Dr. Vedprakash Patil Pharmacy College Aurangabad
Casearia graveolens, a medicinal plant traditionally used to treat various ailments, including liver-related disorders, has shown promising hepatoprotective potential. This comprehensive review aims to summarize the current state of knowledge on the hepatoprotective effects of Casearia graveolens, focusing on its phytochemical profile, pharmacological activities, and potential therapeutic applications. The plant's rich composition of bioactive compounds, including clerodane-type diterpenoids, flavonoids, and coumarins, provides a promising foundation for its hepatoprotective effects. While preliminary studies suggest its potential benefits, further research is needed to fully elucidate its mechanisms of action, efficacy, and safety. This review highlights the need for systematic investigation into the hepatoprotective properties of Casearia graveolens, which could pave the way for developing safe and effective plant-based therapeutic candidates for managing hepatic disorders.
Anatomy and Physiology of the Liver
The liver is the largest glandular organ in the human body and performs over 500 critical physiological functions essential for maintaining homeostasis. In adults, it typically weighs between 1.2 and 1.5 kilograms and resides in the right upper quadrant of the abdominal cavity, situated just beneath the diaphragm and partially protected by the rib cage. It is suspended from the diaphragm by the falciform ligament, which anatomically divides the liver into right and left lobes. Functionally, the liver is subdivided into lobes and further segmented based on Couinaud’s classification, which defines eight distinct segments, each independently supplied by a branch of the portal vein, hepatic artery, and bile duct. This segmental architecture is crucial in hepatic surgery and liver transplantation, as it enables selective resection or grafting with preserved vascular and biliary integrity. (Bruha et al., 2012; Seitz et al., 2018)
A unique feature of the liver is its dual blood supply. Approximately 75% of the liver’s blood flow is derived from the portal vein, which delivers nutrient-rich but oxygen-poor blood from the gastrointestinal tract, pancreas, and spleen. The remaining 25% is supplied by the hepatic artery, which provides oxygenated blood from the systemic circulation. These two blood sources mix within the hepatic sinusoids—low-pressure, fenestrated capillary networks lined by specialized endothelial cells that facilitate efficient exchange of solutes between blood and hepatocytes. At the microscopic level, the liver is composed of hepatic lobules, which are hexagonal structural units centered around a central vein. At each corner of the lobule lies a portal triad, consisting of branches of the portal vein, hepatic artery, and bile duct. Hepatocytes, the principal parenchymal cells of the liver, are arranged in radial plates extending from the central vein and are in direct contact with sinusoidal blood. This anatomical arrangement enables rapid uptake and processing of nutrients, hormones, toxins, and xenobiotics. (Gougol et al., 2021; Singal et al., 2024; Suriawinata and Thung, 2006)In addition to hepatocytes, the liver houses several non-parenchymal cells with distinct functions:
Sinusoidal endothelial cells regulate vascular permeability and mediate immune cell trafficking, contributing to hepatic immune homeostasis
Key Metabolic, Detoxification, and Synthetic Roles of the Liver
The liver plays a central role in maintaining systemic metabolic equilibrium and is essential for numerous physiological processes involving the metabolism of carbohydrates, lipids, and proteins, aswell as the detoxification of harmful substances and the biosynthesis of critical biomolecules. In carbohydrate metabolism, the liver regulates blood glucose levels through three primary mechanisms: glycogenesis, glycogenolysis, and gluconeogenesis. Lipid metabolism is another crucial hepatic function. The liver is the primary site for both the synthesis and degradation of fatty acids and cholesterol. It produces very low-density lipoproteins (VLDL) to transport triglycerides to peripheral tissues and facilitates the oxidation of fatty acids through β-oxidation to generate ATP. Detoxification is among the liver’s most vital roles. It acts as the principal site for the biotransformation of xenobiotics, environmental toxins, drugs, and metabolic waste products. Detoxification occurs in two phases. Phase I