Shivlingeshwar College Of Pharmacy (Pharm D), Almala, Latur.
Accurate staging is crucial for determining the best treatment for non-small-cell lung cancer (NSCLC). Early-stage NSCLC is usually treated with surgery. For locally advanced NSCLC, a combination of chemotherapy, radiation, and sometimes surgery is used. In metastatic NSCLC, chemotherapy has been proven to improve survival and quality of life. This discussion will cover the various surgical, chemotherapy, and radiation treatment options, as well as the benefits of combining these therapies for different stages of NSCLC.
Proof using our professional knowledge and the particular values and circumstances of each patient A method of providing healthcare that stresses the integration of the best available scientific evidence with clinical knowledge and patient values is known as evidence-based medicine, or EBM. Critically evaluated and current data from carefully planned research studies informs medical decisions and practices in evidence-based medicine. Enhancing the standard of patient care is the goal of this approach. by making certain that scientific proof of the efficacy of medical interventions, therapies, and diagnostic techniques is used. Evidence-based medical practitioners evaluate scientific literature in a methodical manner, taking into account the validity, reliability, and applicability of research in order to make well-informed decisions regarding patient care. This method seeks to strike a compromise between patient preferences and clinical experience, acknowledging their significance and aiming for the best.
In summary, evidence-based medicine gives medical personnel a methodical and exacting framework to use when making judgments, which eventually improves the general efficacy and caliber of medical practice.
1.2. History:
The term "scientific medicine" was first used in 1990 by Dr. Gordon Guyatt, a young coordinator at McMaster University's Internal Medicine Residency. This method built on the work of his mentor, Dr. David Sackett, by employing critical appraisal techniques to teach medicine at the bedside. Nonetheless, his coworkers disapproved of the notion that contemporary clinical judgments might not be wholly scientific. Guyatt devised a new name for the residency program's core curriculum in order to address this:
"Medicine Based on Evidence" (EBM). An editorial from the ACP Journal Club in 1991 described this trend. Evidence-Based Medicine (EBM), which was developed in 1991, was a groundbreaking approach that drew from years of cross-disciplinary collaboration. Clinical epidemiology, biomedical informatics, and evidence-based guidelines are only a few of the many topics covered by EBM. One important topic will be briefly discussed in this essay: the development of clinical epidemiology and related.
1.3. Integration into clinical practice.
The foundations of EBM can be found in the identification of the shortcomings of conventional healthcare practices in the US and their effects on the cost and quality of patient attention. A paradigm change was brought about by the requirement for more clarity in decision-making. Clinical practice was traditionally viewed as the "art of medicine," depending on the knowledge and judgment of experts. Rarely were scientific methods and statistical analysis used, which are typical in epidemiology and biomedical research. Medical resistance to implementing these technologies was rooted in political mistrust and historical precedent. Global events in the 1960s, however, cleared the path for EBM. The Growing awareness of the limitations in standard clinical approaches prompted a reconsideration of incorporating scientific methodologies. EBM essentially developed as a result of efforts to bring scientific rigor to clinical decision-making, rather than as a stand-alone concept in 1991. Overcoming historical barriers, changing viewpoints, and embracing the insights gained from diverse disciplines worldwide were all part of the voyage. This change signaled a turning point in medical practice by putting an emphasis on facts and evidence in addition to clinical knowledge. Having received training at Harvard Medical School, Stanford Medical Center, and Johns Hopkins University, Suzanne and Robert Fletcher saw a problem in medicine at the beginning of the 1960s. Clinical practice and biological science have not always been compatible. Uncontrolled cellular growth brought on by genetic and epigenetic changes is a hallmark of the diverse group of disorders known as cancer. By interfering with regulatory processes, these alterations allow cells to avoid growth inhibition, withstand apoptosis, and spread. DNA repair deficiencies (e.g., *BRCA1/2*), tumor suppressor gene inactivation (e.g., *TP53*), and oncogene activation (e.g., *RAS*) are important drivers. Risk factors include lifestyle choices (e.g., nutrition, lack of physical exercise), heredity, and environmental exposures (e.g., smoke, UV radiation). Both benign (localized) and malignant (invasive, metastatic) tumor are possible.