Department of pharmacy practice, devaki amma memorial college of pharmacy, malappuram, kerala, India
Drug prescribing patterns during pregnancy are crucial in minimizing risks associated with unethical and inappropriate medication use, thereby safeguarding both maternal and fetal health. This study aimed to evaluate the prescribing trends among pregnant women and identify common complications to optimize treatment outcomes. Conducted in a tertiary care hospital in Calicut, the study involved 169 pregnant women, primarily aged 25-29 years. Most participants were from urban areas and significant proportion were primigravida. Drugs were categorized using the USFDA pregnancy risk classification system, with the majority falling under category B, followed by categories C, A and D. Iron and folic acid supplements, often prescribed from preconception period to third trimester, were the most commonly used medications. Tetanus toxoid, multivitamins, and mineral supplements were also widely administered. The predominant route of administration was oral, with tablets being the most common form. Urinary tract infections were the most frequent condition, with nitrofurantoin being the prescribed antibiotics. Other commonly prescribed drug classes included analgesics, gastrointestinal drugs, antiemetics, and antidiabetics like insulin and Glycomet. Importantly, no drugs from the high-risk category X were prescribed. The findings underscore the necessity of rational drug use in pregnancy, highlighting the prevalence of safe medication practices and the importance of continual monitoring to prevent adverse outcomes such as miscarriage, stillbirth, and birth defects.
Drug prescribing pattern reduces inherent risk resulting from unethical prescription while also offering insights into drug profile and intervention strategies. Pregnancy and medication use have been linked to birth defects since 1960s when thalidomide use during the early stages of pregnancy was discovered. The benefits and possible risks of drug use must be balanced in order for drug use during pregnancy to be rational. The thalidomide crises thus far serve as evidence that inadequate knowledge regarding the safety of many medications when taken by pregnant women is the primary cause of foetal side effects. The study was conducted to assess the drug prescribing pattern in pregnant women in a tertiary care hospital at Calicut.
Objectives
Number and timing of visits
Every pregnant woman makes at least four visits for ANC, including the first visit. The suggested schedules are:
1st visit: within 12 weeks
2 nd visit: between 14 and 26 weeks
3rd visit: between 28 and 34 weeks
4th visit: between 36 weeks and term
The United States food and drug administration (USFDA) established a system to rank the risk of using certain medications while pregnant and categorized in to A, B, C, D and X categories. The level of safety measures recommended by available human evidence and animal research. Pregnant women can safely be prescribed medications in category A and B. However, numerous studies have demonstrated that, under some situations, women may use categories D and X. The purpose of the study was to evaluate the drugs that have been used to lessen common pregnancy complications and to identify the common problems in order to improve drug prescribing during pregnancy.
MATERIALS AND METHODS
The study followed Retrospective cross-sectional study conducted for a period of six-month in PVS Sunrise Hospital, a multispecialty tertiary care hospital in Calicut, Kerala.The study was conducted after getting the approval from the Institutional ethics committee of the hospital. A standard operating procedure was maintained by the department. The various steps were: collection of sociodemographic data from case sheets of the patient viz., patient identification, age, parity, illness, drugs prescribed. Data has been collected from the case sheets of all eligible subjects in the study. Pregnant women’s medications are classified using the FDA classification system, where most drug categories are found.
RESULTS
Total of 169 candidates were enrolled in the study, Majority of pregnant women in the study were between the ages of 25-29 years, 31.9% were from age group 30-34 years, 23.6% were from age group20-24years and remaining 10% were from>35 years age (Fig1). The study further revealed that 30.7 %pregnant women had 1 child (primipara) at the time of ANC visit, 26.6% had 2 children (multipara) and 42.6 %of women had no child (primigravida)at the time of their ANC visit (Fig 2).111(65.6%) were from urban and 58(34.3%) were from rural population (Fig 3). It was observed that during pregnancy 19.5% developed hypothyroidism, 30.1% had diabetes mellitus, 2.3% had asthma, 53.2 % had hypertension, 2.9%anemia, 20.7% urinary tract infection (Fig 4). From drugs prescribed, 985 drugs were prescribed in tablet form ,57 in capsule form and 46 in syrup form (Fig 5). Mainly the drugs were administered in oral route and least as vaginal (Fig 6). According to classification of drugs based on their risk to foetus indicated that from a total of drugs prescribed 185 were belon to USFDA pregnancy risk category A, 403were from category B, 288 from category C, and 13 from category D. There are no drugs prescribed from category X (Fig 7).
