Gitam Institute of Medical Sciences and Research. Visakhapatnam,
Purpose: The iris and its qualitative, quantitative and dynamic factors are closely responsible for the prevalence and severity of Primary Angle Closure Glaucoma. This is correlative study of the peripheral thickness of the iris measured in two deferent ethnic groups to establish the predisposing and risk factors in the pathogenesis of angle closure glaucoma. Methods: 200 eyes of 100 individuals from two different ethnic groups of Asian and African respectively, between the ages of 18 – 35 years are included in this study. The peripheral thickness 500 microns from root of iris measured with Anterior segment OCT (AS OCT) Topcon camera, in static mode and the parameters are analysed. Results: The average peripheral nasal iris thickness in Asians 324.5 µm (324.5 + - 1.00 ; n=40), p < 0.03 and in the Africans 294.5 µm. (294.5 + -1.00 ;n=40) p < 0.05. The average nasal iris thickness in Asian female is 318 µm and males 322 µm. The average nasal iris thickness in African female is 273 µm and males 299 µm. The Asian and African males had slightly thicker iris than Asian and African females. The average nasal iris thickness of Africans RE, 223 µm and LE: 291 µm. The average nasal iris thickness Asians RE 321 µm and LE: 319 µm. The average iris thickness nasal iris of Right and Left eye in Asians are found to have thicker than Africans. The analysis was done using a independent test analysis The results showed a statistical significance between both the ethnic groups with a p-value of < 0.05. Conclusions: Asian ethnic group have thick peripheral iris compared to African race. This study explains and supports the Asian community is more prone for Angle closure glaucoma as they are having thick peripheral iris. AS OCT is an useful non invasive investigation to use in the screening methods to identify the risk factors such as iris thickness, anterior chamber parameters.
Glaucoma is a group of diseases that lead to progressive optic neuropathy, due to loss of retinal ganglion cells and their axons that lead to atrophy of the optic nerve, which can cause visual field defects and ultimately leads to irreversible blindness. The raised intraocular pressure is the major risk factor.1. The major variants of glaucoma are A. Primary Open Angle glaucoma (POAG), B. Primary Angle Closure Glaucoma (PACG). C .Congenital Glaucoma and D. Secondary Glaucoma. IOP will be raised in all types of Glaucoma except in Normal Tension Glaucoma, a variant of Open angle glaucoma. There is vast geographical variation in the incidence of glaucoma. The Prevalence of open angle glaucoma is more in the western than Eastern part of the World and more in Africans and Hispanics. Asian ethnicity have the highest prevalence of PACG, because they have several risk factors. 2,3. Many factors contributes for the ethnic epidemiological variations of PACG. Asians have several anterior chamber and angle anatomical risk factors which makes them prone to PACG. Though both POAG and PACG are ultimately lead to the permanent blindness if not diagnosed in time and not properly treated. PACG is 3 times have more severe in the aspect of complications and blindness than POAG. 4. PACG is more aggressive form of glaucoma. It is responsible for 90% glaucoma blindness in China. PACG More common in Asian Ethnicity especially in Chinese population. China and India have more number of total number of glaucoma individuals than any other part of the World. 5. Age is the another important risk factor for glaucoma. Asia harbour for about 77% of worldwide PACG cases, as 60% of world’s population lives in the Asia and the number of the centenarians are increasing in Asia since the last 200 years. 6. The incidence of all forms of PACD 16.4 per 100 person-years in rural southern India 9The rural part of southern India have 1.58% of primary angle closure disease (PAC and primary angle-closure glaucoma) 7. It is estimated that by 2050, the global population with PACG will be 26.26 million and 18.47 million are in Asia alone.8.. Nearly 50–90% of individuals with glaucoma worldwide are un diagnosed. ? Tielsch JM, Sommer A, Katz J, Royall RM, Quigley HA, Javitt J. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore eye survey. JAMA. 1991;266:369–74. 9. PACG is an important cause for the irreversible blindness. There are 21 million people with angle-closure glaucoma worldwide. Out of them, 5.3 million Bilateral blind due to PACG. 10.There is a need for to understand and to focus on pathology the underlying mechanisms of PACD, to find out new modalities of screening methods, the treatment and to improve the quality of life the individual. There are many risk factors that contribute to the etiology of PACG. Ethnicity, Family history, Female gender, advanced age, hyperopia, shallow anterior chamber, lens vault thick lens, thick peripheral iris and its configuration, pupil and the stickiness of the iris. Chinese are more prone for angle Closure Glaucoma because they have several risk factors like thicker iris, sticky and greater iris surface area 13.Chinese had smaller angle recess area and trabecular-iris space area than Caucasian 11. Iris and its structure plays an important role in Angle Closure Glaucoma. Iris developed from the anterior part Optic cup at seventh week of intra uterine life. The iris stromal layer developed from the mesoderm. 