[1,2]. Keeping up with the latest advancements in medical publications can be challenging for clinicians. For instance, a general practitioner should read 19 articles daily, but we know that many of them only have an hour to devote to this task. When a doctor spends the majority of their working hours reviewing all published articles and studies, they are experiencing academic isolation, often known as the armchair phenomenon. However, even if the physicians had the time to read them all, they would not have enough time to assess the study's worth, methodology, results, and transparency. Given his restricted time, the doctor must so read carefully and choose wisely what he reads and what he does not read.[3] Due to its inherent complexity, family medicine is characterized by a large percentage of poorly differentiated issues that intersect with biological, psychological, and social variables. Evidence-Based Medicine (EBM), which dates back to the second half of the 1800s, refers to the deliberate and prudent application of the best available scientific data when deciding how best to treat each patient. The diligent, clear, prudent, and rational application of the best available evidence when making choices on a patient's treatment is known as evidence-based medicine. Randomized controlled clinical studies with a large sample size that demonstrate the efficacy of several medications as well as the drawbacks and ineffectiveness of others as compared to the best available treatment are thought to provide the finest scientific evidence.[4] In evidence-based medicine, patient care necessitates the acquisition of clinically significant knowledge over a lifetime of self-directed, problem-based learning. PAPER on treatments, diagnosis, prognosis, and other clinical and medical matters. According to EBM, you should focus your reading on topics pertaining to particular patient problems rather than constantly searching through the contents of hundreds of publications for intriguing research. It might be more effective to create clinical questions first, then search up-to-date databases to stay up to date with the research. In evidence-based medicine, "the abstract activity of reading and evaluating the literature is transformed into the practical process of applying the literature to benefit individual patients while simultaneously broadening the clinician's knowledge base." A "cookbook" approach to medicine is not evidence-based medicine. It cannot lead to slavish, cookbook approaches to individual patient treatment since it necessitates a bottom-up strategy that incorporates the best available external evidence with clinical skill and patient preferences. Individual clinical expertise determines whether or not external clinical evidence applies to a certain patient and, if it does, how it should be incorporated into a therapeutic decision. External clinical evidence can support this knowledge, but it can never completely replace it. Comparably, when determining if and how an external guideline fits the patient's clinical state, situation, and preferences—and, thus, whether it should be applied—it must be combined with individual professional competence. Advocates of evidence-based medicine will join clinicians who are afraid of top-down directives at the barricades.[5] Evidence-Based Medicine (EBM) plays a vital role in lung cancer treatment because it can maximize results by combining the best available clinical research, professional knowledge, and patient values.
1.3.1. Diagnosis and Molecular Profiling
Non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC) require distinct treatments. Molecular profiling (e.g., EGFR, ALK, ROS1, KRAS, *PD-L1*) guides targeted therapy selection.
- EGFR mutations occur in ~15% of NSCLC patients in Western populations and up to 50% in Asian populations. Testing for these mutations is standard for first-line EGFR tyrosine kinase inhibitors (TKIs).[6]
1.3.2. Treatment Selection
EBM drives therapy choices based on clinical trial data and biomarker evidence.
A. Targeted Therapies
B. Immunotherapy:
- Pembrolizumab became a first-line standard for PD-L1-high (≥50%) NSCLC after the KEYNOTE-024 trial showed superior overall survival (OS) vs. chemotherapy. [8]
C. Adjuvant and Neoadjuvant Therapy:
D. Adaptive and Personalized Therapy
Osimertinib is standard for *EGFR T790M*-mediated resistance, as shown in the AURA3 trial.
1.4. Guideline Development and Standardization
EBM synthesizes evidence into clinical guidelines to ensure consistency in care.
ESMO Guidelines:
1.5. Emerging Therapies and Trials:
EBM accelerates the adoption of novel therapies validated by clinical trials.
1.6. Antibody-Drug Conjugates (ADCs):
1.7. Challenges and Future Directions:
- Access to Biomarker Testing:
- Disparities in molecular testing persist globally, limiting personalized therapy.
