Department of Pharmaceutical Quality Assurance, A.R. College of Pharmacy & G.H Patel Institute of Pharmacy, Vallabh Vidyanagar, Anand, Gujarat, India. 388120.
Acrylamide, a potentially harmful compound, is formed in starchy foods during high-temperature cooking processes such as baking, frying, and roasting through the Maillard reaction between asparagine and reducing sugars. It is absent in raw foods but is found in significant quantities in everyday food items. This review summarizes various analytical methods employed for the detection and quantification of acrylamide in different food matrices. It also highlights the key factors influencing acrylamide formation, including cooking temperature and time, pH, surface area, moisture content, food composition, cooking methods, fertilizer use, harvesting, and storage conditions. Acrylamide is recognized as a mutagen with notable genotoxic, neurotoxic, and hepatotoxic effects. The European Food Safety Authority (EFSA) has reported its ability to induce neurotoxicity via occupational exposure, and its impact on lipid metabolism has been linked to oxidative stress-related liver damage. Additionally, reproductive toxicity and developmental effects during prenatal and postnatal stages are discussed. The review also includes FDA guidance aimed at reducing acrylamide levels in food, emphasizing the importance of food safety and regulatory strategies.
For thousands of years, people have used heat to cook their food. Thermal processing has a great importance in terms of microbiological safety, nutritional quality, and the desired sensory properties, such as color, texture, and flavor; however, undesirable chemicals have arisen as problems associated with food processing techniques. (3) Heating of food induces chemical reactions that lead to the formation of heat-induced toxic substances, the so-called thermal process contaminants. Acrylamide has recently been detected at high amounts in everyday foodstuff, mainly in fried and baked starch-enriched food (1). It is formed mainly by a reaction of reducing sugars with asparagine when heating the food to >120°C. Food composition and processing conditions have a major effect on acrylamide formation. Based on food contents, the average daily intake of acrylamide for adults in western countries was estimated to be in the range of 0.2 to 1.4 μg/kg body weight, with 0.5 μg/kg body weight probably as the best guess. However, depending on the different diets in younger age groups, a higher exposure is assumed in children and adolescents, reaching up to 3.4 μg/kg body weight daily (95th percentile) in a Berlin cohort (2).Human exposure to AA has become a worldwide concern after the publication of International Agency for Research on Cancer (International Agency for Research on Cancer and World Health Organization 1994) where it has declared that AA is a probable human carcinogen(class 2A), on the basis of its carcinogenicity in rodents and neurotoxicity in humans.(4)
Fig 1: structure of acrylamide.
Table 1: Physico-chemical properties of acrylamide. (5)
|
Acrylamide |
|
|
IUPAC |
Acrylamide |
|
Stum Formula |
C3h5no |
|
Molecular Weight |
71.078 |
|
Properties |
White, Crystlline Solid |
|
Density |
1.127 G/Cm3 |
|
Melting Point |
84-84.5 |
|
Boiling Point |
125 C At 3.3 Pa |
|
Vapor Pressure |
0.9 Pa |
|
Log Pow |
-0.67 To 1.65 |
|
Solubility In Water |
2.115 G/L |
|
Mak Commission Classification |
Skin Absorption H Carcinogen Category 2 Germ Cell Mutagen Category 2 |
Acrylamide is not present in raw foods but forms when they are cooked at high temperatures (above 120°C) through methods like baking, frying, or roasting. This happens because of a reaction called the Maillard reaction, which occurs between an amino acid called asparagine and reducing sugars (like glucose or fructose) when heated.
Here’s a simpler breakdown of the process A (5):
•Acrylamide Formation: When food is heated, asparagine (an amino acid) reacts with reducing sugars (like glucose and fructose) to produce acrylamide.
•Maillard Reaction: This reaction, which creates acrylamide, was first identified by Louis Maillard in 1912. It's a complex series of chemical changes that also give food its brown color and distinctive flavor.
•Sugars Involved: In plants, common reducing sugars include glucose, fructose, and maltose. Sucrose (table sugar) is not a reducing sugar and doesn’t directly participate in this reaction.
•Other Products: The Maillard reaction also produces melanoidin pigments, which make foods brown, and other compounds that add flavor and aroma.
•Challenges: Reducing acrylamide levels can also reduce the desirable colors and flavors produced by the Maillard reaction, making it tricky for food manufacturers tomanage.