12, 13.Iris consists, anterior non pigmented middle vascularized and posterior pigmented layers. The iris is supplied with nerves from the parasympathetic and sympathetic nervous systems, which control the pupil's size: Pupil and the peripheral iris also plays a role in the pathogenesis of Angle closure Glaucoma. The “Relative pupillary block theory mechanism for Angle closure glaucoma was first described by Curren, the father of Angle Closure Glaucoma. He proposed the “Pupillary Block Glaucoma Theory” in 1920 itself. 14. Though there are multiple non pupillary mechanisms also paly a role in the pathogenesis of PACG. They are cornea, Iris, Lens, Ciliary body, Anterior Chamber angle, Zonules, Choroid, Vitreous. The Iris has it’s specific role in etiopathogenesis of angle closure glaucoma. The anatomic factors responsible for Angle closure attack include the iris thickness in the resting state and the insertion of iris into ciliary body. The spongy nature of iris tissue which is first described by the Gregersen in 1958.15. Quigley says “ Iris resembles sponge, with abundant amount of water content , it looses most of its water content when it dilates, becomes thin more at the periphery of the anterior chamber. This thin iris at the periphery, is necessary to keep the AC angle open and to prevent the blockage by the iris tissue. 16. There is considerable amount of fluid exchange between iris and aqueous humor.17. Iris surface and topography plays a role in pathogenesis of PACD. The visible furrows and crypts allows the large molecules and even macroscopic particles to diffuse easily through the iris irrespective of aqueous quality. This is as a part of Uveoscleral outflow, which is an alternative to conventional aqueous out flow pathway. The aqueous passes through iris in to trabecular meshwork even when there is appositional angle closure of the anterior chamber angle. This explains the maintenance of normal IOP in Appositional angel closure. There is sufficient fluid movement through iris to balance the inflow of aqueous. Iris becomes bulky and water logged when pupil is miosed and on dilatation it looses water and becomes thin. In Acute Angle Closure, there are both qualitative and quantitative changes in the iris and the fluid passage ratio through the iris is affected. Iris becomes water logged and bulky. When this character of iris fails to loose water proportionately, iris bulkiness persists at the periphery it predisposes iridotrabecular contact, a potential dynamic risk factors in onset of the Acute Angle closure attack. The compactness of the eye with it’s iris with more water retention in the stroma leads to iris bulkiness which makes the eye more susceptible for AACG. 18.The iris vasculature plays a role in the Acute Angle Closure Glaucoma. Iris volume consists 10% of vascular component. There is a proportionate balance between vascular congestion, size of the pupil and iris volume. During vascular congestion, iris thickness increased and there is a possibility of iridotrabecular contact. 19. The thickness of the iris increase with the age . The thickness of iris is more in females, a risk factor for angle closure glaucoma. 20. This is due to increased arterial adventitia in the iris vessels at the root of the iris and amount of melanin granules increased near the pupillary border and iris root.21 .22. The biomechanical properties like the iris stiffness more in PACD than normal iris.23. 24. These altered biomechanics are due to presence of excess collagen in iris stroma in identified in PACG . 25. This increased stiffness of iris in turn leads to poor exchange of water in the iris from the aqueous, causes more iris volume and increases the thickness of iris. PACG eyes have a low permeability to water. Absorption of water and exudates reduced during smooth muscle contraction in PACG. Inability of Iris stroma to loose interstitial fluid on dilatation is the main contributing factor for angle closure.26. This was demonstrated by Aptel in his iris cross sectional studies.27. The thickness of the iris can also be assessed with the number of furrows present on the anterior surface of the iris. The iris with less number of crypts have less porous in nature and would therefore allow less Aqueous permeability through iris. The number of furrows are inversely proportional to the iris thickness. 28.The thick iris eyes are more prone for PACG. 29 The thickness of iris varies from sex, iris colour, and ethnicity. Brown eyes have a tendency of thick iris stroma leads to less water exchange and little alteration in volume with dilation. 30. Many studies shown that the anterior chamber has comparatively narrow angles nasally than temporal. 31. The thickness of the iris can be assess by ASOCT.32. The iris thickness can be measured either with Anterior Segment Optical Coherence Tomography (ASOCT) or Ultrasound Biomicroscopy (UBM). 33 ASOCT produce high-resolution cross-sectional images and The two dimensional cross sectional image of the iris can be obtained by the standard static mode by ASOCT.34
