Channabasweshwar Pharmacy College (Degree), Latur, Maharashtra, India.
Transferosomes are ultra-deformable lipid vesicles developed to overcome the barrier function of the stratum corneum and enhance dermal and transdermal drug delivery. Composed of phospholipid bilayers integrated with membrane-softening surfactants known as edge activators, these vesicles exhibit remarkable elasticity, enabling them to traverse pores significantly smaller than their own diameter. This review comprehensively discusses the evolution, composition, mechanism of penetration, preparation methods, characterization parameters, advantages, limitations, therapeutic applications, and recent advancements in transferosomal systems. Mechanistically, transferosome penetration is driven by hydration-gradient–induced osmotic transport combined with stress-adaptive membrane flexibility. Compared to conventional liposomes and ethosomes, transferosomes demonstrate superior deformability and enhanced skin permeation under non-occlusive conditions. However, challenges such as phospholipid oxidation, drug leakage, scalability concerns, and regulatory standardization limit widespread commercialization. Future perspectives include nano-transferosomes, QbD-based optimization, hybrid microneedle systems, and stability enhancement strategies to facilitate clinical translation.
Transdermal drug delivery systems (TDDS) have gained considerable scientific and commercial attention over the last four decades as an alternative to conventional oral and parenteral drug administration[1–3]. The first FDA-approved transdermal patch (scopolamine) was introduced in 1979, and since then, multiple transdermal products have been successfully commercialized for drugs such as nicotine, fentanyl, estradiol, clonidine, testosterone, and rivastigmine. The global transdermal drug delivery market was valued at approximately USD 7–8 billion in recent years and is projected to grow steadily due to increasing demand for non-invasive and patient-compliant therapies.
Transdermal systems offer several pharmacokinetic and clinical advantages:
These advantages make transdermal delivery especially beneficial for chronic conditions such as hypertension, pain management, hormone replacement therapy, neurological disorders, and dermatological infections.
However, despite these advantages, only a limited number of drugs are suitable for transdermal administration due to the highly selective barrier function of the skin[3]
1.1 Anatomy and Physiology of Human Skin
Human skin is the largest organ of the body, accounting for approximately 16% of total body weight, with an average surface area of 1.5–2.0 m² in adults. The skin performs essential physiological functions including:
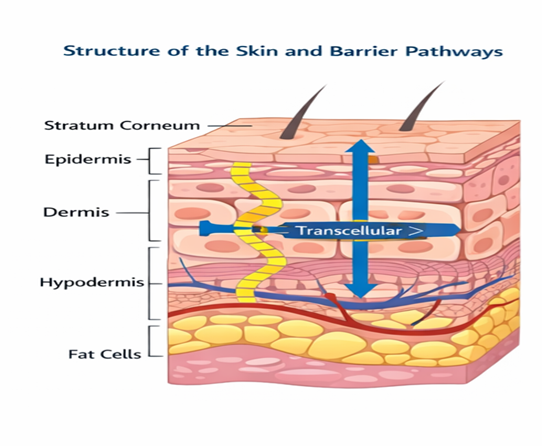
Structurally, the skin consists of three main layers:
1. Epidermis
The outermost layer, 50–100 µm thick (excluding stratum corneum). It consists of five sublayers:
2. Dermis
A 2–4 mm thick connective tissue layer containing:
The dermis plays a crucial role in systemic absorption once drugs cross the epidermis.
3. Hypodermis
Composed primarily of adipose tissue and connective tissue, providing structural support and insulation.
Among these layers, the stratum corneum is the principal barrier to drug permeation.
1.2 Structure and Biochemical Composition of Stratum Corneum
The stratum corneum is approximately 10–20 µm thick and consists of 10–25 layers of flattened, enucleated corneocytes embedded in a continuous lipid matrix.
The intercellular lipids are organized in highly ordered lamellar bilayers and consist primarily of:
These lipids are arranged in orthorhombic and hexagonal crystalline phases, which significantly restrict molecular mobility. The high degree of lipid organization reduces the diffusion coefficient (D) in Fick’s equation, making passive drug permeation extremely slow.
The stratum corneum exhibits a very low permeability coefficient, typically in the range of 10?? to 10?? cm/s for most drugs.