Here’s a simplified explanation of the processB (5):
•Initial Reaction: A reducing sugar (like glucose) reacts with an amino group to form a Schiff base (an imine with a C=N group).
•Cyclization: If the sugar is an aldose (like glucose), the Schiff base cyclizes into a product called an N-substituted aldosylamine (e.g., glucosylamine).
•Amadori Rearrangement: The aldosylamine undergoes an acid-catalyzed rearrangement to form a 1,2-enaminol, which can convert into an N-substituted 1-amino-2-deoxyketose. These are known as Amadori rearrangement products. Similar rearrangements occur with ketoses (like fructose) and are called Heyns rearrangement products.
•Further Reactions: Amadori and Heyns products can undergo further reactions, such as enolization, deamination, dehydration, and fragmentation. These lead to the formation of various reactive carbonyl compounds (like deoxyosones, furfurals, furanones, and pyranones).
•Strecker Degradation: These carbonyl compounds can react with amino acids through a process called Strecker degradation. This process produces aldehydes and α-aminoketones which contribute desirable flavors and aromas to food, such as fruity or malty notes.
•Undesirable Formation: However, when asparagine (an amino acid) reacts with carbonyl compounds, it can produce acrylamide, an undesirable compound. The process involves forming a Schiff base, then decarboxylating it to form 3-aminopropionamide, which further converts to acrylamide through the removal of ammonia.
A schematic diagram of absorption, distribution, metabolism, and excretion of acrylamide is given below. After consumption, acrylamide is rapidly absorbed and distributed to all tissues in humans by systemic circulation. It can be also found (6). Acrylamide is extensively converted to a range of metabolites that are excreted in urine. It can also interact with proteins and DNA resulting in covalent adducts. The main pathways of acrylamide biotransformation are given below. Acrylamide has an α, β-unsaturated structure with an amide group making it an electrophilic compound. Cellular nucleophiles react with acrylamide’s double bond by the Michael addition. These nucleophiles include the –SH of cysteine, homocysteine, and glutathione; α-NH2 groups of free amino acids and N-terminal amino acid residues of proteins, the ε-NH2 of lysine, and the ring NH group of histidine. (7) Sulfhydryl groups in glutathione and proteins are the main targets for acrylamide, and amino groups found in proteins are also targets although to a lesser extent. (8) Acrylamide is partly converted to an epoxide glycidamide, which is also an electrophile, in vivo through oxidation by cytochrome P450 2E1 in phase I metabolism. Therefore, like acrylamide, glycidamide covalently bonds to cellular components containing sulfhydryl and amino groups. Attack by sulfhydryl and amino groups or water results in the ring opening of the epoxide. Glycidamide can be further hydrolyzed by an epoxide hydrolase to glyceramide (2,3-dihydroxypropionamide). (7) Nucleophilic nitrogens in DNA are also susceptible to form adducts especially with glycidamide, which is thought mainly to be responsible for the genotoxicity (9). Orally ingested acrylamide in rodents and humans is extensively conjugatedwith glutathione in phase II metabolism. After degradation and acetylation of the conjugate, the resulting mercapturic acid N-acetyl-S-(2-carbamoylethyl)-l-cysteine (AAMA) is excreted with urine. Glutathione conjugation is of importance to reduce acrylamide reactivity against cellular components. Another important aspect of the conjugation of acrylamide with glutathione is that it is less converted to glycidamide. Depletion ofintracellular glutathione in rat hepatocytes and lung fibroblasts (V79) cells has shown to result in a significant induction of DNA strand breaks after incubation with 1mlAA. (7)
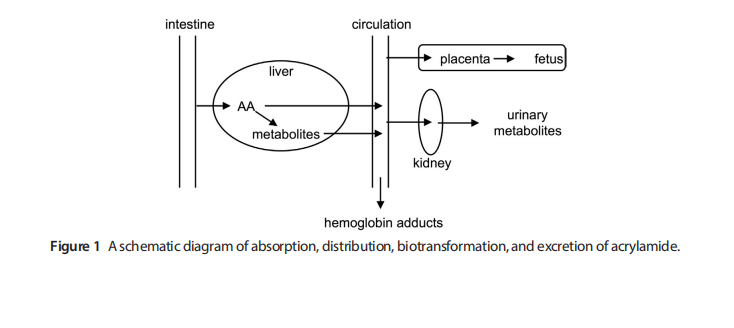
Figure 2: a schematic diagram of absorption, dstribution, biotransformatio, and execretion of acrylamide. (7)
