1,2Research Scholar, Department of Chemistry, Sheth L.H. Science College, Mansa (Gujarat University), Gujarat, 382845, India.
3Assistant Professor, Department of Chemistry, Gyanmanjari Innovative University, Bhavnagar, Gujarat, 364001, India.
4Associate Professor, Department of Chemistry, Sheth L.H. Science College, Mansa (Gujarat University), Gujarat, 382845, India.
5Assistant Professor, Department of Chemistry, Government Science College, Gandhinagar, Gujarat, 382016, India
Apixaban, a widely used direct oral anticoagulant (DOAC), is pivotal for managing thromboembolic conditions. This study reviews advancements in analytical methodologies, including high-performance liquid chromatography (HPLC) and UV spectrophotometric techniques, utilized for their quantification in various matrices. Pharmaceutical developments, such as formulation strategies, bioavailability improvements, and stability enhancements, have also been explored. Additionally, this study assessed the pharmacokinetic and pharmacodynamic properties of apixaban, along with its clinical implications and safety profile. A comprehensive literature review covering 2015-2024 has been conducted to ensure that the review is current and inclusive, highlighting recent advancements and innovative approaches in the development of analytical methods. These findings underscore the critical need for ongoing research to enhance analytical methodologies and optimize pharmaceutical formulations, aiming to achieve improved therapeutic outcomes for patients treated with apixaban. Future research directions are suggested to address the challenges associated with the long-term use of apixaban and to explore novel applications in various clinical settings.
Analytical chemistry is focused on the separation, quantification and identification of chemical constituents of natural and artificial materials, which are natural and artificial materials composed of one or more compounds or elements. Analytical chemistry can be classified into two primary groups: qualitative analysis, which involves the identification of the chemical constituents that are present in the sample, and quantitative analysis, which estimates the concentration of specific elements or species in the material, i.e., the sample. Pharmaceutical analysis plays a vital role in examining pharmaceutical formulations and bulk drugs in terms of quality control and assurance [1]. Apixaban (Eliquis®) is an oral pyrazole-derived direct factor Xa inhibitor that was developed by Bristol-Myers Squibb (BMS) and Pfizer as a new therapeutic option for the prevention and treatment of thrombotic disorders [2]. The chemical structure of Apixaban is shown in Figure 1.

Figure 1: Chemical Structure of Apixaban
The FDA-approved anticoagulant apixaban (BMS-562247-01), a direct factor Xa inhibitor, is a novel and promising oral antithrombotic agent that selectively acts on activated factor Xa of the blood coagulation cascade. APX was approved in Europe in 2011 for the prophylaxis of venous thromboembolic events in adult patients [3]. Apixaban produces predictable and consistent anticoagulation effects with favourable efficacy and safety profiles in clinical trials, both for the prevention and treatment of a variety of thromboembolic diseases. The pharmacologic and clinical characteristics of apixaban commonly enable it to overcome many of the shortcomings of warfarin therapy [4].
Apixaban has a bioavailability of ~50% and is not substantially altered by dose or when taken with food. The oral absorption of apixaban was rapid, with peak plasma levels occurring approximately 3 hours after dosing. Apixaban has ∼87% protein binding ability. APX and RVX have similar elimination pathways, including metabolism, primarily by cytochrome P450 3A4 (CYP3A4) and biliary and renal elimination, and have relatively similar terminal half-lives (apixaban∼12 hours, rivaroxaban∼10 hours). APX has an approximate bioavailability of 50%, which is relatively independent of the dose or concomitant meal administration. APX was rapidly absorbed, with peak plasma concentrations attained within ~3 hours post dose. Apixaban results in ∼87% protein binding. APX and RVX further exhibit analogous elimination mechanisms, including metabolism, primarily via cytochrome CYP3A4, as well as biliary and renal excretion, and have comparable terminal half-lives (apixaban ∼12 hours, rivaroxaban ∼10 hours) [5]. Anticoagulant agents are used to reduce the possibility of thromboembolic complications. Owing to an imbalance of clotting factors and endogenous anticoagulants, a thrombus can develop because of arterial (thromboembolic disease) or venous (VTE) thromboembolism. Deep vein thrombosis (DVT) and PE are often classified as VTE and are frequently life-threatening tags. DVT and PE are often classified as life-threatening. Direct oral anticoagulants (DOACs) were developed to treat thromboembolic disease, which represents a shift away from vitamin K antagonist (VKA) anticoagulant therapies [6]. APX is a new oral anticoagulant (NOAC) that was licenced for use in nonvalvular AF patients by the US FDA in 2012 for the prevention of stroke and blood clots. It was subsequently approved for DVT and PE in 2014. It was also approved in 2014 to decrease the risk of blood clots (DVT and PE) in patients after knee and hip replacement surgery [7]. This review provides information on different methods that have been reported for the estimation of APX via UV spectrophotometry and HPLC methods. This will be beneficial in the future exploration of method development and validation of APX.