Tumor Heterogeneity:
- Clonal evolution and resistance mechanisms necessitate ongoing research.[11]
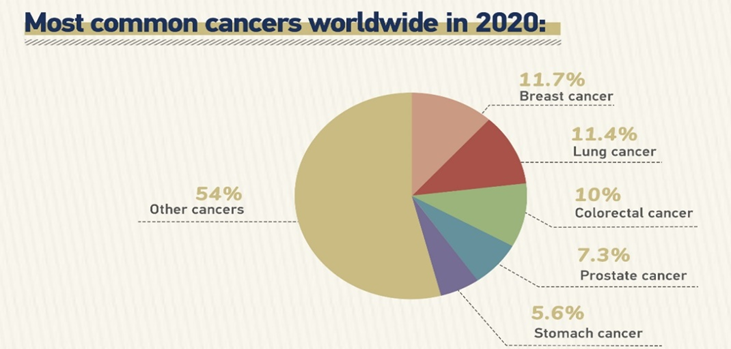
Fig:01
Table:01
|
|
Male |
Female |
Both Sex |
|
Population
|
3972735747 |
3912335034 |
788507081 |
|
Incidence |
|
||
|
Number Of New Cancer Case |
10311610 |
96649889 |
19978499 |
|
Age Standardized Incidence Rate |
212. |
186 |
196 |
|
Resk Of Development of Cancer Before The Age Of 75 Years |
21 |
18 |
20 |
|
Top 3 Leading Cancer |
Lungs Prosted Colorectum |
Brest Luns Colorectum |
Lungs Brest Colorectum |
|
Mortality |
|
||
|
Number Of Cancer Death |
5430284 |
4313538 |
9743832 |
|
Age Standard Mortility Rate |
109 |
76 |
91 |
|
Resk Of Deaying Of Cancer Befor The Age Of 75 Year |
11 |
08 |
09 |
|
Top 3 Leading Cancer |
Lungs Liver Colorectum |
Best Lungs Colorectum |
Lungs Colorectum Liver |
|
Prevelance |
|
||
|
5 Year Prevelent Case |
25747272 |
27756915 |
53503187 |
2. Lung cancer in India
2.1. Current status and promising strategies
Among the world's biggest causes of mortality is lung cancer. It is a significant issue in Indian healthcare as well. On February 20, 2016, the following results were found when searching for "lung cancer India" online. There were 43,80,000 results from Google, 1,77,000 Scholarly articles, and 2592 papers on the nlm.nih.gov website in the PubMed Medline database. Figure 1 lists the Indian lung cancer papers that were cited in PubMed. The fact that the medical profession as a whole and oncologists in particular are consistently adding to the body of information regarding lung cancer is encouraging.[12]
The number of publications doubled from 42 in 2004 to 2006 and then reached a peak of 407 in 2014, over 10 times the number in just ten years. The impact this data is having globally is even more significant. Some of the pieces from India have citation indexes that are comparable to those of renowned periodicals, which is quite astounding. This can be attributed to some original research that included the largest series of lung cancer patients from India, demonstrated pharmacogenomic differences in any cancer for the first time in history, and showed that choosing one of the standards of care options can be customized to maximize the outcome based on previously unidentified criteria.
Nevertheless, other papers compare the characteristics and results of patients of Asian descent, including those from India, and show that patients with advanced lung cancer who receive treatment from medical oncologists rather than other oncologists or healthcare providers had a higher chance of survival.[13] The public and private sectors of India's healthcare system coexist. For those with low incomes, the public health system offers free or heavily discounted medical treatment. Nonetheless, India's overall health care spending (including public and out-of-pocket) as a proportion of GDP is low (3.6% of GDP) in comparison to the Organization for Economic Co-operation and Development's average of 8.8% of GDP in 2018. Health insurance coverage is also inadequate. Fewer than 28.7% of families had any regular member insured by any health insurance plan, according to the National Family Health Survey 2015–2016 (National Family Health Survey-4; http://rchiips.org/nfhs/index.shtml) (28.2% in urban areas and 28.9% in rural one). In order to give 500 million people free access to healthcare, the government recently launched the Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (https://pmjay.gov.in), which provides insurance coverage of 5 lakh rupees per family annually for secondary and tertiary healthcare. India ranks third globally in terms of tobacco production and consumption. In India, tobacco consumption is estimated to be 28.6%. 267 million tobacco users are expected to be in the nation (Global Adult Tobacco Survey-2 [GATS]-2 2016–2017: India information sheet; http://gatsatlas.org), with 42.4% of males and 14.2% of women smokers. In GATS-2 (2016–2017), the prevalence of tobacco usage has significantly decreased in comparison to GATS-1 (2009–2010). In 2007 and 2008, the Indian government launched. National Tobacco Control Program (http://ntcp.nhp.gov.in) to increase public awareness of the harmful effects of tobacco, regulate tobacco production and consumption, enact and enforce the Cigarette and Other Tobacco Product Act, support and strengthen tobacco cessation services, and encourage the successful application of the WHO Framework Convention on Tobacco Control's strategies. 612 districts across are currently using this program.[14]
3. Epidemiology
The worldwide burden In 2020, there were approximately 10.3 million new cases and 10 million deaths globally (WHO, 2020).
3.1. Common Cancers: Prostate, colorectal, stomach, lung, and breast cancers are the most common. Geographic variance is present; for example, HPV causes cervical cancer to be more common in low-resource areas.
3.2. Disparities: While low-income areas have late diagnosis and infection-related cancers (e.g., HBV, *H. pylori*), high-income nations report higher incidence but lower mortality (early detection/treatment availability).