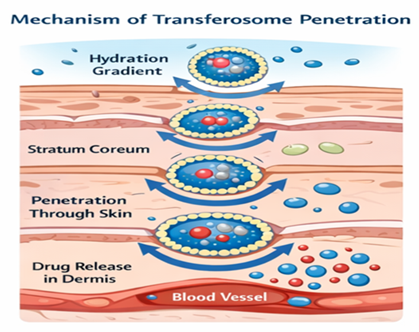
Additionally, trans epidermal water loss (TEWL) from skin surface creates a natural hydration gradient. TEWL typically ranges from 5–15 g/m²/h under normal conditions. This physiological gradient later becomes an important driving force for transferosomal penetration[5,6]
1.3 Physicochemical Requirements for Transdermal Drug Delivery
For a drug to be suitable for passive transdermal delivery, it must ideally satisfy the following criteria[1,3]
Very few drugs naturally meet all these criteria. For example:
Thus, enhancement strategies are essential for most therapeutic agents.
1.4 Limitations of Conventional Enhancement Techniques
Several strategies have been employed to enhance transdermal delivery:
1. Chemical Penetration Enhancers
Examples include ethanol, DMSO, and fatty acids.
Limitations: Skin irritation, barrier damage, unpredictable effects.
2. Physical Enhancement Techniques
Limitations:
3. Conventional Vesicular Systems
Liposomes, niosomes, and ethosomes were developed to improve drug deposition in skin layers.
However:
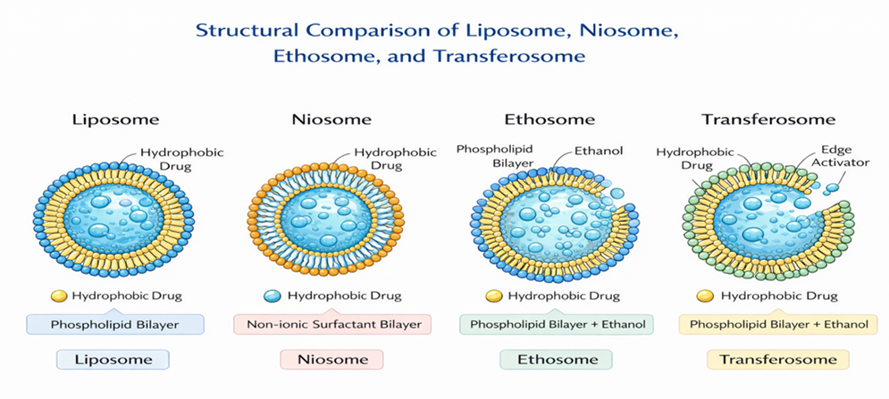
These limitations necessitated development of a more adaptable vesicular system.
|
Parameter |
Liposome |
Niosome |
Ethosome |
Transferosome |
|
Composition |
Phospholipids |
Non ionic surfactant |
Phospholipids +high ethanol |
Phospholipid+edge activator |
|
Deformability |
Low (rigid) |
Moderate |
Moderate – high |
Very high |
|
Skin penetration |
Limited to upper skin layer |
Improved vs liposomes |
Enhanced via ethanol fluidization |
Penetrate intact skin deeply |
|
Mechanism of enhancement |
Passive diffusion |
Surfactant mediated |
Ethanol – induced lipid disruption |
Hydration gradient+ membrane elasticity |
|
Irritation risk |
Low |
Low |
Possible ( due to high ethanol ) |
Low |
|
Drug suitability |
Hydrophilic and lipophilic |
Hydrophilic and lipophilic |
Mainly lipophilic |
Hydrophilic and lipophilic |
|
Stability |
Moderate |
Good |
Ethanol-related volatility issue |
Moderate (risk of lipid oxidation) |
|
Commercial translation |
Limited product |
moderate |
Research / development |
emerging
|
1.5 Concept and Evolution of Transferosomes
Transferosomes were introduced by Cevc and Blume in 1992 as “highly deformable vesicles” capable of crossing intact skin under non-occlusive conditions[5]. Their work demonstrated systemic insulin delivery in animal models following topical application, challenging the long-held belief that vesicular carriers could not traverse the SC barrier intact[6].
