cell based Cancer Vaccines
DC's that convey antigens to T cells and encourage immune system activation are the subject of a novel therapeutic strategy. Since the late 1990s, DC therapy has been thoroughly researched.[26] When DC's were discovered, Dr. Ralph M. Steinman saw their potential and that DCs may be used as a vaccine.[27] DCs may be loaded with a range of antigens, such as tumor cells, proteins or peptides originating from tumours, and DNA/RNA/virus, could be potentially loaded on DCs. There are additional methods, such as the fusion of DCs with tumor cells. Different types of receptors are present on the surface of dendritic cells (DCs). For example, binding of an antigen to a lectin-like receptor known as scavenger receptor on DCs is reported to induce antigen-specific suppressive CD4(+) T cells. It is noteworthy that not all antigen presentation by DCs contributes to immune activation[28].
GVAX is a cancer vaccine that uses tumor cells that have been genetically altered to release GM CSF. It is used to stop the unchecked proliferation of cancer cells following cancer radiotherapy. GM-CSF secretion and patient prognosis have been positively correlated in GVAX phase 1/2 clinical studies for patients with non-small-cell lung cancer[29].However, phase 3 clinical trials for prostate cancer have not shown any effects. [30].
With encouraging outcomes, a number of phase 2 trials of GVAX therapy for advanced pancreatic cancer have been carried out in conjunction with body radiation, cyclophosphamide (CY), or the mesothelin expressing Listeria monocytogenes vaccination. A combination approach utilizing allogeneic GVAX against metastatic castration-resistant prostate cancer (CRPC) and an immune checkpoint inhibitor is being investigated, despite the fact that homologous GVAX against CRPC did not meet its phase 3 clinical trial objectives. [31, 32]
Autologous irradiation tumor cells, either with or without BCG as an adjuvant, make up OncoV AX (Vaccinogen). 254 patients with stage II and III colon cancer were randomly assigned to und ergo OncoVAX or no adjuvant treatment following curative removal of the main tumor in a multi- canter phase III clinical trial. [33]
Compared to the control group, patients receiving OncoVAX had a 20.4% lower risk of disease progression throughout the 5.8-year median follow up. A statistically significant improvement in recurrence free survival in stage Il was found with a 41.4% decrease in the relative risk of disease progression (P.018) in the OncoVAX . However, analysis by stage revealed no meaningful benefit of OncoVAX in stage III disease. With a relative risk reduction of 11.1% for all patients and 33.3% for stage Il patient the OS rate for the OncoVax-treated group was higher than that of the control group. [34]
DC cancer vaccines are an essential subset of cellular cancer vaccines because of their potent immunogenicity and excellent anti-gen-presenting properties. Neoantigenic cancer vaccines based on personalized DC have recently shown significant anti-tumor activity in clinical settings. [35-37] For example, patient-derived leukocytes activated in vitro with mesenchymal DC's and a GM-CSF-linked prostatic acid phosphatase (PAP) antigen produce sipuleucel-T, which was licensed by the FDA in 2010 for metastatic castration-resistant prostate cancer (mCRPC). Sipuleucel-T showed a median OS of 25.8 months compared to 21.7 months in the placebo group in the phase III IMPACT study, which included 512 mCRPC patients [38].
Another autologous tumor lysate-loaded DC vaccine is DCVax L which is noteworthy for its ability to optimize antigen presentation by using tumor lysates to target a broad antigenic library [39,40,41]. In a phase III trial with patients with recurrent gliomas (r GBM) and newly diagnosed gliomas (nGBM), it demonstrated encouraging efficacy. In particular. among nGBM patients, the median OS was 19.3 months for the DCVax-L group and 16.5 months for the placebo group, with 5-year survival rates of 13.0% and 5,7%, respectively. Furthermore, compared to patients receiving standard medication, those treated with DCVax-L showed a 20% relative reduction in mortality risk over time. The DCVax-L group's median OS for rGBM patients was 13.2 months, while the placebo group's was 7.8 months.[42]
2) Vaccines based on viral Or bacterial vectors
Developing a way to overcome the host’s typically weak immune response against TAAS is one of the main challenges in cancer immunotherapy, as was previously discussed. Recombinant genes, such as those that express TAAs, costimulatory molecules, or cytokines, can be introduced into APCs using a variety of vectors Vaccines based on recombinant vectors may cause the immune system to produce a potent inflammatory response that is primarily focused on vector proteins. An enhanced immune response to the target genes placed into the vector may follow from this inflammatory reaction. One benefit of delivering a recombinant protein using vectors is that it is far more immunogenic than delivering the protein with adjuvants.[43, 44] Yeast, bacterial, and viral vectors are employed in cancer immunotherapy. Because each vector has unique properties and may be able to stimulate the host immune system in a different way, the choice of vector can have significant effects on the ensuing immunological response against TAAs.