3.3. Trends: Urbanization, aging populations, and changes in lifestyle (such as smoking and obesity) are all associated with an increasing incidence.[15]
Squamous and small cell lung cancers, which are closely linked to tobacco use, used to dominate the epidemiology of lung cancer in India. However, adenocarcinoma eventually overtook them as the most common histologic type. This change in histologic profile has mostly taken place in the last ten years, and it has trailed behind the change seen in industrialized nations in this regard. The reason for this "time lag" has been attributed to the fact that, in India, "bidi," or handmade tobacco smoking products, which are mainly based on cottage industries, have been and still are the most popular kind of smoking product. This is in contrast to the more regulated and mechanized cigarette manufacturing process, which has seen little change over time (similar to the latter, which has been marketed for a long time with low nicotine content and filtered cigarettes). Furthermore, the reported prevalence of NSCLC-not otherwise specified (undifferentiated NSCLC) subtype has decreased as a result of improvements in histologic typing by reporting pathologists linked to increased use of immunochemistry (IHC). The majority of cases are classified as non-squamous NSCLC adenocarcinoma. enumerates the significant epidemiologic research conducted on lung cancer in India during the previous thirty years. The majority of lung cancer patients in India had both locally progressed and metastatic illness upon presentation.[16]
Table:02 Demographic and Key Stastics of India
|
Demographic Variable |
Numerical Value |
|
Total population |
1.38 billion |
|
Urban population |
34.5% |
|
Life expectancy |
70.42 y |
|
Languages |
216 |
|
Sex ratio |
924 females per 1000 males |
|
Nominal GDP |
$3.202 trillion |
|
PPP |
$11.33 trillion |
|
Total health care expenditure |
3.6% of GDP |
|
Health insurance coverage |
20% of women and 23% of men |
|
Doctor-population ratio |
1:1456 (WHO recommendation 1:1000) |
|
Noncommunicable diseases |
60% of all deaths |
|
Tobacco use |
28.6% of adults |
Table:03
|
Globocan India statistics 2018 |
|
|
Number of new cancer cases |
1.16 million |
|
Cancer deaths |
784,821 |
|
Number of prevalent cancer cases (5-y) |
2.26 million |
|
Lung cancer |
5.9% of all cancer cases (fourth most common) |
|
Lung cancer incidence |
67,795 |
|
Lung cancer mortality |
63,475 (8.1% of all cancer deaths) |
Table:04
|
Projected incidence, 2020S2 |
|
|
All sites |
1,392,179 |
|
Males |
679,421 |
|
Females |
712,758 |
|
Lung cancer |
712,758 |
|
Males |
71,788 |
|
Females |
26,490 |
4. CLASSIFICATION OF CANCERS
4.1. Carcinomas (Cancers of Epithelial Cells)
4.2. Sarcomas (Cancers of Connective Tissues)
4.3. Leukemia (Blood Cancers)
4.4. Lymphomas (Cancer of Lymphatic System)
4.5. Brain and Spinal Cord Tumor
4.6. Other Notable Cancers
Germ Cell Tumor– Cancer in reproductive cells (e.g., testicular and ovarian cancer).[18]
Fig:02
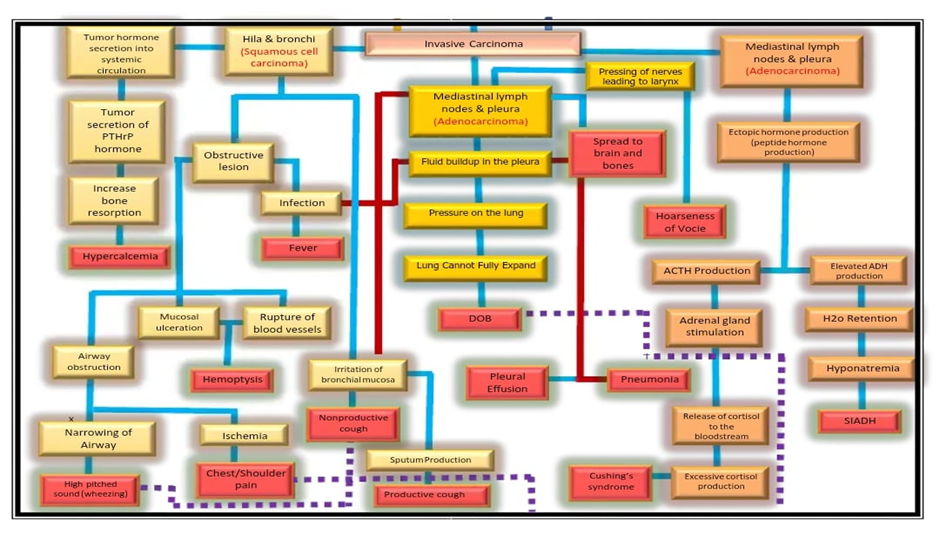
5.Pathology:
6.Investigation Of Disease
The most popular methods for identifying lung cancer are transthoracic sampling and flexible bronchoscopy. While lesions in the peripheral third of the thorax are often addressed trans thoracically, those in the central third are typically accessed bronchoscopically. Over the last ten years, bronchoscopy services have expanded significantly in India, however they appear to be concentrated in large cities.12- Numerous pulmonologists provide advanced bronchoscopic methods, including endobronchial ultrasonography (EBUS).[19] Interventional radiologists typically use imaging guidance (CT or ultrasound) when doing transthoracic sampling. Less than 1% of Indian hospitals now have a special setup for interventional radiology, though.13 Depending on patient-specific characteristics and the level of competence available, either modality can access lesions in the middle part of the chest. These bronchoscopy methods include electromagnetic navigation bronchoscopy, virtual bronchoscopic avigation, radial EBUS, and ultrathin bronchoscopy for sampling peripheral lesions. Nevertheless, these bronchoscopic methods are not commonly accessible. PET-guided biopsy has become a viable method for transthoracic sampling in more recent times.14. It is noteworthy that the metabolic characterisation offered by PET-CT can make it possible to target live tissue when sampling, increasing the diagnostic yield.