Over the past three decades, research on transferosomes has progressed through three distinct phases:
Despite significant academic interest, commercial translation remains limited, highlighting the need for critical evaluation of both strengths and constraints.
Transferosomes were introduced in the early 1990s as ultra-deformable lipid vesicles designed to overcome mechanical resistance of the stratum corneum.
They consist of:
The inclusion of edge activators destabilizes the lipid bilayer in a controlled manner, reducing bending modulus and allowing extreme flexibility.
Unlike traditional liposomes, transferosomes:
The penetration is not purely diffusion-driven but is strongly influenced by hydration gradient–induced osmotic transport.
1.6 Clinical Relevance and Emerging Need
Transdermal systems are particularly beneficial for:
In antifungal therapy, conventional topical creams often fail to penetrate the dense keratinized layers effectively. Transferosomes can enhance drug permeation through lipid lamellae and keratin-rich regions, making them promising carriers for antifungal and anti-inflammatory agents.
Furthermore, increasing interest in biologics and macromolecular therapeutics has renewed focus on deformable vesicles capable of transdermal peptide delivery.
2. Composition
Transferosomes are generally composed of:
The phospholipid-to-surfactant ratio is critical for vesicle deformability, entrapment efficiency, and stability[10,14].
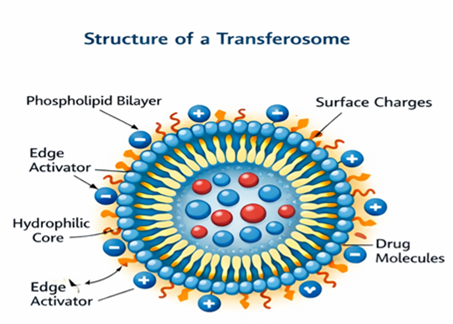
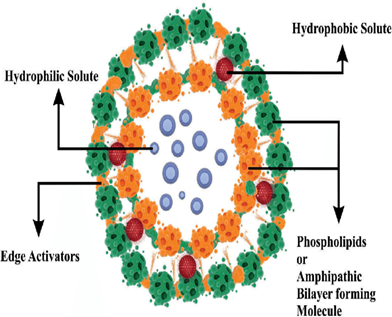
Figure: Transferosome Structure
3. TYPES OF TRANSFEROSOME.
Transferosomes can be classified based on composition, functional modification, and application. Although the basic structure remains the same (phospholipid + edge activator), researchers have developed different types to improve stability, targeting ability, drug loading, and therapeutic effectiveness. The major types of transferosomes are explained below in detail[6,9,12]
3.1 Classification based on composition
1) Conventional Transferosomes[6,9]
These are the basic and most commonly prepared transferosomes composed of phospholipids and edge activators such as surfactants. The phospholipids form the bilayer vesicle structure, while edge activators provide elasticity and deformability. These transferosomes are capable of penetrating through the stratum corneum by squeezing through narrow pores due to their flexible membrane. Conventional transferosomes can encapsulate both hydrophilic drugs (in the aqueous core) and lipophilic drugs (within the lipid bilayer). They are mainly used for transdermal delivery of anti-inflammatory drugs, antifungal agents, and analgesics. However, they may face stability issues during long-term storage due to oxidation of lipids and leakage of drug.
2) Modified Transferosomes[10,14]
Modified transferosomes are developed to improve the stability, penetration ability, and drug release profile of conventional transferosomes. In this type, additional components such as cholesterol, charge-inducing agents, or stabilizers are incorporated into the formulation. Cholesterol helps strengthen the vesicle membrane and reduce drug leakage. Charge-inducing agents improve vesicle stability by preventing aggregation. These modifications enhance entrapment efficiency and prolong drug release. Modified transferosomes are commonly used in the delivery of sensitive drugs that require better protection and controlled release.
3.2 Classification based on surface charge
1) Cationic Transferosomes[10,12]
Cationic transferosomes contain positively charged lipids or surfactants in their composition. These positively charged vesicles can easily interact with negatively charged biological membranes and skin surfaces, leading to better adhesion and enhanced drug penetration. This type is particularly useful for gene delivery, protein delivery, and targeting specific tissues. The positive charge also increases vesicle stability by preventing fusion and aggregation. However, excessive positive charge may sometimes cause skin irritation.