Glycidamide can also be conjugated with glutathione and is excreted with urine after metabolic conversion to the mercapturic acids N-acetyl-S-(2-carbamoyl- 2-hydroxyethyl)-l-cysteine (GAMA) and N-acetyl-S-(1-carbamoyl-2-hydroxyethyl)- l-cysteine (iso-GAMA)which are excreted with urines.Toxicokinetic studies on humans show that nearly 60% of absorbed acrylamide is excreted in the urine mostly (86%) as GSH-conjugates and that unchanged acrylamide accounts only for 4.4% of the up taken dose. Only marginal amounts of unchanged glycidamide could be found in human urine.(10)
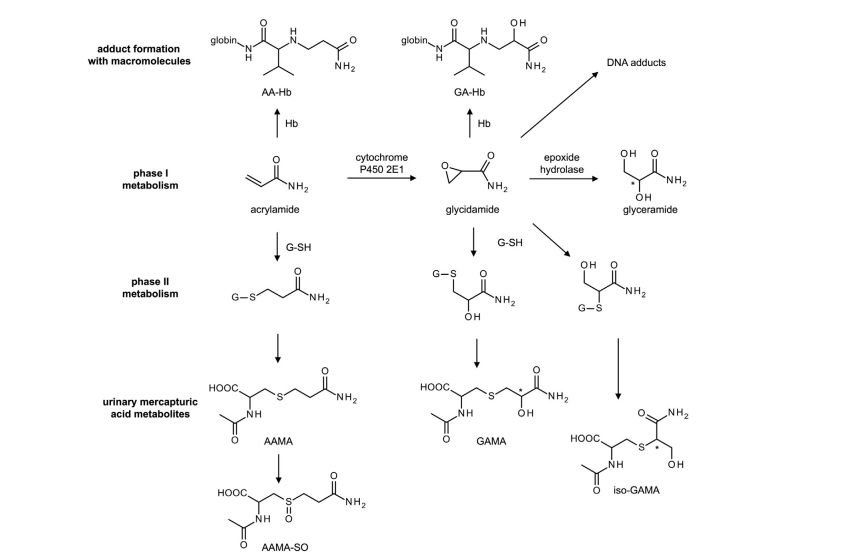
Figure 3: Biotransformation of acrylamide in human. * indicates chiral carbons.(7)
|
Sr No. |
Method |
Parameters |
Ref. No. |
|
1 |
HPLC-UV Quantitative Analysis of Acrylamide in Snack Foods of India |
Mobile phase: water, acetonitrile and formic acid Wavelength: 210 nm LOQ value: 17.08 µg/kg LOD value: 5.12µg/kg Stationary phase: ODS-2 column Acrylamide concentration: In deep fat fried snack: 788.99 - 4191.82 µg/kg deep fat fried food: 372 µg/kg to 6391 µg/kg baked food: 435-3147 µg/kg breakfast cereal: 434-1307 µg/kg |
43 |
|
2 |
HPLC-UV quantitative analysis of acrylamide in baked and deep-fried Chinese foods
|
Mobile phase: acetonitrile-water Wavelength: 210 nm LOQ value: 25 μg/kg LOD value: 8.0 μg/kg Flow rate: 0.40 mL/min Retention time: 8.90 min |
44 |
|
3 |
Determination of Acrylamide in Starch-Based Foods by HPLC with Pre-Column Ultraviolet Derivatization |
Stationary phase: ODS-3 C18 column (250 mm × 4.6 mm) Mobile phase: 7% (v/v) methanol in 0.025 mol/L sodium dihydrogen phosphate Wavelength: 215 nm Linearity: 50–2000 µg/L R2: LOQ value: 50 µg/kg LOD value: 15 µg/kg Flow rate: 1.0 mL/min Retention time: Injection volume: 20 µL |
45 |
|
4 |
Acetone extraction and HPLC determination of acrylamide in potato chips |
Stationary phase:C18-AQ (2 × 250 mm) Mobile phase: acetonitrile-water Wavelength:202 nm Linearity: 20-400 ng g-1 R2: 0.999 LOQ value:3.14 ng g-1 LOD value:2.46ng g-1 Flow rate: 0.15 ml min-1 Retention time: 8 min Injection volume:20 µl |
46 |
|
5 |
HPLC-MS Detection for Acrylamide Determination in Black Ripe Olives |
Stationary phase:ODS-2 (5 µm, 25 cm × 4.6 mm) Mobile phase:100% water acidified with formic acid (0.06%) R2: 0.9995 LOQ value: 11µg/kg LOD value:4µg/kg Flow rate: 0.4 mL/min Retention time:14.4 min |
47 |
|
6 |
RP-HPLC-DAD studies on acrylamide in cereal-based baby foods
|
Stationary phase:Synergi Hydro-RP 80 A with 5 mM sodium 1-heptanesulfonate Mobile phase: water/acetonitrile (97/3, v/v) Wavelength: 200 nm Relative standard deviations:<5.0% LOQ value: LOD value:10.0 μg/kg Acrylamide concentration: In instant baby foods:10.8–15.7 μg/kg In candy-bars:19.2–59.9 μg/kg Ready-to-eat:39.0–61.2 μg/kg Cakes:13.3–49.5 μg/kg |
48 |
|
7 |
Determination of acrylamide in cooking oil by HPLC-DAD |
Stationary phase:Agilent ZORBAX HILIC Plus 4.6 × 50 mm, 3.5 μm 0.2 mL/min Mobile phase: Isocratic elution: A = 3% 5 mM acetic acid B = 97% acetonitrile Wavelength:210 nm nm R2:0.9992 LOQ value:108 ng/mL LOD value:32.4 ng/mL Flow rate: 0.15 ml min-1 Retention time: 10 min Injection volume:5 μL |
49 |
|
8 |
VALIDATION OF HPLC-UV METHOD FOR SIMULTANEOUS ANALYSIS OF ACRYLAMIDE AND GLYCIDAMIDE IN VOLUMETRIC ABSORPTIVE MICROSAMPLING |
Stationary phase:e C18 SunfireTMWaters® column (5 µm; 250 mm x 4.6 mm) Mobile phase: 6 mmol potassium dihydrogen phosphate pH 3.5–methanol (96:4 v/v) Wavelength: 210 nm Linearity: 1.0-100.0 µg/ml LLOQ value: 1.0 µg/ml Flow rate: 0.5 ml/min |
50 |
|
9 |
Determination of Trace Acrylamide in Starchy Foodstuffs by HPLC
|
Stationary phase:C18 column (250 × 4.6 mm i.d., 5 μm) Mobile phase:methanol/water (10:90, v/v) Wavelength: 200 nm Linearity: 4–4000 ng/mL R2: >0.9999 LOQ value: 20ng/g LOD value: 5ng/g Flow rate: 3 mL/min Retention time: Injection volume: |
|