MOLECULAR CHEMISTRY AND SPECTROSCOPIC DATA OF APIXABAN:
Apixaban is a white to pale yellow non hygroscopic crystalline powder, with an aqueous solubility of approximately 0.028 mg/mL (at 24°C). APX is a small molecule chemically described as 1-(4-methoxyphenyl)-7-oxo-6-[4-(2-oxopiperidin-1-yl) phenyl]-4,5,6,7-tetrahydro-1H-pyrazolo [3,4-c] pyridine-3-carboxamide. The molecular formula of APX is C25H25N5O4, which corresponds to a molecular weight of 459.4971 [g/mol]; CAS number 503612-47-3. Apixaban is a nonionizable compound with a partition coefficient at 24°C and a log Po/w of 1.65 (44.7) at pH 7.4 (n-octanol/aqueous buffer). The molecule has no chiral centers; therefore, no stereoisomers exist [8].
1H NMR (CDCl3) δ

Mass spectrum: 460.37 (M+1) in positive mode.
FT-IR: 1630 for -C=O stretch cyclic amide; 1595 for -C=O stretch amide lactam; 3023 for -C-H stretch aromatic [10].
MECHANISM OF ACTION:
There are two broad pathways leading to the clotting cascade: the intrinsic and extrinsic pathways. External injury triggers the extrinsic pathway and leads to hemorrhage from the vascular compartment. This pathway is more rapid than the intrinsic pathway and is dependent on factor VII. The intrinsic pathway is activated by damage to or trauma to tissue within the vascular system; particularly when damage occurs to platelets, platelets are exposed to the exposed endothelium, chemicals, or collagen. These factors include factors VIII, IX, XI, and XII. These two pathways meet at the point of factor X activation to Xa. APX is a direct, oral, highly selective, reversible and very potent FXa inhibitor (inhibitory constant = 0.08 nM [0.037 ng/mL] at 25°C) that does not require antithrombin III to exert its antithrombotic activity. APX specifically inhibits free and clot-bound FXa and prothrombinase activity to prevent the feedback mechanism that promotes further development of the clot [7,11]. A diagram of the mechanism of action is shown in Figure 2.