reactions, primarily mediated by cytochrome P450 enzymes, involve oxidation, reduction, or hydrolysis to introduce reactive groups. Phase II reactions involve conjugation processes such as glucuronidation, sulfation, and acetylation, which increase the water solubility of metabolites, facilitating their excretion via urine or bile. In carbohydrate metabolism, the liver regulates blood glucose levels through three primary mechanisms: glycogenesis, glycogenolysis, and gluconeogenesis. During the postprandial state, the liver converts excess glucose into glycogen for storage, preventing hyperglycemia. In contrast, during fasting conditions, it breaks down stored glycogen into glucose and also synthesizes glucose from non-carbohydrate sources such as lactate, glycerol, and glucogenic amino acids, ensuring a continuous supply of energy. Lipid metabolism is another crucial hepatic function. The liver is the primary site for both the synthesis and degradation of fatty acids and cholesterol. It produces very low-density lipoproteins (VLDL) to transport triglycerides to peripheral tissues and facilitates the oxidation of fatty acids through β-oxidation to generate ATP. Additionally, during prolonged fasting or starvation, the liver produces ketone bodies as an alternative energy source. In terms of protein metabolism, the liver is responsible for the deamination of amino acids, a process that generates ammonia, a toxic byproduct. This ammonia is promptly converted to urea via the urea cycle and excreted by the kidneys. The liver also synthesizes most of the body’s plasma proteins, including albumin, which maintains plasma oncotic pressure; clotting factors such as fibrinogen, prothrombin, and Factors V, VII, IX, and X; transport proteins like transferrin and ceruloplasmin; and various binding globulins involved in hormone and mineral transport. A reduction in the levels of these proteins, particularly clotting factors, is a hallmark of impaired liver function and is commonly observed in advanced liver disease. (Sumadewi, 2023)
Micronutrient Storage and Metal Metabolism:
The liver plays a critical role in regulating iron and copper metabolism, essential for systemic micronutrient balance. It synthesizes hepcidin, a key regulatory hormone that controls intestinal iron absorption and systemic iron distribution. In addition to regulating trace minerals, the liver also serves as a storage site for fat-soluble vitamins A, D, E, and K, as well as iron and copper, further underscoring its role in maintaining nutritional homeostasis. Another vital exocrine function of the liver is bile production, which is essential for digestion and the elimination of metabolic waste. Hepatocytes continuously synthesize and secrete bile, a complex fluid composed primarily of bile acids (cholic and chenodeoxycholic acids), phospholipids (mainly lecithin), cholesterol, bilirubin, excreted into bile. Any disruption in this process can lead to jaundice or cholestasis, signaling impaired hepatic function. In addition to bilirubin, bile facilitates the elimination of excess cholesterol, heavy metals, xenobiotics, and lipophilic drugs, many of which are not effectively cleared by the kidneys. Thus, bile secretion represents a critical detoxification pathway within hepatic physiology. Pathological impairments in bile formation or flow are central to the development of several cholestatic liver diseases, including primary biliary cholangitis, biliary cirrhosis, and obstructive cholestasis. These conditions are marked by reduced bile secretion, toxic bile acid accumulation, and progressive inflammation and fibrosis within the liver. Consequently, disturbances in bile homeostasis not only compromise digestive function but also contribute to hepatocellular damage, highlighting the essential role of bile physiology in both health and disease.(Bacon et al., 1984; Luza et al., 1996)
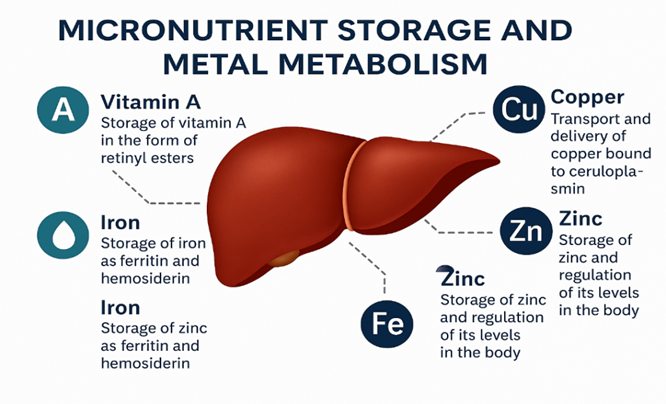
Figure 1: Micronutrient storage and metal metabolism
Global and Indian Epidemiology of Liver Diseases
Global Burden of Liver Disease