In simpler terms, when food is cooked at high temperatures, a chemical reaction occurs between an amino acid called asparagine and sugars in the food. This reaction forms a compound that eventually turns into acrylamide, a substance that has been found to increase in food as cooking temperatures rise.However, prolonged heating shows decreased acrylamide content due to degradation.Whereas cooking food products at a lower temperature for a prolonged time reduces the acrylamide content.(11). The formation of acrylamide in food diminishes under lower pH conditions during the frying or baking of carbohydrate-rich foods.the formation of acrylamide in food is influenced by pH levels. When the pH is lower (more acidic), the chemical groups involved in making acrylamide become protonated, which means they can’t react as easily. This process helps to reduce the amount of acrylamide formed during cooking. when the cooking environment is more alkaline (basic), it encourages acrylamide formation in food. In these conditions, the amino groups lose their extra hydrogen ions, becoming more reactive. This makes it easier for these groups to interact with sugars and start a chain reaction that leads to the creation of acrylamide. (12). How thick the slices of food are can affect how much acrylamide forms during cooking. Thin slices cook more evenly and quickly, reducing acrylamide levels. On the other hand, thicker slices need higher temperatures to cook through, which can lead to more acrylamide. For example, potato slices that are 1/4 inch thick have more acrylamide compared to 1/2-inch-thick slices because they cook faster and more evenly. (13)
5.2 Moisture content
Moisture content refers to the amount of unbound water in food products, which plays a significant role in the formation of acrylamide in food products. The moisture content of the food decreases with an increase in temperature, promoting acrylamide formation. In the case of bread, the moisture content alters the acrylamide concentration and the nature of the dough during the baking process. A lower moisture content is likely to be associated with the Maillard reaction, which plays a significant role in the decarboxylation of the Amadori compound. This, in turn, favors the formation of acrylamide in the food by not hindering the reaction caused by excess water molecules. (14). Considering that the moisture content at the external surface of food products is much lower than the internal surface, acrylamide formation tends to be higher at the outer surface of food products such as French fries, cookies, chicken nuggets, sweet biscuits, and breakfast cereals.In addition to moisture content, water activity is also associated in influencing acrylamide formation; when the water activity ranges between 0.4 and 0.8 and the moisture content is <5% it is likely to favor the Maillard reaction, subsequently leading to the formation acrylamide in food products(15-16)
The formation of acrylamide depends on the food composition. Various studies have reported that the presence of exogenous phenolics enhances the formation of acrylamide. However, the phenolic antioxidants did not affect the acrylamide formation. (17)
Acrylamide formation is comparatively lower when food is cooked using a moisture-less oven or dry heating than in deep-frying, where the degree or level of browning is high. In contrast, the degree of browning in a moisture-less oven is slight, and acrylamide formation was observed at temperatures above 120 ?C. However, in some cases, microwave cooking influences the acrylamide production as it favors the condition for the Maillard reaction compared to traditional cooking methods. Cooking meat, chicken, and shrimp nuggets using the traditional cooking method increased the acrylamide content compared to the industrial cooking method, owing to differences in the cooking temperature and time. The lowest acrylamide content was found in chicken nuggets at 7.3 ng g−1 fried using the industrial process for 3 min at 180 ?C. The highest was found in shrimp nuggets at 27 ng g−1, which were fried using the traditional method for 6 min at 220 ?C, as reported by (18)