Viral based vaccines
i) Oncogenic virus vaccines, ii)oncolytic viruses (OVs)and iii) replication defective viral vector vaccines are the three primary categories of virus based immunizations.
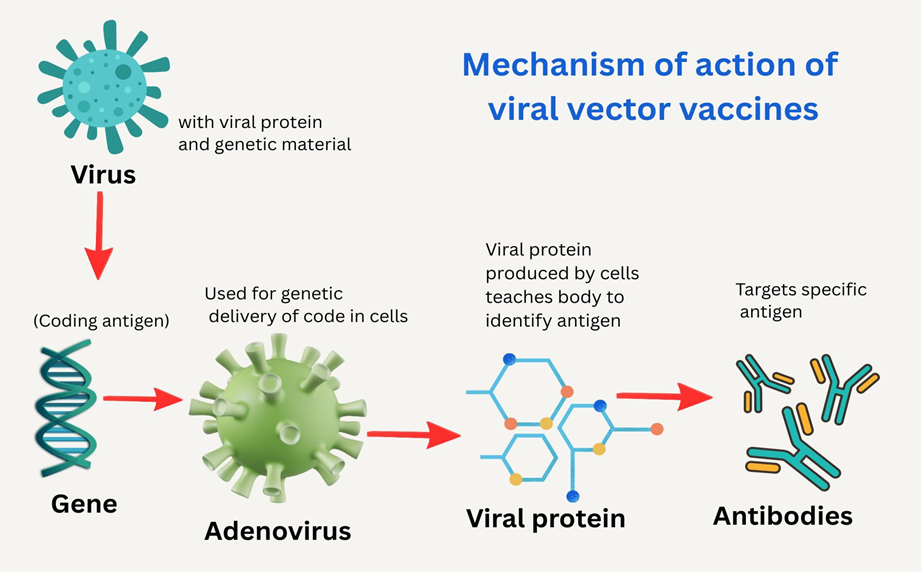
Figure 3: Mechanism of action of Viral vector vaccines
i) Oncogenic virus vaccines
Inactivated virus, live attenuated virus, viral subunits, and VLPs are among the various kinds of oncogenic virus based vaccines that are mainly employed in prophylactic contexts. While inactivated viruses are safer but less successful in eliciting cellular immune responses, live attenuated viruses are highly immunogenic but carry hazards of virulence reversal and illness causation in immunocompromised patients.[45]
Gardasil, Gardasil 9, Cervarix, and Cecolin, which target the HPV L1 epitope, and EngerixB. Recombivax HB, HeplisavB, and PreHevbrio, which target the HBV, are now authorized prophylactic VLP-based cancer vaccines available on market. [46,47] VIP vaccinations may be used to treat melanoma and HER2positive breast cancer, according to recent research. In a mouse model of HER2+ mammary cancer, the human HER2 vaccine candidate ES2B-C001 demonstrated potent anti-tumor effectiveness, reaching a 70% tumor-free rate and total suppression of lung metastases [48].
Preclinical experiments with CMP 001 in situ immunization have demonstrated encouraging tumor control[49]. In patients with metastatic melanoma, a phase II clinical trial found that CMP001 with pembrolizumab was well tolerated and produced 1800RR.[50] One problem with viral vectors is that they may express highly immunogenic epitopes, which could prevent some CTL responses against targeted tumor antigens[51]. Additionally, using alternative vectors or heterologous regimens can address the neutralizing anti-bodies that viral vectors can elicit, which prevent the repeated use of the same vector. [52]
ii) Replication-defective viral vector-based vaccines.