Liver diseases constitute a major and escalating global health concern, responsible for approximately two million deaths each year—accounting for nearly 4% of all global mortality, or one in every 25 deaths worldwide. A significant portion of these deaths is linked to chronic liver conditions, particularly cirrhosis and hepatocellular carcinoma (HCC), the most common form of primary liver cancer. Although acute liver failure—often caused by acute viral hepatitis—represents a smaller share of liver-related mortality, its clinical significance remains considerable. Notably, there is a marked gender disparity, with nearly two-thirds of liver disease-related deaths occurring in males, highlighting the disproportionate burden of liver disease in men. (Jain et al., 2024; Sakamoto et al., 2017; Wong et al., 2019) The etiology of chronic liver disease is multifactorial and varies geographically, with the leading global causes including chronic viral hepatitis (HBV and HCV), alcohol-related liver disease (ALD), and non-alcoholic fatty liver disease (NAFLD), recently redefined as metabolic dysfunction-associated fatty liver disease (MAFLD). Among these, hepatitis B virus (HBV) and hepatitis C virus (HCV) have historically been the most significant contributors to cirrhosis and hepatocellular carcinoma, affecting over 250 million and several tens of millions of individuals worldwide, respectively. Together, HBV and HCV infections account for a considerable proportion of global liver-related mortality. (Malviya and Verma, 2023; Mondal et al., 2022; Sumadewi, 2023) Although vaccination initiatives and antiviral therapies have reduced the prevalence of viral hepatitis in many high-income regions, HBV and HCV remain pressing public health concerns in Asia and Sub-Saharan Africa. In these areas, limited access to early diagnosis and treatment significantly hinders disease control efforts. Alcohol consumption represents another major driver of liver disease. Alcoholic liver disease (ALD) encompasses a spectrum of hepatic injury, ranging from simple steatosis to alcoholic hepatitis, progressive fibrosis, and cirrhosis In recent years, non-alcoholic fatty liver disease (NAFLD) has emerged as the most prevalent chronic liver disorder worldwide, driven largely by the escalating global prevalence of obesity, physical inactivity, and type 2 diabetes mellitus. Current estimates suggest that NAFLD affects approximately 25% of the adult population globally—representing over one billion individuals with metabolic-associated hepatic steatosis
The global distribution of liver disease burden reflects the regional dominance of various etiologies. For instance, East Asia and Sub-Saharan Africa continue to bear a disproportionately high burden of HBV-associated cirrhosis and hepatocellular carcinoma (HCC), attributable to historical endemic transmission and gaps in early childhood immunization coverage. On the other hand, countries in Eastern Europe and segments of the Americas exhibit a high prevalence of alcohol-related liver disease (ALD), which is often correlated with socioeconomic and behavioral determinants. Concurrently, NAFLD is becoming a universal public health issue, transcending traditional boundaries between developed and developing nations. In low- and middle-income countries, rapid urbanization and shifting dietary habits towards energy-dense, Westernized food—coupled with a rise in sedentary behavior—are accelerating the incidence of NAFLD, even in regions where viral hepatitis had previously been the primary driver of liver pathology. (Butt et al., 2015; Jindal et al., 2022; Wong and Gish, n.d.; Zhang et al., 2022) This multifaceted interaction of infectious, metabolic, and lifestyle-related risk factors underscores the likelihood of an increasing global burden of liver disease. Without timely and comprehensive interventions, the morbidity and mortality associated with chronic liver diseases are expected to rise further. A multipronged approach is critical to reversing these trends, including: widespread implementation of HBV vaccination; routine screening and early diagnosis of liver disease; policy-driven measures to limit harmful alcohol consumption; large-scale lifestyle modification initiatives targeting diet and physical activity; and improved access to effective antiviral therapies and metabolic disease management
Liver Disease Burden in India
India carries a considerable share of the global liver disease burden, driven by its large and diverse population, coupled with the presence of both infectious and metabolic risk factors. Liver diseases are now recognized among the top ten leading causes of death in the country, reflecting a growing public health concern. According to recent epidemiological estimates, approximately 250,000 deaths per year in India are attributed to liver-related disorders. Among these, cirrhosis accounts for a major portion, with the country's age-standardized death rate for cirrhosis surpassing the global mean. This highlights the urgent need for targeted interventions in screening, prevention, and management of liver diseases within the Indian healthcare framework. (Bhaumik et al., 2015; Mondal et al., 2022; Sumadewi, 2023)