Fertilizers, especially nitrogen ones, can increase acrylamide levels in crops like potatoes by boosting reducing sugars. How long crops are allowed to grow and the weather conditions also affect acrylamide levels; colder (8-12°C) and warmer (25-30°C) temperatures can both raise acrylamide content. Potatoes stored for longer periods develop more reducing sugars and acrylamide. Higher nitrogen fertilizer and longer storage time lead to more acrylamide and asparagine. Additionally, cooking at high temperatures, with low moisture, or in alkaline conditions, increases acrylamide in food. Understanding how acrylamide forms and interacts with biological molecules is important because it has potential health risks. (19)
Acrylamide produce various type of toxicity in human body.it will affect various organ organ and normal function in body.the toxicity which are produce by acrylamide is following.
Acrylamide-a known by-product in the cooking of specific foods-is a mutagen that is commonly regarded as having significant genotoxic potential. It has been demonstrated to be potent in the induction of sister chromatid exchanges to cause aneuploidy and polyploidy. (20). It combines with cellular constituents in the human body to form adducts with bases of nucleic acid acids, thereby providing hazardous products, which could have genotoxic influence. The major concern is the biologically active metabolite of acrylamide, glycidamide (GA), since although acrylamide itself has very low reactivity and is considered to be an inactive mutagen at this point, its conversion to glycidamide increases its potential to induce mutations. The biotransformation leads to DNA adduct formation in experimental models as well as in humans: notably to lymphocytes and DNA damage that have been highlighted by analyses by comet assay.The biotransformation of acrylamide is complex, with more time taken in forming glycidamide compared to detoxification through glutathione. Estimated acrylamide intake through dietary exposure places the MOEs below 500.The compound has been debated on whether it acts at consumer-relevant doses as a genotoxic carcinogen. (21). However, the EFSA has pointed out that despite all the debate, the framework for MOE is applicable and valid for the risk evaluation of acrylamide as a carcinogen. Additionally, acrylamide and glycidamide are two compounds that are thought to be the cause for mutations in the tumor suppressor gene TP53. Various tumors have been shown to occur in models treated with acrylamide, such as in the ovaries, lung, and breast. (22). International Agency for Research on Cancer has categorized acrylamide as a "probable human carcinogen," while the US National Toxicology Program has classified it as a "reasonably anticipated human carcinogen." Its carcinogenic potential would arise from its capability to cause DNA adducts, which are behind gene mutations and chromosomal abnormalities that may lead to cancer. Acrylamide and its metabolite form covalent adducts with DNA, proteins, and hemoglobin, and are likely to cause lung carcinomas in mouse embryonic fibroblasts. The hemoglobin adducts can be used as biomarkers for exposure to acrylamide and glycidamide. (22)
6.1.1. Evidence of genotoxicity and carcinogrnrcity of acrylamide
Acrylamide exposure caused oxidative stress and increased levels of malondialdehyde (MDA) levels in a rat model leading to lipid peroxidation, and histopathological changes, including degeneration of focal gliosis in the brain, which was observed following oral administration of acrylamide at concentrations of 5 to 20 mg/kg per day for 60 days.Other studies have indicated that acrylamide could induce DNA adducts in the lungs and then histone modifications with epigenetic alterations. That was after a mouse model had received 0.70 mM acrylamide through drinking water. (23). Acrylamide exposure lowered the levels of TSH and serum T4 in females rats. Once the 50 mg/kg acrylamide was put into the drinking water, the cell proliferation increased in this rat's higher possibilities of forming the tumors. It, therefore, seems that acrylamide negatively impacts thyroid health and leads to tumordevelopment.(24)
6.2 Neurotoxicity of acrylamide