Target proteins are introduced into the host by replication-defective viral vectors When coupled with standard treatment, TG4010, a modified vaccinia Ankara (MVA) strain vaccine expressing MUC1 and IL2, significantly improved OS (12.6 vs. 10.6 months) and PFS (5.9 vs 5.1 months) in patients with advanced non small cell lung cancer. [53.54]
In a phase III experiment, Nanofaragene firadenovec, an Ad vaccine that delivers IFNA2B to b ladder epithelial cells, produced 53.4% CR within three months of the initial injection, with 45.5 % sustaining response at twelve months [55]. This resulted in its FDA approval in 2022 for the treatment of non-muscle invasive bladder cancer that is not responsive to Bacille Calmette-Guérin (BCG).[56]
Novel approaches have been investigated, such as combination immunizations and heterologous regimens. Research has shown that administering numerous virus vaccines at the same time was both safe and immunogenic. [57, 58]
In a phase II trial of patients with metastatic castration resistant prostate cancer PROSTVAC-VF, a heterologous prime boost regimen using recombinant vaccinia and fowlpox viruses expressing prostate specific antigen (PSA) along with three T-cell costimulatory molecules (B7.1, leukocyte function-associated antigen-3, and intercellular adhesion molecule-1) plus GM-CSF, increased the three-year OS rate (30% vs. 17%) and prolonged PFS or detectable PSA. [59] Because there was no improvement in OS or event free survival the subsequent phase III trial was terminated early. [60] These findings show that replication-defective viral vector-based cancer vaccines hold potential but need continued exploration to optimize their effectiveness.
iii) Oncolytic virus vaccines
OV vaccines use a natural ability to proliferate in and kill tumor cells, offering a more aggressive but possibly more successful strategy than replication-defective vaccinations, which provide safety by preventing virus replication.[61] Natural viruses are frequently genetically modified by removing unnecessary viral genes and adding target genes, such as cytokines and tumor antigens, to improve tumor targeting and decrease viral pathogenicity. To strengthen anti-tumor immunity, immuno modulatory substances such as GM-CSF, IL-2, IL-18, IFN-y, and TNF-a have been added to OVs either separately or in combination.[62,63] Four OV vaccines have been authorized thus far for advanced cancer: DELYTACT in 2021, talimogene laherparepvec (T-VEC) in 2015, Rigvir in 2004, and 11101 in 2005. [64]
Although it is not commonly used, rigvir, an unaltered ECHO-7 enterovirus, was approved for melanoma in a number of European nations. Two post-marketing trials revealed that patients with early stage melanoma had longer survival times[65]
H101, an E1B-deleted adenovirus, was approved in China for nasopharyngeal carcinoma after achieving a 78.8% ORR in combination with chemotherapy as opposed to 39.6% with chemotherapy alone. [66] The FDA approved the OV vaccine in 2015 after T-VEC, an attenuated HSV-1 expressing GM CSF improved median OS(23.3 vs. 18 months) in patients with incurable melanoma. [67,68]
DELYTACT has proven to be effective in treating gliomas. In 12 juvenile patients with recurrent or progressive high-grade glioma, G207, a modified HSV-I with deletions in y34.5 and ICP6, extended the median OS (12.2 vs. 5.6 months) [69]. The third generation HSV1 vaccine Delytact which was created by removing the a47 gene from parental G207, has been authorized in Japan for the treatment of malignant glioma and may be effective against a number of solid tumors. [70,71]
Bacterial based vaccines
Traditionally created to prevent infectious diseases, bacteria-based vaccinations have recently surfaced as novel ways to elicit anti-cancer immune responses. Bacillus Calmette-Guérin (BCG) is a prominent example. Originally created as a tuberculosis vaccine, BCG is currently a licensed attenuated bacteria-based immunotherapy (Mycobacterium bovis) for the treatment of bladder cancer that is not muscle invasive. [72,73]
William B. Coley invented the use of microbes for cancer immunotherapy in the late 19 century [74]. Since then, it has been documented that a number of bacteria specifically colonize tumors and cause immune reactions [75,76]. Furthermore, a range of pathogen-associated molecular patterns (PAMPs) that might elicit immune responses are present in bacteria and their derivatives [77]. Additionally, bacteria can be readily altered and loaded with tumor antigens [78]. Bacteria are a viable platform for anti-cancer vaccine methods because of these features [79] Additionally, another intriguing platform for cancer vaccines is the integration of tumor antigens into bacterial outer membrane vesicles (OMVs) that the host immune system can identify.[80-83]
However, despite their potential, biosafety issues and the absence of standardized production methods now restrict the clinical translation of bacteria-based immunotherapy [76].