Table 1: Sociodemographic data’s
|
AGE |
SAMPLE(n) |
PERCENTAGE (%) |
|
20-24 |
40 |
23.6% |
|
25-29 |
57 |
33.7% |
|
30-34 |
54 |
31.9% |
|
>35 |
18 |
10.6% |
|
PARITY |
|
|
|
Primigravida |
72 |
42.6% |
|
Primipara |
52 |
30.7% |
|
Multipara |
45 |
26.6% |
|
PLACE OF STAY |
|
|
|
Urban |
111 |
65.6% |
|
Rural |
58 |
34.3% |
|
ILLNESS OBSERVED |
|
|
|
Hypothyroidism |
33 |
19.5% |
|
Diabetes Mellitus |
51 |
30.1% |
|
Asthma |
4 |
2.3% |
|
Hypertension |
10 |
53.2% |
|
Anaemia |
5 |
2.9% |
|
Uti |
35 |
20.7% |
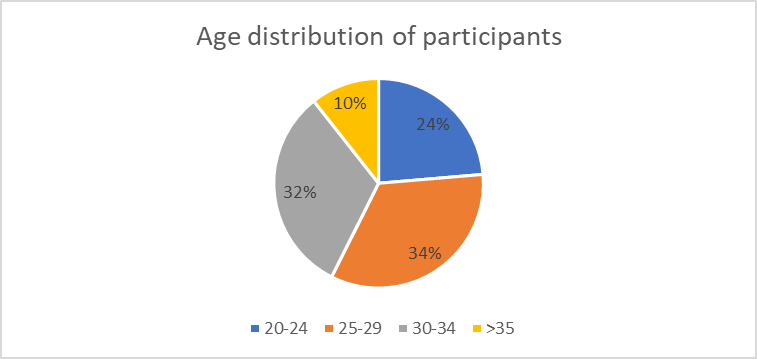
Figure 1 Age distribution of participants
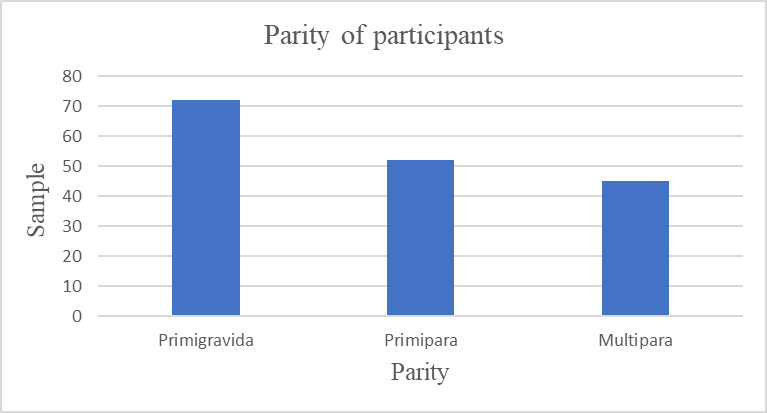
Figure 2 Parity of participant
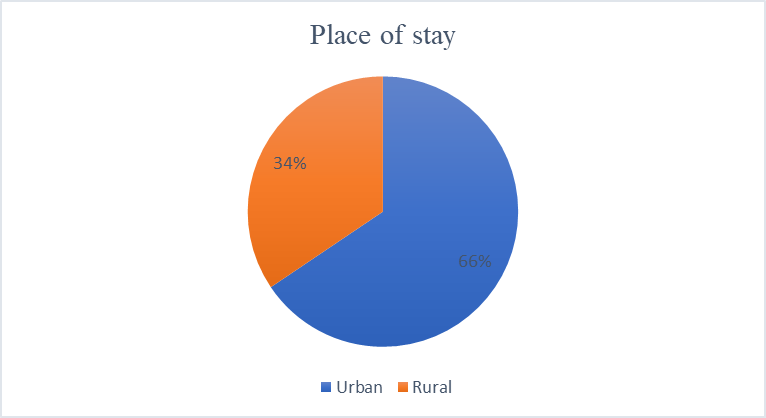
Figure 3 Place of stay
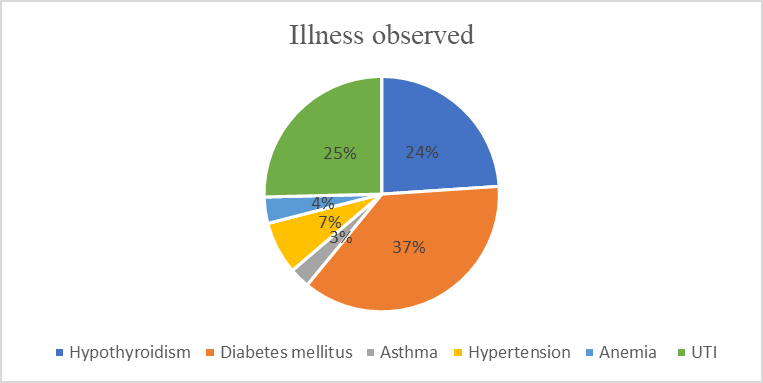
Figure 4
Table 2
|
Dosage form |
Sample |
|
Injection |
135 |
|
Tablet |
985 |
|
Capsule |
57 |
|
Syrup |
46 |
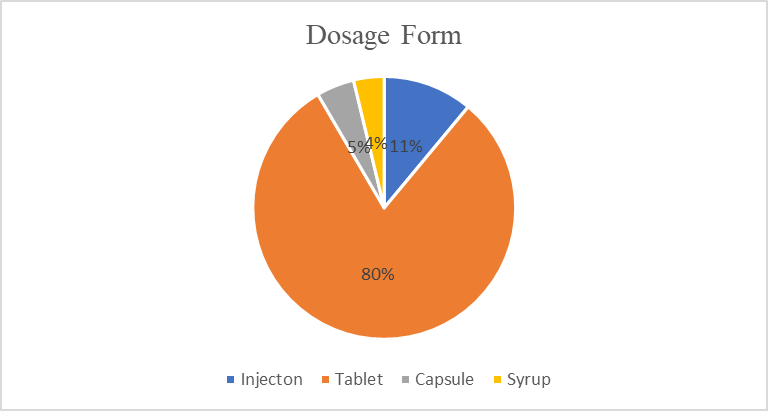
Figure 5
Table 3
|
Route of administration |
Sample |
|
Oral |
850 |
|
Intravenous (IV) |
50 |
|
Vaginal |
13 |
|
Intramuscular |
82 |
|
Subcutaneous |
6 |
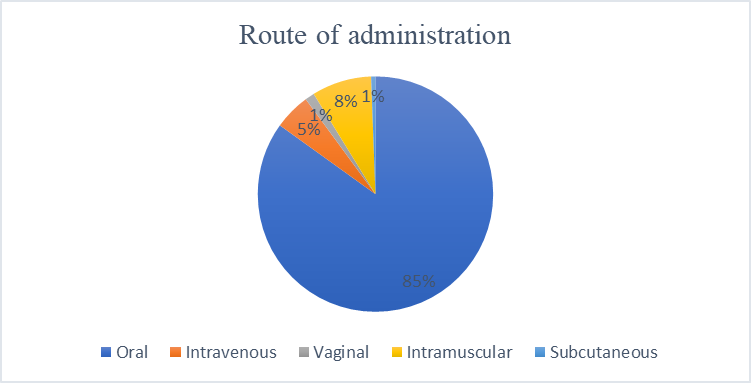
Figure 6
Table 4 USFDA Categorization
|
CATEGORY |
SAMPLE |
|
CATEGORY A |
185 |
|
CATEGORY B |
403 |
|
CATEGORY C |
288 |
|
CATEGORY D |
13 |
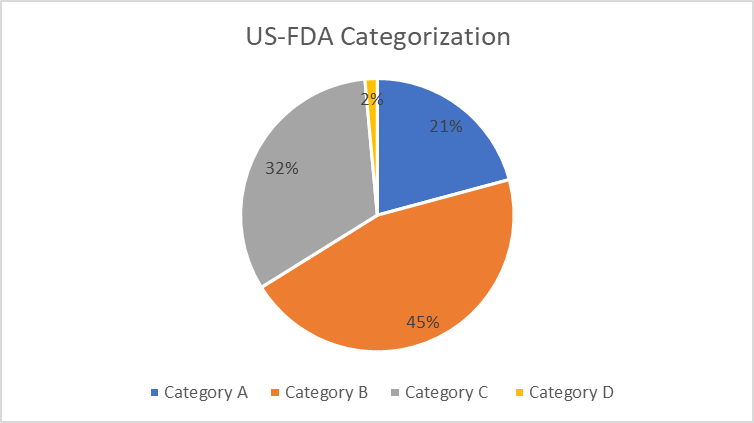
Figure7
Table 5: Category A Drugs
|
DRUG |
NUMBER |
PERCENTAGE |
|
Multivitamin and iron supplement |
121 |
72.4% |
|
Thyroid agents |
37 |
22.1% |
|
Antiemetics |
9 |
5.3% |
Table 6: Category B Drugs
|
DRUG |
NUMBER |
PERCENTAGE |
|
Antidiabetic agents |
58 |
17.2% |
|
Analgesics |
53 |
15.7% |
|
Antibiotics |
68 |
20.1% |
|
Antiemetics |
24 |
7.1% |
|
Drugs acting on GIT |
41 |
12.1% |
|
Hormonal drugs |