[20] According to preliminary findings, a diagnosis might be made for all patients following a PET-CT-guided biopsy if the results of prior invasive sample were unclear for thoracic lesions.14. In cases with advanced illness, it is crucial to ensure sufficient samples for histologic and molecular characterization. However, this might be difficult at smaller centers due to a lack of experience. Detecting driver mutations using liquid biopsy might be useful in these circumstances when sufficient tissue is not available for further analysis. In order to determine the local and distant extent of the illness, patients with lung cancer typically undergo non-invasive imaging staging. Particularly for individuals with serious illness, non-invasive staging is crucial. The most reliable non invasive staging technique for lung cancer is a whole-body PET-CT scan. A radionuclide bone scan is used in conjunction with a contrast-enhanced CT scan of the chest and upper abdomen (containing the liver and adrenal glands) for staging in centers where PET-CT is not easily accessible.[21] Magnetic resonance imaging of the brain is typically included of the staging evaluation since PET-CT is not sensitive enough for brain metastases. When evaluating patients who are not surgical candidates, the majority of Indian centers limit the staging examination to a contrast-enhanced CT scan of the chest and upper abdomen. If the clinical evaluation does not indicate metastatic illness, PET-CT or magnetic resonance imaging of the brain are not typically performed. Mediastinal staging is usually invasive for the majority of patients with resectable illness.
Because of the potential for false-positive results, invasive mediastinal staging is typically used to confirm any imaging indications of nodal involvement. It is particularly important to provide histological proof of nodal involvement in nations like India where granulomatous illnesses, like TB, are widespread. A limited percentage of patients with peripheral stage IA illness who show no signs of hilar or mediastinal involvement on PET-CT often do not require invasive mediastinal staging. [22] In India, the practice varies. Because the negative predictive value of a PET-CT is not 100%, some centers choose to undertake invasive mediastinal staging in all patients with resectable disease even if the PET-CT is negative. However, other centers would rather adopt a policy that limits the use of invasive mediastinal staging to individuals in whom PETCT shows suspicion of N3 illness, thereby promoting liberal neoadjuvant chemotherapy (NACT) in subjects with any N2 disease on PET-CT. The methods for invasive mediastinal staging include mediastinoscopy and endosonographic procedures (EBUS with or without endoscopic ultrasonography). The widely acknowledged method for invasive mediastinal staging is mediastinoscopy. When opposed to endosonographic procedures, mediastinoscopy delivers a greater volume of tissue for further analysis and presents the possibility of a full lymphadenectomy, particularly when video aided. It is constrained, nonetheless, by the scarcity of skilled thoracic surgeons and the possibility of higher morbidity as compared to endosonographic treatments. However, the morbidity and mortality linked to mediastinoscopy are often insignificant in seasoned centers. Research suggests that endoscopic operations are less likely to result in complications and have a comparable yield to mediastinoscopy. Nonetheless, some centers adopt a negative endoscopic mediastinal staging in conjunction with mediastinoscopy due to ongoing concerns about the increased false negative rate of endosonographic procedures as compared to mediastinoscopy. In other centers, a negative endoscopic mediastinal staging is followed immediately by surgery.[23]
7.Screening Techniques:
• Flexible bronchoscopy and transthoracic sampling are the two methods most frequently employed to diagnose lung cancer.