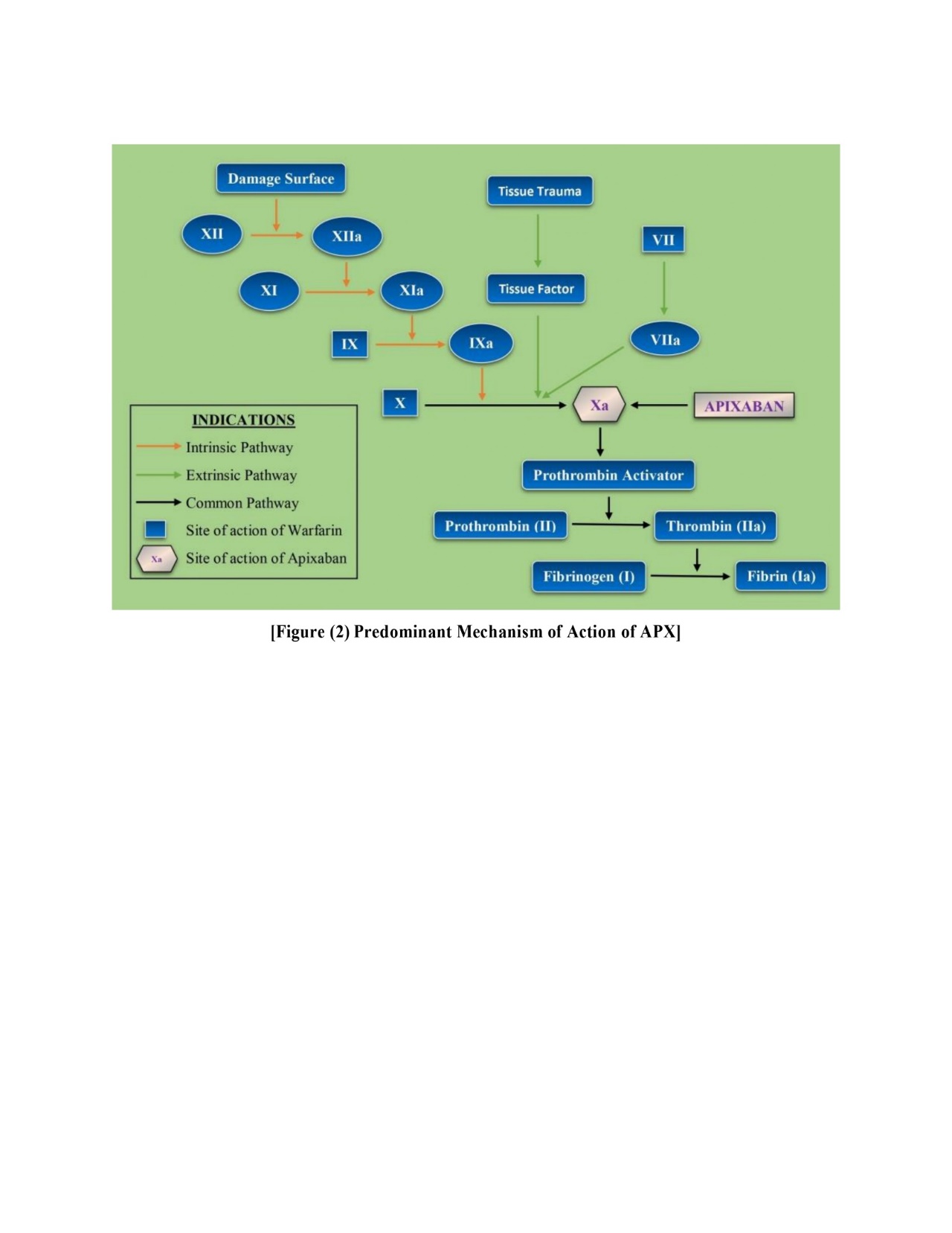
Figure 2: Predominant Mechanism of Action for Apixaban
PHARMACOKINETIC STUDY:
Apixaban has approximately 50% oral bioavailability. It is absorbed from the GI tract after oral administration. The plasma maximum concentration is reached at 3-4 h. Imaging of biomarkers revealed that apixaban has dose-linear pharmacokinetics up to 10 mg. Apixaban: 87% bound to plasma proteins; Vd = 21 h; unchanged apixaban is the only active drug. Apixaban does not have an active metabolite. The orally administered dose is metabolized to 25%. APX is metabolized primarily by the enzyme CYP3A4. Some cytochromes make a small contribution to the metabolism of apixaban. CYP1A2, 2C8, 2C9 and 2J2 contribute to apixaban metabolism in minor amounts. The biotransformation of the 3?oxopiperdinyl moiety generally includes O?demethylation and hydroxylation steps. Excretion of apixaban in the urine and feces. For total elimination, 27% of the patients achieved renal clearance. After intravenous injection, the t½ of apixaban is 5 h, whereas the apparent t½ is 12 h after oral administration. The reason for the wide difference in the half-lives of apixaban between the oral and intravenous routes is its prolonged absorption. P-gp is also responsible for the clearance of apixaban [12].
PHARMACODYNAMIC STUDY:
Apixaban may prevent serious blood clots from forming in a vein (venous thromboembolism) due to a certain heart rhythm disorder (atrial fibrillation) or after hip/knee replacement surgery. If excessive, it affects blood clotting proteins, leading to the risk of severe bleeding. Symptomatic major nosebleeds that occur frequently or do not stop, unexpected tiredness/weakness, unusual pain/swelling/discomfort, excessive bruising, prolonged bleeding from cuts or gums, unexpectedly heavy/prolonged menstrual flow (bleeding (blood in urine, coughing up blood, bloody or coffee-ground vomiting), severe headache, dizziness or fainting, bloody, and difficulty swallowing) [13].