MATERIAL AND METHODS:
Volunteers Asians and Africans students selected from paramedical courses Gitam University, Visakhapatnam campus. In this analytical comparative study, 400 eyes (100 Asians and 100 Africans), between the age of 18 to 35 years are selected for this study. Out of 100 subjects 50 are males and 50 are females from Asian ethnicity and African ethnicity respectively. A comprehensive ophthalmic examination is carried out, includes Best Corrected visual acuity (BCVA) obtained after refractive correction, Anterior segment is evaluated by Slit lamp biomicroscopic examination, Fundus examination is carried out by + 78Ds lens, Intra Ocular Pressure (IOP) recorded with Applanation tonometer. The cases with defective vision, IOP more than 21 mm of Hg, those who underwent LASIK, other Anterior segment diseases are excluded from this study. This study is conducted in the Department of Ophthalmology with the approval of Ethics committee of Gitam Institute of Medical Sciences and Research, Visakhapatnam. All the cases are subjected to measurement of root of iris by the Optical coherent tomograph Topcon 3D OCT-1 Maestro 2 in static mode, 500 microns from the root of the iris. Nasal aspects of the root of the iris thickness of the Africans (Fig 1) and Asians are measured (Fig 2).
RESULTS:
In this study we find the average nasal iris thickness of Asians is 324.5 µm (324.5 + - 1.00 ; n=40), p < 0.03 and in the Africans 294.5 µm. (294.5 + -1.00 ;n=40) p < 0.05. The average nasal iris thickness in Asian female is 318 µm and males 322 µm. The average nasal iris thickness in African female is 273 µm and males 299 µm. p < 0.05 The Asian and African males had slightly thicker iris than Asian females. The average nasal iris thickness of Africans RE is 223 µm and LE is 291 µm. The average nasal iris thickness Asians RE is 321 µm and LE is 319 µm. The nasal iris thicknesses of Right and Left eye in Asians are found to be thicker than Africans. The results showed a statistical significance between both the ethnic groups with a p-value of < 0.05, for both eyes respectively. Independent “t” test analysis comparing the mean nasal iris thickness between Asian and African group shows p value < 0.05 indicating statistically significant difference between the two groups. Females shows slightly higher nasal iris thickness in both ethnic groups (Fig. 5). Our study revealed Asians had greater iris thickness than Africans.
DISCUSSION:
The angle closure attack involves multiple mechanisms including pupillary bock and iridotrabcular contact. Understanding of pathogenesis is important to help for early diagnosis and to plan the treatment strategies. The pattern and thickness of iris is the key factor in the prediction of primary angle closure disease. The thickness of the root of the iris, surface convexity, the pupil area of the iris, iris volume, the number of iris crypts, insertion of iris and the micro structure of the iris are the important landmarks and plays an important role in the pathogenesis of Angle Closure Glaucoma and also in the Acute Angle Closure Glaucoma.35. The iris root thickness is more in Angle closure individuals than normal ones. The Iris thickness is more in the Asians especially in Chinese, which is a risk factor for PACD. Many studies shown the incidence of PACD is more in Chinese ethnicity because of the thick peripheral iris. The iris thickness increase with the age. Advanced age is another risk factor for PACD. As the age advances, several parameters of the anterior segment altered, that contribute to the Angle closure Glaucoma. Iris convexity is another important parameter in the pathogenesis of PACD. In our study we find the nasal iris thickness in Asians is 324.5 µm and in Africans 289.6 µm. This explains the Asian Ethnicity more prone for Angle closure glaucoma than African ethnicity. Males are found to have thick iris than females, as revealed in the other study. In a study conducted by Qingchen by who measured the the mean iris thicknesses in Chinese population the temporal and nasal sides were 364.79 ± 47.58 μm and 372.44 ± 43.75 μm, respectively. 36. The thickness of iris found to be much higher in chinese population than Asians and Africans. The limitations of our study less number of sample is less and the participants are younger age individuals, who are not in the risk group of PACD. In vivo Studies are necessary to read the iris structural and functional qualities, which are prone for Angle closure glaucoma. So these investigative procedures may helpful in the screening methods of Angle Closure Glaucoma. Our study compared with that the Similar study Iris Thickness was thicker in males when compared to females. The Guangzhou Twin Eye Study also revealed the same results 37.