2) Anionic Transferosomes[10,12]
Anionic transferosomes contain negatively charged lipids or additives that provide a negative surface charge to the vesicles. These vesicles show improved dispersion stability because the negative charges repel each other and prevent vesicle aggregation. Anionic transferosomes are mainly used for the delivery of anti-inflammatory and anti-cancer drugs. They also provide controlled drug release and better storage stability compared to neutral vesicles.
3.3 Classification based on size
1) Nanotransferosomes[12,25]
Nanotransferosomes are transferosomes prepared in the nanometer size range using advanced techniques like high-pressure homogenization or microfluidization. The small size increases surface area and enhances skin penetration. These nano-sized vesicles provide better drug absorption, improved bioavailability, and uniform drug distribution. Nanotransferosomes are widely used in the delivery of hormones, peptides, vaccines, and cosmetic agents such as anti-aging and skin-lightening drugs[12,25]
3.4 Functionalised and targeted transferosomes
1) Ligand-Targeted Transferosomes[10,22]
This is an advanced type of transferosome in which specific ligands such as antibodies, peptides, or other targeting molecules are attached to the surface of vesicles. These ligands help direct the transferosomes toward specific cells or tissues, improving targeted drug delivery. This type is mainly used in cancer therapy and site-specific drug delivery. It reduces drug loss, enhances therapeutic efficiency, and minimizes side effects.
3.5 Application based variants
1) Herbal Transferosomes[23,24]
Herbal transferosomes are designed for the delivery of plant-based active compounds such as curcumin, aloe vera extract, and other herbal drugs. Many herbal compounds have poor solubility and low skin penetration when applied directly. Transferosomal encapsulation improves their stability, penetration, and therapeutic effectiveness. These are widely used in cosmetic and dermatological applications such as anti-aging creams, anti-acne gels, and skin-brightening formulations.
2) Transferosomal Gels[23]
Transferosomes are often incorporated into gel bases to improve ease of application and patient compliance. These are not structurally different vesicles but are considered a formulation type. Transferosomal gels provide controlled drug release, better skin contact, and prolonged retention at the application site. They are widely used for topical treatment of acne, psoriasis, inflammation, and fungal
4. Mechanism of Penetration
Transferosome penetration is primarily driven by the transepidermal hydration gradient. Evaporation from the skin surface generates osmotic stress, propelling vesicles inward[5,6]. Edge activators enhance bilayer fluidity, allowing vesicles to deform and traverse narrow intercellular lipid channels[6,8]. Intact vesicles can penetrate pores smaller than their diameter, releasing drugs gradually during transport or after reaching deeper layers[7,9].
4.1 Mechanistic Controversies
Transferosomes were originally described as ultra-deformable vesicles capable of penetrating intact skin driven by the transepidermal hydration gradient[5,6]. However, subsequent imaging studies using confocal microscopy have produced mixed findings. Some investigations suggest intact vesicle transport, whereas others indicate partial vesicle disruption during penetration, implying that transferosomes may also function as penetration enhancers by fluidizing intercellular lipids before drug release. Therefore, whether intact vesicular transport occurs across the entire skin thickness remains an area of ongoing scientific debate requiring further mechanistic validation