PHARMACEUTICAL DOSAGE AND ADMINISTRATION:
Decreased risk of stroke and systemic embolism in nonvalvular AF patients. For many patients, 5 mg of ELIQUIS is taken orally twice a day. For patients with at least two of the following characteristics, the recommended dose of ELIQUIS is 2.5 mg bid:
INSTRUMENTATION OF UV SPECTROPHOTOMETRY AND HPLC:
UV spectrophotometry provides quick and effective analysis in analytical chemistry. It requires only a small amount of substance (at the mg and µg levels), which is frequently recoverable after testing, and it provides permanent chart recording information because UV spectrophotometry is highly sensitive and selective; moreover, it is useful for identifying substances in complicated combinations and finding minute contaminants [15]. Chromatography is a technique that was first invented by Russian Botanist M.S. Tswett in 1903, but after that, many revolutions and amendments were developed and are still ongoing. High-performance liquid chromatography (HPLC) is one of the most common analytical techniques employed. More than 85% of general pharmaceuticals are analyzed via HPLC [16]. Each chemical entity in the sample mixture has a unique affinity toward the adsorbent material in the column or the mobile phase, thus causing different constituents to move at different rates and separate in an HPLC. It was formerly called high-pressure liquid chromatography since it relies on high-pressure pumps to allow quicker separation. Some of the key interdependent tunable attributes and environmental powers for HPLC separation are mobile phase properties, such as type and its characteristics (e.g., polarity), composition, flow rate, pH stationary phase nature, and environmental factors, such as temperature- and detector-dependent factors [17].
ANALYTICAL METHOD VALIDATION:
The validation of an analytical method is a process that is established by laboratory studies to evaluate the performance uniqueness of the procedure to meet the requirements for its intended use. The method validation process for analytical procedures begins with planned and systematic collection by the applicant of the validation data to support analytical procedures [18].
Components of Method Validation:
The following are examples of analytical performance features that might be assessed as part of method validation:
REPORTED METHODS OF APIXABAN:
The reported UV spectrophotometric methods for the assessment of apixaban are shown in Table 1.
Table 1. Reported UV Spectrophotometric Methods for Assessment of Apixaban
|
Sr. No. |
Title |
Description |
Reference |
|
1. |
Spectrophotometric Determination of Apixaban in Bulk Drug and Oral Dosage Formulation |
Solvent: Water, Methanol Wavelength: 680 nm Linearity: 5-50 µg/mL %RSD: 1.97 |
[19] |
|
2. |
Method Developed for the Determination of Apixaban by using U.V. Spectrophotometric |
Solvent: Water, Methanol, Ethanol Wavelength: 278 nm Linearity: 10-80 µg/mL %RSD: 0.02 |
[20] |
|
3. |
Method Development and Validations of Apixaban in Bulk and Its Formulations By UV-Spectroscopy (Zero Derivatives) |
Solvent: Methanol Wavelength: 279 nm Linearity: 5–25 µg/mL %RSD: 0.790 |
[21] |
|
4. |
Method Development and Validations of Apixaban in Bulk and its Formulations by UV-Spectroscopy (Area Under Curve) |
Solvent: Methanol Wavelength: 269 nm and 289 nm Linearity: 5-25 µg/mL %RSD: 0.988 |
[22] |
|
5. |
Method Development and Validations of Apixaban in Bulk and its Formulations by UV-Spectroscopy (Zero Derivatives and Area Under Curve) |
Solvent: Methanol Wavelength: 279 nm and 269-289 nm Linearity: 5-25 µg/mL %RSD: 0.790 and 0.988 |
[23] |
|
6. |
Development and Validation of UV Spectrophotometric Methods for Apixaban in Tablets |
Solvent: Methanol Wavelength: 276 nm Linearity: 1-60 µg/mL %RSD: <1.8 |
[24] |
The reported HPLC methods for the assessment of apixaban are shown in Table 2.