CONCLUSION:
Asian ethnic group have thick peripheral iris compared to African race and Asian iris are found to be thicker than Africana. AS OCT is an useful non invasive investigation to use in the screening methods to identify the risk factors such as iris thickness, anterior chamber parameters.
REFERENCES
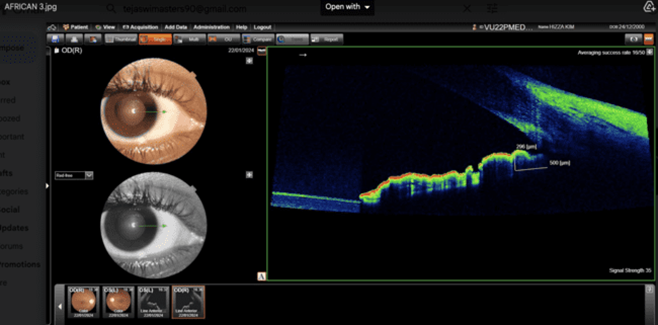
Fig 1: Iris thickness of African at T500 with 296 microns

Fig 2: Fig: Iris thickness of Asian at T500 with 325 microns
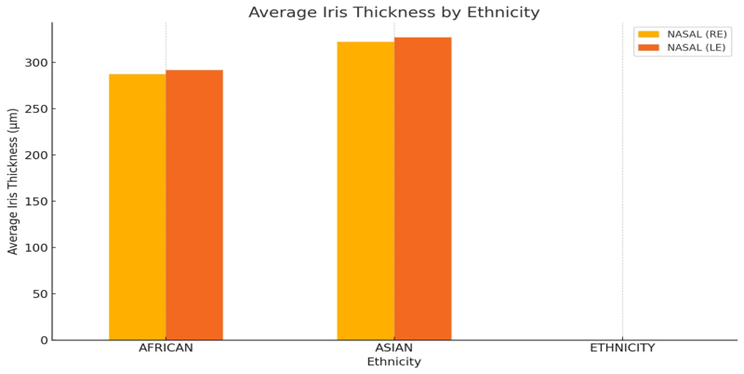
Fig 3: The bar graph represents the nasal iris thickness between the African and Asian ethnicities.
Asian ethnicity has significantly thicker irises on average than African ethnicity in this dataset.

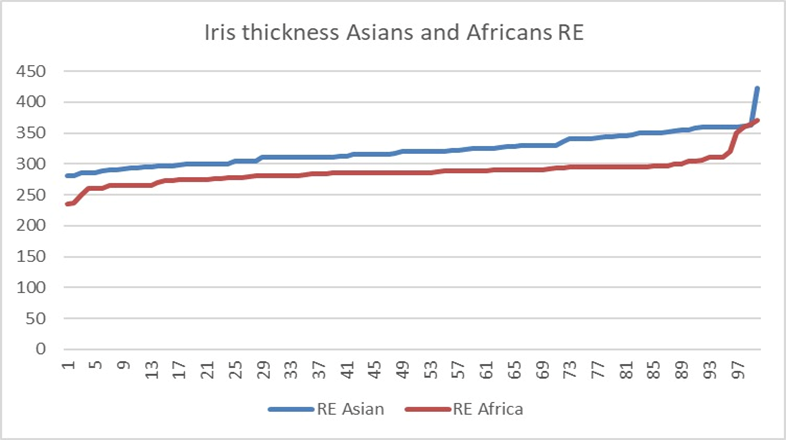
Fig 4: The line diagram shows the Asian ethnicity has higher average iris thickness in both right and left eyes compared to African ethnicity.

Fig 5: The box plot represents that the Females have higher average iris thickness in compared to Males of both ethnicities, respectively.