77 |
22.8% |
|
Antiallergic drugs |
16 |
4.7% |
Table 7: Category C Drugs
|
DRUG |
NUMBER |
PERCENTAGE |
|
Immunizers |
169 |
65.2% |
|
Vit D and calcium supplements |
81 |
31.2% |
|
Antihypertensive agents |
9 |
3.5% |
Table 8: Category D Drugs
|
DRUG |
NUMBER |
PERCENTAGE |
|
NSAIDS |
13 |
100% |
DISCUSSION
Drugs administered during all three trimesters were classified based on USFDA categorization. Majority of drugs prescribed in this study were from category B followed by category C, A and least from category D. Iron /folate combinations were found predominately prescribed medications with the highest consumption seen in first and second trimester.TT (tetanus toxoid) was administered to majority of the pregnant women. Out of all drugs, multivitamins and iron supplements are most of the drugs from category A (72.4%). And in category B hormonal drugs were mostly given (22.8%). TT comprises 65.2% of common drugs from category C. In category D NSAIDS were commonly given. The majority 985 were prescribed in tablet form. Capsule 57, injection 135 and syrup 46 were prescribed respectively. Mainly, the drugs administered in oral route and the least being vaginal.
C0NCLUSION
The study was conducted to assess the prescribing pattern in pregnancy and concluded that among the total of 169 pregnant women participants,33.7% were from age group 25-29 years. Majority of antenatal women were primigravida. A high proportion of drugs were prescribed from US FDA pregnancy risk category B (403), followed by category C (288), category A (185) and least from category D (13). Only few drugs with positive evidence of risk (category D) were found being prescribed and none of the prescribed drug were found to have