Table 2. Reported HPLC Methods for Assessment of Apixaban
|
Sr. No. |
Title |
Description |
Reference |
|
1. |
Stability Indicating RP?HPLC Method Development and Validation for Determination of Nine Impurities in Apixaban Tablet Dosage Forms Robustness Study by Quality by Design Approach |
Stationary phase: Zorbax RX C18 (250 mm × 4.6 mm, 5 μm particle size) Mobile phase: 0.03 M Ammonium acetate and Acetonitrile (90:10 v/v) Flow rate: 1.0 mL/min. Conc. range: 0.1-1.6 μg/ml. Detection: 280 nm Temperature: 40 ºC Retention time: 13 min Tailing factor: 1.52 Theoretical plates: 9878 %RSD: <2 |
[25] |
|
2. |
A Green HPLC Method for the Determination of Apixaban in Pharmaceutical Products: Development and Validation |
Stationary phase: Agilent C18 (250 mm × 4.6 mm, 5 μm particle size) Mobile phase: Trifluoroacetic acid (TFA) solution (0.1%) and Ethanol (65:35, v/v) Flow rate: 1.0 mL/min. Conc. range: 5-30 µg/mL Detection: 276 nm Temperature: 25 ºC Retention time: 4.51 min Tailing factor: 1.30 Theoretical plates: 5,651 %RSD: 0.10 |
[26] |
|
3. |
Stability Indicating Method Development and Validation for Anticoagulant Drug Apixaban in Apixaban Drug Substance and Drug Product |
Stationary phase: Inertsil ODSC18 (150 mm × 4.6 mm, 5 μm particle size) Mobile phase: A buffer solution pH 4 and ACN in a ratio of 50:50 v/v Flow rate: 1.2 mL/min. Conc. range: 7.5-37.5 µg/mL Detection: 230 nm Temperature: 25 ºC Retention time: 2.2 min Tailing factor: 1.37 Theoretical plates: 4572 %RSD: 0.40 |
[27] |
|
4. |
A stability Indicating Method Development and Validation of Apixaban in Pharmaceutical Dosage Form by using RP-HPLC and In-Vitro Evaluation of Apixaban Suspension Delivery Through Enteral Feeding Tubes |
Stationary phase: Zorbax C-18, (150 mm × 4.6 mm, 5 µm particle size) Mobile phase: Ammonium formate Buffer: Acetonitrile (65:35 v/v) Flow rate: 1.1 mL/min. Conc. range: 50-300 μg/ml. Detection: 280 nm Retention time: 4.0 min Tailing factor: 1.12 Theoretical plates: 9116 %RSD: 0.69 |
[28] |
|
5. |
Development and Validation of a New High Performance Liquid Chromatography Method for Determination of Apixaban Isomers |
Stationary phase: Chiralpak IA (250 mm × 4.6 mm × 5 µm particle size) Mobile phase: n-Hexane: Toluene: Methanol: Ethanol (65:15:10:10 v/v) Flow rate: 1.1 mL/min. Conc. range: 50-500 μg/ml. Detection: 290 nm Temperature: 25 °C ± 2 °C Retention time: 1.0 min %RSD: 0.33 |
[29] |
|
6. |
Development and Validation of a Stability Indicating RP-HPLC Method of Apixaban in Commercial Dosage Form |
Stationary phase: Ascentis Express® C18 (100 mm × 4.6 mm × 2.7 µm particle size) Mobile phase: Phosphate buffer and Acetonitrile (various v/v) Flow rate:1.3 mL/min. Conc. range: 20-90 ppm Detection: 225 nm Temperature: 35 °C Retention time: 6 min Tailing factor: 0.85 Theoretical plates: 5538 %RSD: 0.069 |
[30] |
|
7. |
HPLC Method Development and Validation for the Determination of Apixaban and Clopidogrel in Novel Fixed-Dose Combination Tablets |
Stationary phase: BDS Hypersil C18 (150 mm × 4.6 mm × 4.5 μm) Mobile phase: Acetonitrile (ACN) and Trifluoroacetic acid (TFA) in the ratio 48:52 (v/v) Flow rate: 0.9 mL/min. Conc. range: 1.25-10 μg/ml. Detection: 210 nm Temperature: 45 ºC Retention time: 2.46 min Tailing factor: 1.073 & 1.085 Theoretical plates: 8561 & 8552 %RSD: 1.8 & 1.13 |
[31] |
|
8. |
Formulation Development and Stability Indicating HPLC Assay of Tablets of Apixaban |
Stationary phase: Purospher Star RP-18e (250mm × 5 µm × 6mm) Mobile phase: Water: Acetonitrile (60:40 v/v) + 0.1 % TEA Flow rate: 1.0 mL/min. Conc. range: 5-30 μg/ml. Detection: 280 nm Retention time: 5.56 min %RSD: <2 |
[32] |
|
9. |
Development, Validation and Application of a new HPLC-DAD Method for Simultaneous Quantification of Apixaban, Dabigatran, Edoxaban and Rivaroxaban in Human Plasma |
Stationary phase: LiChroCART Purospher Star C18 column; 55 mm × 4 mm, 3 μm particle size) Mobile phase: Acetonitrile: water (90:10, v/v) Flow rate: 1 mL/min. Conc. range: 0.017-5.28 μg/ml. Detection: 300 nm Temperature: 30 ºC Retention time: 2 min %RSD: 0.12 |
[33] |
|
10. |
Full Factorial Experimental Design for Development and Validation Of RP-HPLC Method For Estimation of Apixaban in Bulk and Pharmaceutical Formulations |