The European Food Safety Authority (EFSA) summarized experimental data in 2015 and reported that acrylamide can induce adverse neurotoxic effects in humans through occupational skin absorption and peripheral neuropathy.(32)As a well-known neurotoxin, acrylamide affects both the central and peripheral nervous systems, manifesting in general symptoms such as weakness of the skeletal muscles, axon degradation in the peripheral and central nervous systems, distal edema, loss of weight, and ataxia.(17). Acrylamide exerts several harmful effects on the brain and the sciatic nerve through peripheral neuropathy due to oxidative stress and damaging the nerves. Demyelination, axonal degeneration, and myelin structural alterations. Acrylamide may also exhibit neurotoxicity by forming a conjugate with cysteine residues on presynaptic membrane protein. This interference disrupts vesicular and membrane interaction leading to degeneration at nerve terminals through a mechanism of impaired neurotransmitter release. Enhanced malondialdehyde production is associated with an imbalance of redox in the brain and subsequent damage to neuronal cells that cause neurodegeneration. High levels are represented within blood, erythrocytes, and neurofibrillary tangles, thus contributing to the pathology of Alzheimer's disease. (21)
6.2.1. Evidence of neurotoxicity of acrylamide
The level of malondialdehyde was high and glutathione was low in the acrylamide model rat treated with 50 mg/kg body weight in the spinal cord and the brain exhibiting pathological gait. Acrylamide also induced activation and necrosis of glial cells in the sciatic nerve, cerebellum, cerebrum, spinal cord, and hippocampus. (25). Low doses of acrylamide at 0.5 µg/kg body weight per day and high doses of 5 µg/kg body weight per day administered in a pig model for four weeks caused damage to the duodenal ENS neurons. Such modification in the function of ENS may lead to disorders in the gastrointestinal tract. (26)
6.3 Hepatoxicity of acrylamide
The main organ for the metabolism of dietary acrylamide is the liver, which is hence the main target for its toxicity. A fundamental mechanism is oxidative stress, creating ROS that enhance lipid peroxidation and lead to oxidative damage to the liver. Acrylamide upset the oxidation balance by producing free radicals, thus leading to lipid peroxidation. The ROS combine with reactive fatty acids, which leads to the formation of lipid hydroperoxides and then the peroxyl radicals, where MDA is formed that further enhances lipid peroxidation drastically, increasing the oxidative stress in the liver.(35)Exposure to acrylamide resulted in a deficiency of glutathione (GSH) and reduced glutathione-S-transferase (GST) activity in liver tissues, driven by increased reactive oxygen species (ROS) levels, which ultimately damaged hepatic cells.(27). The hepatotoxic effect of acrylamide extends to lipid metabolism, which significantly affects the liver due to oxidative stress. It therefore can influence both the pathological and physiological damage in liver tissues that reveals factors which alter acrylamide's hepatotoxicity.
6.3.1. Evidence of hepatotoxicity of acrylamide
Exposure to the substance in 8–12-week-old female rats fed 500 µg/kg body weight per day of acrylamide via tap water resulted in the decrease of glutathione (GSH) contents and significantly reduced the activity of glutathione-S-transferase (GST) in liver tissues. This decrease was accompanied with the increased ROS content leading to cell damage in the hepatic cells. (28). Indeed, in the male albino rat model that was administrated with 50 mg/day acrylamide for 14 days, hepatic fibrosis and a massive accumulation of collagen fibers were recorded within the liver cells. Apparently, this caused an impairment of hepatic blood flow through increased oxidative stress and decreased glutathione (GSH) levels. (29). In male Wistar rats that received acrylamide with 250 mg/kg/day for 21 days, it was observed that hepatocytes were a ground where large lipid vacuoles had been formed due to mitochondrial swelling and fatty lipid deposition. This led to vacuolization and congested central veins with chromatolysis, which caused hypoxia and ischemia along with lipid accumulation in cells. (30)
Reproductive Toxicity and Prenatal and Postnatal Effects of Acrylamide
Acrylamide affect both male and female.