Table 1: Master list showing the data of Ethnicity, Male female, Age and iris thickness at nasal quadrant.
Iris Thickness – Nasally At 500 µ Between Asians and African Population
|
S. No. |
Age |
Ethnicity |
Nasal (RE) |
Nasal (LE) |
Age |
Ethnicity |
Nasal (RE) |
Nasal (LE) |
|
1. |
19/F |
Asian |
320 µ |
325 µ |
21/M |
African |
280 µ |
255 µ |
|
2. |
20/F |
Asian |
300 µ |
290 µ |
23/F |
African |
285 µ |
280 µ |
|
3. |
20/M |
Asian |
350 µ |
360 µ |
25/F |
African |
295 µ |
300 µ |
|
4. |
20/M |
Asian |
300 µ |
315 µ |
18/M |
African |
236 µ |
255 µ |
|
5. |
20/F |
Asian |
285 µ |
295 µ |
22/F |
African |
275 µ |
280 µ |
|
6. |
20/F |
Asian |
320 µ |
340 µ |
21/M |
African |
250 µ |
280 µ |
|
7. |
20/M |
Asian |
310 µ |
325 µ |
22/M |
African |
286 µ |
300 µ |
|
8. |
19/F |
Asian |
300 µ |
290 µ |
20/F |
African |
280 µ |
290 µ |
|
9. |
22/M |
Asian |
325 µ |
330 µ |
22/M |
African |
286 µ |
290 µ |
|
10. |
24/F |
Asian |
290 µ |
325 µ |
20/M |
African |
300 µ |
310 µ |
|
11. |
33/M |
Asian |
305 µ |
281 µ |
31/M |
African |
306 µ |
300 µ |
|
12. |
19/F |
Asian |
285 µ |
290 µ |
21/F |
African |
365 µ |
350 µ |
|
13. |
20/F |
Asian |
305 µ |
320 µ |
23/M |
African |
290 µ |
300 µ |
|
14. |
22/F |
Asian |
310 µ |
320 µ |
23/M |
African |
360 µ |
365 µ |
|
15. |
20/M |
Asian |
320µ |
380µ |
23/M |
African |
280 µ |
290 µ |
|
16. |
19/F |
Asian |
325 µ |
310 µ |
23/M |
African |
370 µ |
375 µ |
|
17. |
19/M |
Asian |
311 µ |
330 µ |
20/F |
African |
310 µ |
305 µ |
|
18. |
19/F |
Asian |
325 µ |
340 µ |
24/F |
African |
290 µ |
280 µ |
|
19. |
21/M |
Asian |
423 µ |
430 µ |
18/F |
African |
280 µ |
300 µ |
|
20. |
21/M |
Asian |
327 µ |
315 µ |
22/F |
African |
350 µ |
354 µ |
|
21. |
35/M |
Asian |
300 µ |
310 µ |
30/M |
African |
285 µ |
290 µ |
|
22. |
24/F |
Asian |
363 µ |
359 µ |
23/F |
African |
235 µ |
250 µ |
|
23. |
22/M |
Asian |
360 µ |
350 µ |
25/F |
African |
260 µ |
270 µ |
|
24. |
20/F |
Asian |
316 µ |
300 µ |
22/M |
African |
300 µ |
310 µ |
|
25. |
19/M |
Asian |
350 µ |
300 µ |
31/F |
African |
295 µ |
320 µ |
|
26. |
22/F |
Asian |
310 µ |
360 µ |
26/M |
African |
260 µ |
285 µ |
|
27. |
20/F |
Asian |
330 µ |
340 µ |
32/M |
African |
310 µ |
290 µ |
|
28. |
22/M |
Asian |
320 µ |
350 µ |
28/F |
African |
320 µ |
300 µ |
|
29. |
20/F |
Asian |
320 µ |
335 µ |
22/M |
African |
280 µ |
290 µ |
|
30. |
21/M |
Asian |
360 µ |
350 µ |
23/M |
African |
285 µ |
305 µ |
|
31. |
24/F |
Asian |
330 µ |
340 µ |
31/M |
African |
310 µ |
300 µ |
|
32. |
23/M |
Asian |
296 µ |
330 µ |
24/F |
African |
290 µ |
295 µ |
|
33. |