Stationary phase: C18 column Waters X Bridge (250 mm × 4.6 mm × 5 µm particle size) Mobile phase: Acetonitrile, Methanol, Water, Buffer (10-30% v/v) pH range: 5-7 Flow rate: 1.0 mL/min. Conc. range: 5-50 μg/ml. Detection: 277 nm Temperature: Ambient Retention time: 2.9 min Tailing factor: 0.82 Theoretical plates: 3931 %RSD: 1.19 and 1.79 |
[34] |
|
11. |
Using the AQbD Approach, the Development and Validation of a Simple, Rapid Stability Indicating Chromatographic Method for Quantification of Related Impurities of Apixaban |
Stationary phase: Zorbax Stable Bond Phenyl, 150 mm × 4.6 mm × 5 μm particle size) Mobile phase: water, acetonitrile, methanol and perchloric acid (various ratio) Flow rate: 1.2 mL/min. Conc. Range: 0.4-2.25 μg/ml. Detection: 278 nm Temperature: 45 ºC %RSD: 1.4 |
[35] |
|
12. |
Development and Validation of Stability Indicating RP-HPLC Method on Core-Shell Column for Determination of Degradation and Process Related Impurities of Apixaban—An Anticoagulant Drug |
Stationary phase: Ascentis Express® C18 (4.6 mm × 100 mm × 2.7 µm particle size) Mobile phase: 0.02 M ammonium dihydrogen/ thiophosphate buffer and Acetonitrile 70:30 (v/v) Flow rate: 1.0 mL/min. Conc. Range: 500 μg/ml. Detection: 225 nm Temperature: 35 ºC Tailing factor: 1.05 Theoretical plates: 90016 %RSD: <2 |
[36] |
FUTURE RESEARCH DIRECTIONS:
This study investigated the binding interactions between apixaban and various chromogenic reagents to form stable complexes that can aid in the development of analytical methods. Techniques such as UV spectrophotometry and high-performance liquid chromatography (HPLC) have been refined to enhance the quantification and analysis of apixaban across different matrices. Research has emphasized the need to optimize these methods to achieve greater accuracy, sensitivity, and reliability in apixaban measurement, which is crucial for effective therapeutic monitoring. A separate focus is placed on developing an analytical method using normal-phase HPLC, capitalizing on its ability to separate compounds based on polarity for improved detection and characterization. This normal-phase HPLC method aims to increase the resolution, reproducibility, and sensitivity of the analysis of apixaban in pharmaceutical and biological samples. The study also explored the use of nanoparticles that bind with apixaban to create a stable complex for innovative analytical applications. The large surface area and reactivity of nanoparticles increase their selectivity and efficiency for the detection of apixaban. This approach supports advanced drug monitoring, stability assessments, and in-depth pharmacokinetic and pharmacodynamic evaluations. By refining these methodologies, research contributes to better quality control and more reliable assessments of the stability and formulation performance of apixaban. Overall, these results may help improve therapeutic efficacy and ultimately facilitate the development of personalized treatment strategies. Future research directions are proposed to overcome ongoing challenges and explore new clinical applications.
CONCLUSION:
Apixaban has emerged as a crucial anticoagulant with a strong safety profile and efficacy in the prevention and treatment of thromboembolic conditions. This comprehensive review highlights the analytical methodologies, pharmacokinetic properties, clinical applications, and challenges associated with its pharmaceutical formulation. Current analytical techniques, including HPLC and UV spectrophotometric methods, ensure precise quantification and monitoring, which are essential for both quality control and clinical pharmacology. Furthermore, the pharmaceutical advancements in developing formulations that optimize bioavailability and patient adherence represent significant progress in this field.
ACKNOWLWDGEMENTS:
The authors are grateful to Dr. J. R. Shukla, principal of Sheth L.H. Science College, Mansa for providing detailed information regarding anticoagulant drug Apixaban.
REFERENCES





Devayan Vyas*, Amit Sapara, Nikunj Dave, Kartik Vyas, Kiran Nimavat, Analytical and Pharmaceutical Consideration of the Anticoagulant Drug Apixaban: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 1159-1170. https://doi.org/10.5281/zenodo.15185692
 10.5281/zenodo.15185692
10.5281/zenodo.15185692