3) Peptide/protein vaccines.
Immunity against particular antigenic epitopes obtained from the vaccinated protein or peptides that are expressed in cancer cells (and ideally not expressed in normal tissues) can be induced by protein/peptide vaccines. When a synthetic antigen protein or peptide is given, professional APC absorb artificially produced antigen proteins or peptides and present them in combination with the HLA molecules on the cell surface. Immune responses specific to malignancy are triggered when T cells identify the antigens. Numerous antigenic epitopes that can bind HLA and are generated from tumor-associated antigens (TAAs) have been found. Furthermore, neoantigens-antigens produced from cancer-specific gene alterations that are absent from normal tissues-have recently gained interest.[84-86]
Peptide-based cancer vaccines are very stable, inexpensive to produce, and less harmful. However, they have a number of drawbacks, including as poor immunogenicity, short half-life, degradation susceptibility, and—most importantly—HLA restriction.[87]

Figure 4 : Mechanism of action of Peptide based Vaccines
In patients with resected colorectal adenoma, a mucin 1 (MUCI) peptide vaccination combined with poly ICLC produced strong immune responses but was unable to stop recurrence[88]. Similarly, in patients with metastatic or advanced renal cell carcinoma, adding a ten-peptide vaccination with GM-CSF to first-line sunitinib significantly raised the number of CD8+ T cells but did not result in clinical benefits. [89]
In an early phase II trial, OSE2101, which consists of nine peptides that target five TAAs and a pan-DR T helper cell epitope, produced a median survival of 17.3 months in patients with advanced non-small cell lung cancer (NSCLC) [90]. OSE2101 monotherapy later showed superior safety and efficacy over conventional chemotherapy in a larger phase III clinical trial, considerably extending median OS (11.1 vs. 7.5 months) and postprogression survival (7.7 vs. 4.6 months) in patients with secondary immunotherapy resistance. [91]
A number of peptide-based breast cancer vaccines, including the HER2 targeting E75, GP2, and AE37 vaccines, have been thoroughly studied and shown to have therapeutic potential [92, 93]. In a phase II clinical trial, the E75 vaccination decreased the recurrence r ate in patients with breast cancer; however, in a subsequent phase III trial, the primary survival endpoint was not met. [94,95]Additionally, in high-risk HER2 low expressing breast cancer, the E75 vaccination plus trastuzumab did not increase disease-free survival (DFS)[96]. However, sub-group analyses suggested that individuals with HILA-positive or triple-negative breast cancer (TNBC) might benefit [92,97]
In patients with metastatic melanoma who were not yet receiving anti-PD-1 therapy, 10102-10103, a bispecific vaccination that targets IDO and PDL1, achieved an 80% objective response rate (ORR) and a 25.5-month median progression-free survival (PFS) [98]. Additionally, individuals with metastatic melanoma are participating in a phase III trial (NC105155254) that looks at the combination of 10102-10103 with pembroli zumab .
4) Nucleic acid based vaccines
By transfecting RNA or DNA into host cells, nucleic acid cancer vaccines that can directly gener ate the target antigen cause a strong CD8+T-cell response mediated by MHC-I molecules[99]. Usually, there are two types of cancer vaccines: DNA and mRNA.