• Transthoracic sampling is utilized for peripheral lesions, whereas bronchoscopy is recommended for core thoracic lesions.
• Depending on patient-specific characteristics and available competence, either approach can be used to reach middle thoracic lesions. [24]
? 7.1. Bronchoscopic Techniques:
? 7.2. Transthoracic Sampling:
? 7.3. Non-Invasive Staging:
? 7.4. Invasive Mediastinal Staging:
? 7.5. Variability in Practice:
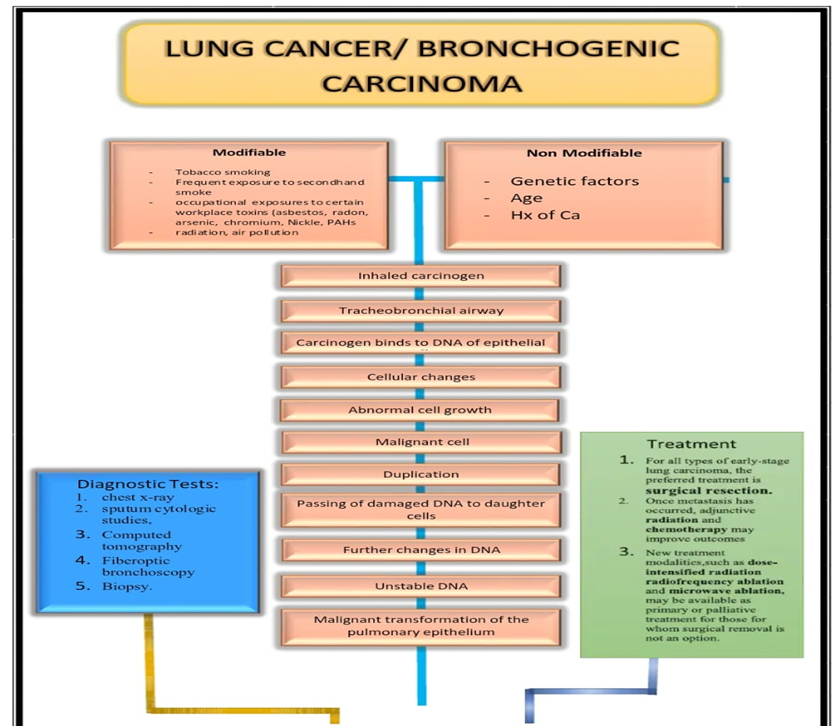
8.Triggering Factor
A. Tobacco Smoking
- Description: The leading cause of lung cancer, responsible for ~85% of cases.
- Mechanism: Carcinogens in tobacco smoke damage DNA in lung cells.
B. Second hand Smoke
- Description: Non-smokers exposed to tobacco smoke have a 20-30% increased risk. [29]
C. Occupational Exposures
- Asbestos: Increases risk of lung cancer and mesothelioma.
- Radon: A radioactive gas found in soil and buildings.
D. Air Pollution
- Description: Particulate matter (PM2.5) from vehicle exhaust and industrial emissions
E. Diet and Lifestyle
- Low Fruit/Vegetable Intake: Associated with increased risk.
- Alcohol Consumption: Heavy drinking may elevate risk. [30]
8.1. Non-Modifiable Risk Factors
A. Genetic Predisposition
- Family History: First-degree relatives with lung cancer increase risk.
- Inherited Mutations: Mutations in genes like *EGFR*, *KRAS*, or *TP53*.
B. Age
- Description: Risk increases significantly after age 50.
C. Gender
- Description: Historically higher in men, but rates in women are rising due to smoking trends.
D. Chronic Lung Disease
- COPD: Chronic inflammation increases cancer risk.
- Pulmonary Fibrosis: Scarring of lung tissue.
B. Infections - HIV: Increased risk due to immunosuppression. - Tuberculosis: Chronic inflammation and scarring.
9. Intervention:
9.1. Alternative Therapy
9.1.1. Surgery
By removing the tumor or a section of the lung, surgery can improve prognosis and possibly even cure localized lung cancer.