26/F |
Asian |
360 µ |
375 µ |
23/M |
African |
260 µ |
275 µ |
|
34. |
25/M |
Asian |
320 µ |
330 µ |
22/F |
African |
270 µ |
280 µ |
|
35. |
20/F |
Asian |
350 µ |
335 µ |
21/F |
African |
265 µ |
275 µ |
|
36. |
24/M |
Asian |
295 µ |
310 µ |
20/F |
African |
280 µ |
300 µ |
|
37. |
27/M |
Asian |
340 µ |
350 µ |
26/F |
African |
290 µ |
290 µ |
|
38. |
30/F |
Asian |
330 µ |
325 µ |
26/F |
African |
286 µ |
296 µ |
|
39. |
31/M |
Asian |
280 µ |
290 µ |
21/F |
African |
305 µ |
315 µ |
|
40. |
29/M |
Asian |
345 µ |
360 µ |
25/M |
African |
297 µ |
310 µ |
|
41 |
21/M |
Asian |
330 µ |
328 µ |
31/M |
African |
285 µ |
290 µ |
|
42 |
26/M |
Asian |
305 µ |
310 µ |
22/F |
African |
275 µ |
280 µ |
|
43 |
21/M |
Asian |
323 µ |
340 µ |
23/F |
African |
265 µ |
282 µ |
|
44 |
26/F |
Asian |
360 µ |
350 µ |
22/F |
African |
275 µ |
285 µ |
|
45 |
28/M |
Asian |
317 µ |
325 µ |
19/M |
African |
283 µ |
290 µ |
|
46 |
27/F |
Asian |
340 µ |
345 µ |
19/M |
African |
290 µ |
300 µ |
|
47 |
32/M |
Asian |
310 µ |
320 µ |
20/F |
African |
295 µ |
284 µ |
|
48 |
31/M |
Asian |
360 µ |
348 µ |
25/F |
African |
265 µ |
283 µ |
|
49 |
24/F |
Asian |
328 µ |
320 µ |
30/M |
African |
295 µ |
290 µ |
|
50 |
30/M |
Asian |
329 µ |
326 µ |
32/M |
African |
273 µ |
279 µ |
|
51 |
27/M |
Asian |
355 µ |
360 µ |
26/F |
African |
285 µ |
288 µ |
|
52 |
25/F |
Asian |
336 µ |
332 µ |
25/M |
African |
295 µ |
276 µ |
|
53 |
24/M |
Asian |
328 µ |
339 µ |
22/F |
African |
286 µ |
289 µ |
|
54 |
28/F |
Asian |
360 µ |
355 µ |
21/M |
African |
295 µ |
275 µ |
|
55 |
30/F |
Asian |
352 µ |
340 µ |
22/M |
African |
279 µ |
283 µ |
|
56 |
31/M |
Asian |
358 µ |
350 µ |
28/F |
African |
276 µ |
285 µ |
|
57 |
24/F |
Asian |
285 µ |
295 µ |
30/F |
African |
292 µ |
295 µ |
|
58 |
26/M |
Asian |
290 µ |
300 µ |
22/M |
African |
286 µ |
275 µ |
|
59 |
27/M |
Asian |
340 µ |
330 µ |
23/M |
African |
285 µ |
280 µ |
|
60 |
19/F |
Asian |
312 µ |
326 µ |
21/F |
African |
289 µ |
295 µ |
|
61 |
20/F |
Asian |
320 µ |
334 µ |
27/M |
African |
275 µ |
285 µ |
|
62 |
22/M |
Asian |
311 µ |
322 µ |
28/F |
African |
265 µ |
286 µ |
|
63 |
22/F |
Asian |
296 µ |
300 µ |
31/F |
African |
297 µ |
305 µ |
|
64 |
28/F |
Asian |
353 µ |
363 µ |
25/M |
African |
289 µ |
295 µ |
|
65 |
30/M |
Asian |
340 µ |
355 µ |
19/M |
African |
288 µ |
286 µ |
|
66 |
31/F |
Asian |
316 µ |
328 µ |
21/F |
African |
285 µ |
290 µ |
|
67 |
25/F |
Asian |
344 µ |
350 µ |
24/F |
African |
296 µ |
285 µ |
|
68 |
21/F |
Asian |
316 µ |
310 µ |
22/F |
African |
284 µ |
295 µ |
|
69 |
28/M |
Asian |
329 µ |