6.4.1. Effect on male
Acrylamide caused severe damage to male reproduction by affecting organs such as the epididymis and testis. The fertilization anomalies that follow the exposure of these animals to this chemical result in decreased motility and sperm count surmised to result in infertility. Acrylamide caused severe damage to male reproduction by affecting organs such as the epididymis and testis. The fertilization anomalies that follow the exposure of these animals to this chemical result in decreased motility and sperm count surmised to result in infertility. (31)
6.4.2. Effect on female
In females, acrylamide targets the ovary, affecting corpus luteum formation, atresia, and follicular development. Nitric Oxide Synthase (NOS) involvement during follicular oocyte formation, development, and atresia leads to changes in corpus luteum size and primordial follicles, with a percentage increase of the primary follicles observed. (32). The quality of the egg cells or oocytes is very crucial for mature development. Recently, researchers have established that the consumption of acrylamide, a chemical on some foods, devastates the quality of egg cells considerably. The majority of the damaged oocytes cannot initiate meiosis, that is division, as its inner structure essential in cell division, which involves spindle organization, gets ruptured. Damage occurs due to some malfunctions in specific proteins called centrosome proteins that are involved in the maturation of the cell. Furthermore, human oocytes as well as human embryos are highly vulnerable to the damaging action of molecules termed Reactive Oxygen Species or ROS that give rise to cellular damage and thus inhibit growth and development leading up to the prevention of proper maturation of the oocytes. (32). Some very interesting researches have looked into the link between dietary intakes of acrylamide and health outcomes in mothers and fathers. Acrylamide intake through diet was linked to altered blood estradiol levels in the umbilical cord at birth; changes in sex hormones affect pregnancy development. Some of the studies have indicated that acrylamide causes damages to the tissues in the kidneys of pregnant women. The damage leads to inflammation, loss of particular cells in the kidney called tubular cells, and massive cell death. It causes the blood vessels to become congested and affects a part of the kidney known as Bowman's capsule, which is essential for filtering wastes. (33). Acrylamide in food can have highly adverse effects on the development of babies both before and after birth. Intake of acrylamide by pregnant women can harm the baby directly because acrylamide and its major metabolite, glycidamide, can cross the placenta. These chemicals may reach the tissues or organs of the baby during pregnancy thereby disrupting its development. (34) Acrylamide and its metabolite, glycidamide, are water-soluble, allowing them to cross the placenta and cause damage to fetal tissues. After birth, acrylamide may affect infants through mothers' milk. As it decreases levels of prolactin, which is a hormone for poor lactation, infants can become malnourished and lose weight. In addition, consumption of acrylamide-rich foods during pregnancy results in infants being born with low birth weight. The birth dimensions of babies in terms of length and weight are affected by this, according to various studies. (34) During pregnancy, the intake of acrylamide-rich foods can increase oxidative stress with a higher risk of maternal inflammation. Oxidative stress, in turn, can cause prenatal and postnatal neurotoxicity by causing morphological changes in the developing cerebellum, reducing the antioxidative defense system. (32) At both stages of prenatal and postnatal development, oxidative stress is involved in damaging kidney tissues as the kidney's antioxidant defense system is lower than any other organ; hence, there is toxic accumulation in the tubules. Furthermore, elevated oxidative stress can impair bone development, leading to bone loss and altering bone cell differentiation. (32)
|
Food |
Process |
Step Steps that may help reduce acrylamide |
|
Potato-based foods |
Raw materials |
• Selecting potato varieties that are low in acrylamide precursors, keeping in mind seasonal variation. • Optimizing potato maturity by controlling planting time, harvest time, and input management, and by removing immature tubers before processing. • Avoiding handling potatoes with excessive roughness, avoiding bruising potatoes, and sorting out or carefully trimming potatoes with defects. • Avoiding cold temperatures during harvest, transport, delivery, and storage. • Managing storage conditions to control sprouting and provide ventilation. • Monitoring reconditioning results and avoiding reconditioning potatoes stored for prolonged periods. • Assessing reducing sugar levels in incoming potatoes, identifying target levels for incoming potatoes, or using treatments to reduce sugar levels. |
|
French fries |
Processing and ingredients |