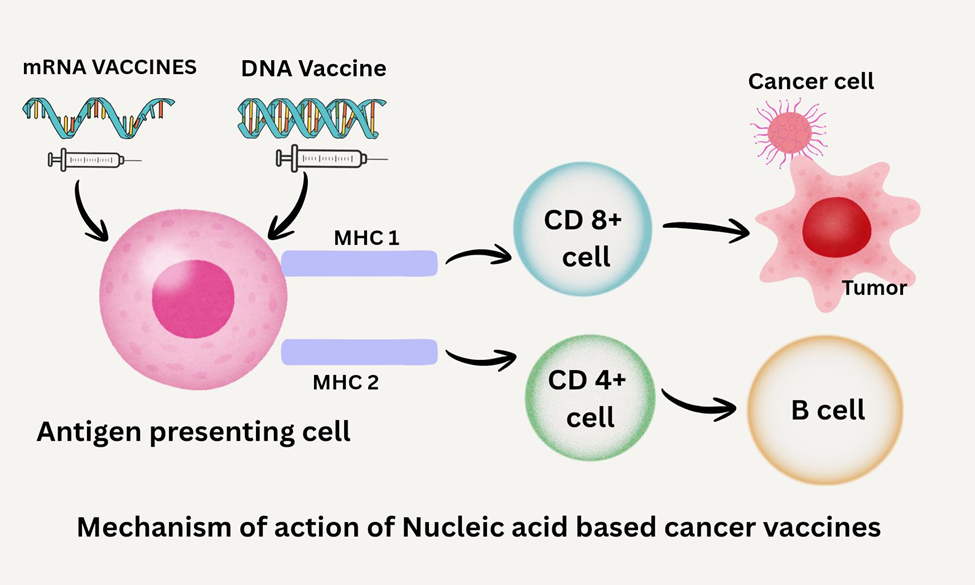
Figure 5: Mechanism of action of Nucleic acid based Cancer vaccines
DNA based
A new approach that has shown promise in generating robust protection against weak TAAs is DNA-based vaccinations Improved delivery systems (Gene Gun, cationic liposomes) [100,101], concurrent administration of cytokines (GM-CSF or 12) [102], and the use of distinct plasmids encoding nonself-antigens (such as hepatitis B surface antigen) [103] are some of the strategies that have been developed and tested to increase the potency of DNA-based vaccines. Different changes of plasmid encoded antigens can also increase the immunogenicity of DNA-based vaccinations. [104,105].
One example of a synthetic DNA cancer vaccine is INO-5401, which encodes several cancer antigens, including prostate-specific membrane antigen (PSMA), WT1, and human telomerase reverse transcriptase (HTERT). Reardon et al.'s study of INO-5401 and INO-9012 (a synthetic DNA plasmid encoding interleukin-12 [IL-12]) in glioblastoma patients revealed that this strategy may elicit a robust immune response that is associated with improved survival rates. [106]
GX-188E, a therapeutic HPV E6/E7 DNA vaccination, improved DC antigen processing a nd presentation when combined with Fms-related tyrosine kinase 3 (Fit3) and the tissue plasminogen activator signal sequence [107]. Patients with grade 3 cervical intraepithelial neoplasia (CIN3) showed strong Th1-polarized cellular immune responses following vaccination, and most of them had particular multifunctional CD8+T cells. [107].
Patients with incurable cervical cancer are presently undergoing a phase II trial to assess the combination of GX-188E with pembrolizumab; the preliminary findings have been encouraging [108].
In patients with proven CIN2/3 intramuscular injection of VGX-3100, which targets HPV E6/E7, followed by electroporation produced a significant histological regression and virus clearance rate The presence of certain CD8+ T cells, antibody production, and the magnitude of perforin expression were linked to the therapeutic outcomes [109]. Positive outcomes have been reported from the phase III clinical trial of VGX-3100 (NCT03721978).
In patients with advanced hepatocellular carcinoma, GNOS-PV02, another therapeutic DNA vaccine that encoded up to 40 personalized neoantigens and was co-administered with plasmid-encoded IL-12 plus pembrolizumab, produced a 30.6% ORR and an 8.3% complete response (CR). [110].