5. METHODS OF PREPARATION.
Transferosomes are commonly prepared using methods similar to liposome preparation but with the addition of edge activators to provide deformability. The selection of preparation method affects vesicle size, entrapment efficiency, stability, and drug release profile. Various techniques have been developed to produce transferosomes with controlled characteristics suitable for transdermal drug delivery[15,16]
List of All Major Methods
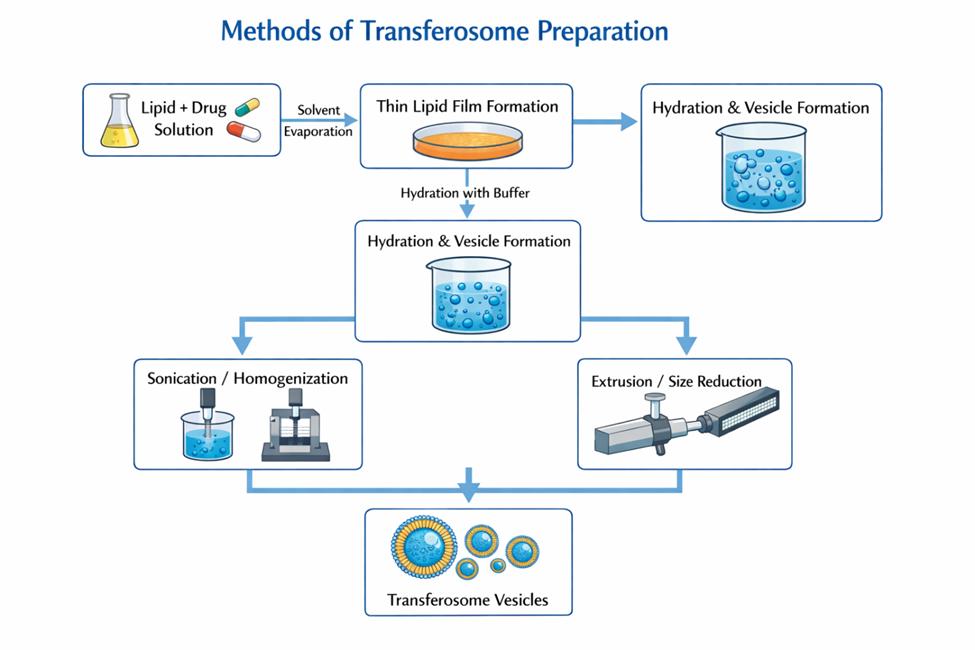
1) Thin Film Hydration Method[15,16]
(Most commonly used and most important)
This is the standard and widely accepted technique for the preparation of transferosomes. In this method, phospholipids and edge activators are dissolved in an organic solvent such as chloroform and methanol. The organic solvent is then removed using a rotary evaporator under reduced pressure at a controlled temperature, leading to the formation of a thin lipid film on the inner wall of a round-bottom flask. This film contains uniformly distributed lipid components.
After complete removal of the solvent, the dried lipid film is hydrated using an aqueous phase containing the drug. Hydration is carried out at a temperature above the lipid transition temperature with continuous rotation. During hydration, the lipid film swells and peels off, forming multilamellar vesicles. These vesicles are then subjected to sonication or extrusion to reduce their size and obtain small unilamellar transferosomes. This method produces vesicles with high drug entrapment and uniform size distribution.
2) Reverse Phase Evaporation Method[15]
In this technique, phospholipids and edge activators are dissolved in an organic solvent such as ether or chloroform. The drug is dissolved in an aqueous phase and mixed with the organic phase to form a water-in-oil emulsion. This emulsion is then sonicated to achieve uniform dispersion.
The organic solvent is slowly removed under reduced pressure, leading to the formation of a viscous gel-like structure. Continued evaporation results in the formation of vesicles as the organic solvent is completely removed. This method is particularly useful for encapsulating hydrophilic drugs because a large aqueous core is formed, resulting in high entrapment efficiency.
3) Ethanol Injection Method[17]
In this method, phospholipids and edge activators are dissolved in ethanol. The ethanolic solution is then slowly injected into an aqueous phase containing the drug under constant stirring. As ethanol mixes with water, lipid molecules precipitate and spontaneously form vesicles.
This technique is simple and does not require complex equipment. It produces small vesicles with relatively uniform size. However, complete removal of ethanol is necessary to ensure stability and safety of the final formulation. This method is particularly useful for temperature-sensitive drugs as it does not involve high temperatures.
4) Vortexing–Sonication Method[15,16]
In this method, lipid components and edge activators are mixed with an aqueous drug solution in a suitable container. The mixture is vortexed vigorously to disperse lipids in the aqueous medium. This results in the formation of large multilamellar vesicles.
The dispersion is then subjected to probe sonication or bath sonication to reduce vesicle size and form small, uniform transferosomes. Sonication breaks down larger vesicles into smaller ones and improves drug encapsulation efficiency. This method is simple and suitable for laboratory-scale preparation with reproducible vesicle formation.
5) Freeze–Thaw Method[15]
This method is often used as a supportive technique to improve entrapment efficiency. Transferosomal suspensions prepared by any primary method are subjected to repeated freezing and thawing cycles. The dispersion is frozen at very low temperatures and then thawed at room temperature.