• Cutting fries in shapes with lower surface area to volume ratio and screening out small fragments. • Changing blanching practices, although such changes may affect product quality. • Using sugar dips to reduce variability, but using reducing sugars such as fructose in dips may increase acrylamide. • Using alternative coloration methods by discouraging overbaking. • Using sodium acid pyrophosphate (SAPP) and evaluating other dip or batter ingredients to determine if they contribute to acrylamide formation during frying. |
|
Sliced potato chips |
Processing and ingredients |
• Increasing peel removal. • Washing or soaking potato chips before frying, but may cause unacceptable changes to the chips. • Cutting thinner potato chip slices. • Decreasing frying temperatures to 175 °C (347 °F) or below and targeting higher moisture endpoints, but it is important to determine if moisture endpoints provide acceptable product quality. • Using lower temperatures during final cooking stages and using techniques like flash frying, vacuum frying, or batch frying. • Sorting by color, by providing a useful indicator of acrylamide levels, especially if correlated with measured levels of acrylamide in specific products |
|
Fabricated potato chips & snacks |
Processing and ingredients |
• Selecting potato flakes with lower levels of reducing sugars. Lower reducing sugar levels may be found by specifying maximum sugar levels, buying early in the processing season, or by mixing flakes from different sources. Flakes treated with acidulants, calcium, or asparaginase during flake production may also produce flake-based products with lower acrylamide. • Partially substituting potato flakes with other ingredients in fabricated potato products. • Adding calcium salts to potato doughs in fabricated potato products. • Adding acidulants to potato doughs in fabricated potato products. • Adding asparaginase to potato doughs in some fabricated potato products. • Decreasing cooking temperatures, using lower final temperatures in multistage processes, and using higher moisture endpoints in fabricated potato chips. |
|
Potato-based foods (Food service operation) |
Preparation and cooking instructions |
• Providing appropriate cooking instructions on frozen french fry packages to guide final preparation by consumers and food service operators. • Educating food service workers to follow proper frying techniques for french fries. • Selecting potato varieties that are low in reducing sugars for frying or roasting, properly handling and storing potatoes, and using certain cooking practices for foods made from potatoes. |
Reducing Acrylamide in Cereal-based Foods: Fact Sheet by FDA
|
Food |
Process |
Step Steps that may help reduce acrylamide |
|
Cereal-based foods (such as bread, breakfast cereal, crackers, cookies, crispbreads) |
Raw materials Processing and ingredients |
• Using wheat varieties that are lower in asparagine and using wheat grown with adequate soil sulfate and without excessive nitrogen fertilization. • Partially substituting low-asparagine cereal grains for high-asparagine cereal grains in cereal-based foods. |
|
|
Processing and ingredients |
• Replacing ammonium bicarbonate in cookies and crackers with alternative leavening agents, while avoiding overall increases in sodium levels. • Replacing reducing sugars with nonreducing sugars, using reducing sugars with lower fructose content, and only adding sugar coatings to breakfast cereals after toasting steps. • Using asparaginase treatment in cereal-based foods, but dose, contact time, dough water content, pH, and water chlorination are important considerations. • Using calcium supplementation in non-calcium-fortified breads or breakfast cereals, but the addition of calcium propionate may increase acrylamide levels. • Using yeast fermentation and changing fermentation conditions. • Lowering thermal input through modifying baking times and temperatures and considering alternative baking technologies. • Monitoring production by using color as an indicator of acrylamide, but the correlation between color and acrylamide may have to be determined on a product-by-product basis. • Setting a higher moisture endpoint in cereal-based foods, and monitoring moisture levels in finished products may be useful as an indirect indicator of acrylamide levels |
|
Preparation and cooking instructions |
• Baking and toasting breads and other baked goods to a light brown, not a dark brown color; and avoiding overly dry or crusty products in cereal-based foods |
CONCLUSION:
Acrylamide, a byproduct of high-temperature cooking, poses significant health risks including carcinogenicity, neurotoxicity, and reproductive toxicity. Understanding the factors that influence its formation, such as temperature, food composition, and storage conditions, is essential for managing its levels in food. Continued research and adherence to regulatory guidelines are critical to minimizing exposure and protecting public health.
REFERENCES



Krina Patel*, Keval Gondaliya, Ruchita Savaniya, Dr. Hina Bagada, Acrylamide: Analytical Methods, Toxicity and Regulatory Aspect, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 528-543. https://doi.org/10.5281/zenodo.16750294
 10.5281/zenodo.16750294
10.5281/zenodo.16750294