RNA based
Another appealing therapeutic strategy for the treatment of cancer is mRNA-based gene transfer vaccines [111, 112]. Because the transfected mRNA does not integrate into the host genome, this technique, which is mainly based on transitory transfection of nondividing cells, is considered pharmaceutically safe [113]. Additionally, electroporation can be used to obtain high transfection efficiency In vitro transcription from a bacteriophage promoter-equipped plasmid DNA produces mRNA, which can be efficiently overexpressed in target cells. It consists of a polyadenosine tail (polyA tail), the target antigen’s coding RNA, and a cap structure at the 5’ end.[114,115,116]
The target antigen may be autologous tumor mRNA [121], allogeneic cancer cell lines [130, 119, 120], or a single peptide PSA [117] or CEA [118]. After being transfected into DCs, the mRNA-based vaccine carrying the mRNA-coding TAA is translated into proteins. An antigen-specific CTL response can be triggered by loading the antigen onto MHC molecules for antigen presentation following protein processing. [122]
Patients with prostate cancer[130,117,123] RCC[124] ovarian cancer [125] lung cancer breast cancer [118], pediatric brain cancer [126], neuroblastoma [127], and melanoma [128, 129] have undergone clinical trials using mRNA-transfected DCs or directly injecting mRNA. PSA-mRNA-transfected DCs were used in a phase I clinical trial for patients with metastatic prostate cancer [117]. The results showed that the vaccine could boost PSA-specific CTL responses when the effects of repeated immunizations with PSA-mRNA-transfected DCs were investigated.
Future Prospects of Cancer Vaccines
Cancer vaccines are emerging as an important area of research in modern oncology, with a growing focus on personalized and precision-based treatment strategies. Rapid progress in tumor genomics and molecular profiling has made it possible to identify tumor-specific antigens unique to each patient. This has encouraged the development of personalized cancer vaccines that can stimulate a targeted immune response against cancer cells while sparing healthy tissues.
Neoantigen-based vaccines represent one of the most promising advancements in this field. Since neoantigens arise from tumor-specific mutations, they are highly immunogenic and reduce the risk of immune tolerance. In addition, the development of mRNA and DNA vaccine platforms has further strengthened cancer vaccine research. These platforms allow rapid production, flexibility in antigen selection, and the inclusion of multiple antigens within a single formulation, making them well suited to address tumor heterogeneity.
Another important future direction is the use of cancer vaccines in combination with other treatment modalities. When used alongside immune checkpoint inhibitors, chemotherapy, radiotherapy, or targeted therapies, cancer vaccines may enhance immune activation and improve therapeutic outcomes. Such combination approaches can help overcome immune suppression created by the tumor microenvironment. Clinical research is also shifting toward the use of cancer vaccines in early-stage disease and adjuvant settings, particularly after surgical removal of tumors. At this stage, the immune system is better equipped to respond, increasing the chances of preventing recurrence. Additionally, targeting cancer stem cells and circulating tumor cells through vaccination strategies may reduce metastasis and long-term relapse. The identification of reliable biomarkers and improved immune monitoring techniques will further guide patient selection, treatment optimization, and assessment of vaccine efficacy. Together, these advancements suggest that cancer vaccines may play a more significant role in future cancer management.
CONCLUSION
Although the development of cancer vaccines has faced several setbacks in the past, recent scientific advances have renewed confidence in this therapeutic approach. Earlier challenges, such as tumor heterogeneity, inadequate antigen selection, and use in late-stage disease, limited their clinical success. However, improved understanding of tumor biology and immune mechanisms has highlighted the importance of personalized, multi-antigen, and combination-based vaccine strategies. The future of cancer vaccines lies in individualized treatment, early clinical application, and integration with other cancer therapies. Despite challenges related to manufacturing, cost, and regulatory approval, cancer vaccines hold strong potential as a safe and targeted treatment option with continued research and technological progress, they are likely to become an important component of precision oncology.
REFERENCES




Ashwini Taware, Chetana Mayekar, Manisha Nangude, Harsh Tapal, Pranali Vekhande, Manas Suryarao, Cancer Vaccines, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3632-3651. https://doi.org/10.5281/zenodo.19248034
 10.5281/zenodo.19248034
10.5281/zenodo.19248034