330 µ |
26/M |
African |
290 µ |
306 µ |
|
70 |
27/M |
Asian |
310 µ |
320 µ |
26/F |
African |
288 µ |
285 µ |
|
71 |
19/F |
Asian |
347 µ |
330 µ |
29/M |
African |
289 µ |
290 µ |
|
72 |
21/F |
Asian |
311 µ |
317 µ |
31/F |
African |
284 µ |
289 µ |
|
73 |
29/M |
Asian |
361 µ |
350 µ |
33/F |
African |
285 µ |
290 µ |
|
74 |
28/M |
Asian |
342 µ |
348 µ |
34/M |
African |
295 µ |
293 µ |
|
75 |
27/F |
Asian |
316 µ |
320 µ |
26/F |
African |
288 µ |
287 µ |
|
76 |
28/M |
Asian |
355 µ |
342 µ |
22/M |
African |
295 µ |
285 µ |
|
77 |
22/F |
Asian |
316 µ |
318 µ |
19/M |
African |
295 µ |
302 µ |
|
78 |
22/M |
Asian |
322 µ |
305 µ |
20/F |
African |
265 µ |
285 µ |
|
79 |
21/M |
Asian |
296 µ |
299 µ |
21/F |
African |
273 µ |
289 µ |
|
80 |
24/F |
Asian |
344 µ |
330 µ |
21/F |
African |
286 µ |
295 µ |
|
81 |
25/M |
Asian |
350 µ |
325 µ |
22/M |
African |
265 µ |
275 µ |
|
82 |
33/F |
Asian |
294 µ |
290 µ |
25/F |
African |
278 µ |
295 µ |
|
83 |
31/M |
Asian |
310 µ |
315 µ |
26/M |
African |
287 µ |
295 µ |
|
84 |
29/M |
Asian |
300 µ |
320 µ |
27/M |
African |
295 µ |
293 µ |
|
85 |
28/F |
Asian |
315 µ |
310 µ |
30/M |
African |
276 µ |
285 µ |
|
86 |
24/M |
Asian |
295 µ |
312 µ |
32/M |
African |
280 µ |
295 µ |
|
87 |
23/F |
Asian |
305 µ |
326 µ |
31/F |
African |
290 µ |
285 µ |
|
88 |
26/F |
Asian |
312 µ |
330 µ |
23/F |
African |
293 µ |
289 µ |
|
89 |
25/M |
Asian |
300 µ |
290 µ |
25/M |
African |
278 µ |
295 µ |
|
90 |
20/F |
Asian |
298 µ |
315 µ |
22/F |
African |
284 µ |
281 µ |
|
91 |
24/F |
Asian |
321 µ |
336 µ |
23/M |
African |
275 µ |
285 µ |
|
92 |
27/M |
Asian |
310 µ |
316 µ |
21/F |
African |
295 µ |
290 µ |
|
93 |
30/M |
Asian |
292 µ |
298 µ |
25/M |
African |
286 µ |
295 µ |
|
94 |
31/F |
Asian |
310 µ |
320 µ |
30/M |
African |
305 µ |
285 µ |
|
95 |
23/F |
Asian |
299 µ |
302 µ |
32/F |
African |
290 µ |
285 µ |
|
96 |
25/M |
Asian |
289 µ |
296 µ |
33/M |
African |
278 µ |
275 µ |
|
97 |
27/F |
Asian |
345 µ |
332 µ |
25/F |
African |
265 µ |
282 µ |
|
98 |
26/F |
Asian |
325 µ |
329 µ |
22/M |
African |
293 µ |
295 µ |
|
99 |
31/M |
Asian |
280 µ |
295 µ |
22/F |
African |
288 µ |
292 µ |
|
100 |
29/F |
Asian |
293 µ |
315 µ |
24/M |
African |
295 µ |
286 µ |



Dr. KVV Satyanarayana*, Dr. Vidhya Kuppili, CH. Tejaswi, Dr. K. Ravi Naini, Satya Varaprasad, Dr. VVL Narasimha Rao, A Clinical Study on Iris Thickness in Asians and Africans, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 8, 1928-1938 https://doi.org/10.5281/zenodo.16900334
 10.5281/zenodo.16900334
10.5281/zenodo.16900334