In contrast, rural and socioeconomically disadvantaged areas of the country face unique challenges in liver disease management. The burden is compounded by delayed or missed diagnoses due to lack of awareness and inadequate access to diagnostic services. Specialist hepatology care is often unavailable in these regions, and the health infrastructure is frequently ill-equipped to handle the complexity of chronic liver disease. Together, these urban and rural dynamics underscore the need for a comprehensive national strategy encompassing early detection, public awareness, integration of metabolic health management, and stricter regulation of hepatotoxic exposures to curb the growing impact of NAFLD and other chronic liver diseases in India. (Allen et al., 2016; Sakamoto et al., 2017; Smith et al., 2021; Sumadewi, 2023)
Public Health Implications and Strategic Response
The increasing liver disease burden in India necessitates an integrated and proactive public health approach focused on both prevention and early intervention. Key components of such a strategy include:
Improving disease surveillance and registry data, enabling policymakers to monitor incidence, prevalence, and outcomes more accurately across regions
Pathophysiology of Liver Injury
Mechanisms of Hepatic Injury
Liver injury, whether acute or chronic, can be initiated by a diverse range of etiological factors, including alcohol consumption, viral infections, drug-induced hepatotoxicity, chemical exposure, metabolic dysfunction, and autoimmune disorders. Despite this diversity, these insults converge on several shared pathophysiological mechanisms, including oxidative stress, mitochondrial dysfunction, cytokine dysregulation, and the activation of regulated cell death pathways notably apoptosis, necroptosis, and pyroptosis. These events collectively result in hepatocyte injury, immune system activation, and extracellular matrix remodeling, ultimately driving the progression toward fibrosis, cirrhosis, and in some cases, hepatocellular carcinoma (HCC). Understanding these mechanistic underpinnings is essential for identifying novel therapeutic targets, particularly for the development and scientific validation of hepatoprotective agents derived from medicinal plants, and for designing interventions aimed at halting or reversing liver damage at various stages. (Chen et al., 2024)
Oxidative Stress
Oxidative stress is a key early event in liver injury, arising from an imbalance between the production of reactive oxygen species (ROS) and the liver’s antioxidant defenses. Under physiological conditions, ROS such as superoxide anion (O??), hydroxyl radical (•OH), and hydrogen peroxide (H?O?) are generated at low levels during mitochondrial respiration, xenobiotic metabolism, and immune responses. Enzymes like superoxide dismutase (SOD), glutathione peroxidase (GPx), catalase (CAT), along with non-enzymatic antioxidants such as glutathione (GSH) and vitamin E, normally neutralize ROS.(Pinzani, 2015)
Plant Profile
Taxonomy

Figure 2: Casearia graveolens Dalz
Common Name: Eng : Chilla; Hindi : Safed-karai, Chilla, Phempri; Kannada: Haniche, Konje, Bokara; Marathi: Bhokoda, Mori, Pimpari
Morphology and Occurrence
Casearia species are shrubs or trees. Leaves simple, alternate, distichous, usually pellucid punctate, lanceolate-ovate to elliptic-oblong, margin entire, serrate-dentate to pinnately veined, rarely 3-5 pliveined at the base, apex acute to acuminate, chartaceous, glandular pellucid on serrate-crenate teeth or margins, lateral veins very thin compared with midrib, petiole slender, long, sometimes with pair of glands at apex, stipules minute, caducous. Inflorescence clustered in shortly pedunculate axillary fascicles, few to many flowers, rarely solitary or cymes. Flowers bisexual, perigynous, pedicels short rarely sessile, bracts ovate, chartaceous, scalelike, sepals 4-5, imbricate, joined near base, free above, margin ciliate, persistent, petals absent Distribution :
Native : Native to Assam, Bangladesh, Cambodia, China South-Central, East Himalaya, India, Laos, Myanmar, Nepal, Pakistan, Thailand, Vietnam, West Himalaya
Global Distribution
Asia: Bangladesh, Bhutan, Cambodia, China, India, Laos, Myanmar, Nepal, Pakistan, Thailand, Vietnam.