This process causes disruption and reformation of vesicles, allowing better mixing of drug molecules within the vesicular structure. It increases drug encapsulation, especially for hydrophilic drugs. After freeze–thaw cycles, the formulation is sonicated to obtain uniform vesicle size.
6) High Pressure Homogenization Method[18]
This method is mainly used for large-scale production. In this technique, lipid and aqueous phases are mixed to form a coarse suspension. This suspension is passed through a high-pressure homogenizer at very high pressure.
The intense shear forces and turbulence reduce vesicle size and produce uniform, nano-sized transferosomes. This method improves physical stability, uniformity, and scalability of the formulation. It is particularly useful in industrial manufacturing.
7) Suspension Homogenization Method[18]
In this method, lipids and edge activators are first dispersed in an aqueous phase to form a suspension. This suspension is then homogenized using mechanical homogenizers to reduce particle size.
Continuous homogenization helps in the formation of small vesicles with uniform size distribution. This method is easy to scale up and suitable for commercial production.
8) Hand Shaking Method[15]
This is a basic and simple technique similar to the thin film hydration method but performed manually. Lipids are dissolved in organic solvent and the solvent is evaporated by gentle heating and hand shaking. This forms a thin lipid film.
The film is then hydrated with an aqueous drug solution while shaking continuously. This results in the formation of vesicles. The dispersion is later sonicated to reduce size. This method is mostly used for small laboratory experiments.
9) Microfluidization Method[12,18]
This is an advanced technique used to prepare very small and uniform vesicles. Lipid and aqueous phases are forced through microchannels at high velocity using a microfluidizer. The collision of streams creates high shear forces that form nano-sized transferosomes.
This method provides excellent control over vesicle size, uniformity, and stability. It is suitable for large-scale and high-quality production.
6. Characterization
Key parameters include:
6.1 Quantitative Characteristics
Transferosomes typically exhibit vesicle sizes ranging from 50–300 nm[12] with polydispersity index values below 0.3 indicating uniform size distribution. Entrapment efficiency generally ranges between 60–90%[9] depending on lipid composition and drug properties. Zeta potential values of ±20 to ±40 mV[18] contribute to electrostatic stability. The deformability index of transferosomes is significantly higher than conventional liposomes, confirming their ultra-flexible membrane characteristics
7. Advantages
8. Limitations
9. Applications
10. Recent Advances (2020–2025)
Research highlights:
11. Regulatory and Commercial Perspective
Despite promising preclinical outcomes, large-scale commercialization of transferosomal formulations remains limited[10]. Regulatory challenges include batch-to-batch variability, oxidative degradation of phospholipids, lack of standardized deformability measurement methods, and insufficient long-term safety data. Industrial scalability requires advanced manufacturing techniques such as high-pressure homogenization and microfluidization under Good Manufacturing Practice (GMP) conditions. Clear regulatory guidelines for vesicular nanocarriers are essential to facilitate clinical translation and commercialization.
12. Future Outlook
Future research should focus on integration with microneedle-assisted delivery[22], AI-based formulation optimization, large-scale GMP-compliant manufacturing, improved antioxidant stabilization systems, clinical trials for peptide and vaccine delivery, and standardized deformability testing protocols.
13. CONCLUSION
Transferosomes represent a significant advancement in vesicular drug delivery systems by combining membrane elasticity with hydration-gradient–driven transport to overcome the stratum corneum barrier. Compared with conventional liposomes, niosomes, and ethosomes, transferosomes demonstrate superior deformability and enhanced dermal penetration under non-occlusive conditions. They are capable of delivering hydrophilic, lipophilic, and macromolecular drugs with improved bioavailability and sustained release profiles. Nevertheless, challenges including oxidative instability, drug leakage, high production cost, and limited regulatory standardization restrict their widespread commercial adoption. With continued innovation and regulatory clarity, transferosomes hold substantial promise for next-generation transdermal therapeutics.
REFERENCES




Akash Kawale, Shivappa Nagoba, Krishna Patil, Manmath Palaskar, Transferosomes: Ultra-Deformable Vesicular Carriers for Enhanced Transdermal Drug Delivery, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 1850-1862. https://doi.org/10.5281/zenodo.19072023
 10.5281/zenodo.19072023
10.5281/zenodo.19072023