proven fetal risk (category X). Majority of the study population used safe and appropriate medications according to US FDA risk classification system. Most of patients were prescribed oral drugs. Urinary tract infection occurred most frequently and Nitrofurantoin was most commonly prescribed. The pharmacological class of most frequently prescribed drugs were vitamins/mineral supplements, antibiotics, analgesics, gastro intestinal drugs, anti-emetics medications. Diabetes mellitus was found to be a top most illness observed during pregnancy in which glycomet and insulin were prescribed. Pregnancy supplements have been shown to have positive benefits on both mother and foetal health; therefore, their widespread use is justified. The problem of prescribing medications from category D and X should be addressed by informing prescribers to follow treatment guidelines, even though the drug utilization pattern in this study was encouraging. In order to ensure the more efficient and rationed use of medications, the study necessitates the requirement to implement the relevant WHO recommended core intervention and to develop a health care system by incorporating clinical pharmacist. Thus, study revealed care full prescribing behaviour of physician and increases the awareness of health care providers and women about potential risks of drug use during pregnancy. Therefore, the study reflects good, safe and rational medication practice during pregnancy.
REFERENCES



Shaimol T., Malavika S.*, Shahana C. P., Assessment of Drug Prescribing Pattern in Pregnancy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 1406-1413. https://doi.org/10.5281/zenodo.15614016
 10.5281/zenodo.15614016
10.5281/zenodo.15614016