Local Distribution : Andhra Pradesh, Assam, Bihar, Gujarat, Himachal Pradesh, Karnataka, Kerala, Madhya Pradesh, Maharashtra, Meghalaya, Odisha, Punjab, Sikkim, Tamil Nadu, Uttar Pradesh, West Bengal.
Chemical Constituants
Casearia graveolens is chemically rich in diverse and pharmacologically potent secondary metabolites, most notably clerodane-type diterpenoids, which are well recognized for their cytotoxic, anti-inflammatory, and neurotrophic properties.
Traditional / Ethno medicinal Uses
In traditional and ethnomedicinal systems across India, Southeast Asia, and China, Casearia graveolens has been widely used for its therapeutic benefits. It is traditionally employed to treat snake bites, tumors, fevers, skin diseases, ulcers, joint pain, rheumatism, diabetes, and diarrhea. The leaves and bark are used in poultices and decoctions, particularly in tribal and rural communities, for wound healing, anti-inflammatory applications, and relief from liver and stomach ailments. Some local traditions also use the bark as an abortifacient, while the root extracts are employed as a tonic and febrifuge. Reports also suggest its use in treating leprosy, venereal diseases, and digestive issues. These uses align well with modern findings, where C. graveolens extracts and isolated compounds have shown strong anticancer, anti-angiogenic,
Pharmacological Study Reported
Research Gap
Despite its widespread ethnomedicinal use across South and Southeast Asia for treating liver ailments, fevers, ulcers, and inflammatory Casearia graveolens remains significantly underexplored in terms of its hepatoprotective mechanisms. The plant is chemically rich in bioactive secondary metabolites, notably clerodane-type diterpenoids such as micromelin, casearlucin A, and caseariagraveolin, which have demonstrated potent cytotoxic, antiangiogenic, and neurotrophic activities. Additionally, flavonoids, coumarins, and lignans identified in the leaves possess well-established antioxidant and anti-inflammatory properties—two key pharmacological actions relevant to liver protection. However, while preliminary in vitro and anticancer studies have been conducted, there is a conspicuous absence of systematic research evaluating its hepatoprotective efficacy using both in vivo models of liver injury and computational tools such as network pharmacology and molecular docking. Specifically, no prior studies have examined its protective role in CCl?-induced hepatotoxicity, a widely accepted model for mimicking oxidative and inflammatory liver damage. Moreover, the multi-target potential of its phytoconstituents remains poorly characterized. Bridging this gap is crucial to substantiate its traditional use, identify its active hepatoprotective constituents, and explore its mechanism of action at the molecular level. Such integrative research could pave the way for developing safe, plant-based therapeutic candidates for managing hepatic disorders, particularly in resource-limited settings where access to conventional hepatoprotective drugs is constrained.
CONCLUSION
This review highlights the potential hepatoprotective properties of Casearia graveolens Dalz, a medicinal plant traditionally used to treat various ailments, including liver-related disorders. The plant's rich phytochemical profile, including clerodane-type diterpenoids, flavonoids, and coumarins, provides a promising foundation for its hepatoprotective effects
ACKNOWLEDGEMENT
The authors sincerely acknowledge the contributions of previous researchers whose work has provided valuable insights into the traditional uses, phytochemistry, and preliminary studies of casearia graveolens dalz. This review article is based on an extensive analysis of existing literature, and we acknowledge the contributions of all the authors whose studies have been cited in this article.We would like to thank our institutions for providing the necessary resources and support to conduct this review.
REFERENCES



Ashwini Helaskar, Dr. Karna Khavane, Aditi Mishra, Unveiling the Hepatoprotective Potential of Casearia Graveolens: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 1648-1659. https://doi.org/10.5281/zenodo.15869520
 10.5281/zenodo.15869520
10.5281/zenodo.15869520