If the tumor is limited to one lung and the patient has sufficient lung function, a lobectomy (removal of a lung lobe) or pneumonectomy (removal of an entire lung) may be carried out. Patients with early-stage malignancies or those who are unable to undergo more involved surgery may benefit from segmentectomy, which involves removing a portion of a lobe. Some situations where the cancer is in a peripheral site may use wedge resection, which involves removing a small part of the lung tissue.[31,32]
9.1.2. Radiation Therapy
Patients who are unable to have surgery can benefit from radiation therapy, which can also be used to relieve symptoms or as part of a curative treatment plan that includes chemotherapy or surgery.
High-energy X-rays are delivered to the tumor by external beam radiation treatment (EBRT).
For patients who are not candidates for surgery or for early-stage, incurable cancers, stereotactic body radiation treatment (SBRT), a more accurate kind of radiation, is frequently utilized.
By employing protons rather of X-rays, proton therapy is a type of radiation that may help preserve healthy tissue surrounding malignancies. [33]
9.1.3. Palliative Care
Symptom relief and quality of life enhancement are the main goals of palliative care for patients with advanced lung cancer or those who are not responding to curative treatment.
Pain management that reduces discomfort by non-pharmacological methods including physical therapy, acupuncture, or relaxation techniques. Breathing techniques and pulmonary rehabilitation to enhance respiratory function, particularly for people with diminished lung function or shortness of breath
Nutritional assistance through dietary guidance and weight-loss management techniques, which are frequent in patients with lung cancer.[34]
9.1.4. Physical Therapy and Pulmonary Rehabilitation
Maintaining physical function, strength, and mobility—particularly after surgery or in advanced stages of disease—requires physical therapy. Programs for pulmonary rehabilitation are especially designed to improve quality of life, lessen dyspnea, and improve lung function.
Exercise training enhances physical endurance and lessens weariness. Patients can increase oxygenation and control dyspnea by using breathing techniques including pursed-lip breathing and diaphragmatic breathing instruction on symptom management, including ways to save energy and increase physical capability. [35]
9.1.5. Nutritional Therapy
Malnutrition is a common problem in lung cancer patients due to loss of appetite, difficulty swallowing, or the effects of the cancer itself. Nutritional therapy aims to maintain optimal weight, prevent cachexia (wasting), and improve patient strength and overall health
Dietitians work to provide high-calorie, high-protein foods and manage side effects of treatment such as nausea or taste changes.
In some cases, enteral nutrition (tube feeding) or parenteral nutrition (IV feeding) may be required.
9.1.6. Psychosocial Support
The diagnosis and treatment of lung cancer can have a serious negative effect on mental health, increasing stress, anxiety, and depression. Patients can better handle their diagnosis and treatment with psychological support from mental health providers, support groups, and counseling.
It has been demonstrated that cognitive-behavioral therapy (CBT) helps cancer patients with their anxiety and depression symptoms. [36,37]
Relaxation methods and mindfulness meditation may aid in stress management and enhance mental health.
9.1.7. Complementary and Alternative Therapies
To control pain, lessen symptoms, or deal with stress, some patients could look for complementary therapies. These consist of: Acupuncture for weariness, nausea, and discomfort. massage treatment to promote relaxation and ease tense muscles.
Yoga and meditation can help you feel less stressed, more flexible, and less anxious.
Aromatherapy for relaxation and mood enhancement. It is important to remember that although complementary therapies could help with symptoms, they should only be used sparingly and in addition to conventional treatments, not in substitute of them. [38,39]
10. Drug Therapy
Table 05. Chemotherapy for Lung Cancer
|
Drug |
Type of Agent |
Major Adverse Effects |
Comments |
|
Platinum agents |
|
|
|
|
Cisplatin (Platinol) |
Atypical alkylator |
Nausea and vomiting (common),† nephrotoxicity, ototoxicity, neuropathy, myelosuppression (mild), electrolyte wasting (potassium and magnesium) |
Hydration required before and after administration |
|
Carboplatin (Paraplatin) |
Atypical alkylator |
Myelosuppression, † nausea and vomiting (mild), neurotoxicity (rare), nephrotoxicity (rare |
Dose usually determined by area under the curve, taking renal function into account with use of the Calvert formula |
|
Nonplatinum agents |
|
|
|
|
Etoposide (VePesid) |
Topoisomerase II inhibitor |
Myelosuppression, † nausea and vomiting, stomatitis, diarrhea |
Stomatitis and diarrhea rare with normal dose |
|
Topotecan (Hycamptin |
Topoisomerase I inhibitor |
Myelosuppression, † nausea and vomiting, diarrhea, headache |
Increased monitoring of liver function necessary |
|
Irinotecan (Camptosar) |
Topoisomerase I inhibitor |
Myelosuppression, † diarrhea, nausea and vomiting |
------------ |
|
Gemcitabine (Gemzar) |
Antimetabolite |
Myelosuppression, † nausea and vomiting, diarrhea, edema, influenza-like syndrome |
Increased monitoring of liver function necessary |
|
Paclitaxel (Taxol) |
Microtubule inhibitor |
Myelosuppression, † mucositis, peripheral neuropathy, hypersensitivity reaction, nausea and vomiting |
Requires pretreatment with dexamethasone, diphenhydramine hydrochloride, ranitidine |
|
Docetaxel (Taxotere) |
Microtubule inhibitor |
Myelosuppression ,† edema and fluid retention, mucositis, diarrhea, nausea and vomiting |
Requires treatment with dexamethasone before, during, and after infusion |
|
Vinorelbine (Navelbine) |
Microtubule inhibitor |
Myelosuppression, † nausea and vomiting |
Mild vesicant |
|
Vincristine (Oncovin) |
Microtubule inhibitor |
Neuropathy, † constipation |
Vesicant |
|
Doxorubicin (Adriamycin) |
Anthracycline antibiotic |
Myelosuppression, † cardiomyopathy, nausea and vomiting, diarrhea, stomatitis |
Cardiotoxic effects occur with cumulative doses of more than 375 mg/m 2 of body surface area; potent vesicant; precautions against extravasation necessary |
|
Cyclophosphamide (Cytoxan) |
Alkylating agent |
Myelosuppression, † nausea and vomiting, hemorrhagic cystitis |
Hemorrhagic cystitis rare with standard doses |
|
Ifosfamide (Ifex) |
Alkylating agent |
Myelosuppression, † nausea and vomiting, hemorrhagic cystitis, nephrotoxicity, neurotoxicity |
Mesna given to prevent Hemorrhagic cystitis |
11. Adverse Reaction
11. 1. Surgery
Common Side Effects:
-The place of the incision is painful.
-Breathlessness (caused by decreased lung capacity).
-Lung infection or pneumonia.
-Extended bleeding or air leaks [40]
Long-term Risks:
-Prolonged discomfort or numbness.
- Decreased tolerance to exercise
11. 2. Radiation Therapy
Acute Side Effects:
-Weariness.
- Skin discomfort (such as peeling or redness).
-Esophagitis, or difficult swallowing [41]
Long-term Risks:
- Pneumonia from radiation (inflammation of the lung).
-The scarring of lung tissue is known as pulmonary fibrosis.
-Damage to the heart (should radiation strike the chest).
11.3. Chemotherapy
Common Side Effects:
- feeling queasy or throwing up.
Weariness and hair loss.
Myelosuppression, or decreased neutrophil numbers [42]
Serious Risks:
- Neuropathy (nerve damage).
- Kidney or liver damage.
- Increased infection risk (due to immunosuppression).[43,44]
11.4. Targeted Therapy (e.g., EGFR, ALK inhibitors)
Common Side Effects:
- Skin rash (e.g., acneiform eruptions with EGFR inhibitors).
- Diarrhea.
- Fatigue.
Serious Risks:
- Interstitial lung disease (ILD).
- Cardiac toxicity (e.g., QT prolongation with some ALK inhibitors) [45,46]
11.5. Immunotherapy (e.g., PD-1/PD-L1 inhibitors)
Common Side Effects:
- Fatigue.
- Skin rash.
- Diarrhea/colitis.
Immune-Related Adverse Events (irAEs):
- Pneumonitis.
- Hepatitis.
- Thyroid dysfunction.
- Myocarditis (rare but severe). [47,48]
11.6. Combination Therapies
Synergistic Toxicity:
-Enhanced myelosuppression (chemotherapy + immunotherapy).
- Overlapping pneumonitis risk (radiation + immunotherapy).[49]
12. CONCLUSION:
In conclusion, the management and therapy of lung cancer greatly benefit from evidence-based medicine. Patient outcomes have been greatly enhanced by recent developments in immunotherapies, targeted medicines, surgery, and screening procedures. Personalized medicine and customized strategies are becoming more and more crucial in the treatment of lung cancer as research advances. Healthcare providers can give patients with lung cancer the best care possible by remaining current with the most recent scientific discoveries and recommendations.
REFRENCES






Upase Narsing*, Wadekar Vishal, Yadav Anil, Syed Afnaan, Shinde Akanksha, Dr. Giri Ashok, Systematic Review on Lung Cancer Therapies: An Evidence Based Approach, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 1148-1165. https://doi.org/10.5281/zenodo.15017477
 10.5281/zenodo.15017477
10.5281/zenodo.15017477
