Dr. K. V. Subba Reddy Institute of Pharmacy, Kurnool, India
In recent years Gastro retentive drug delivery system has gained researcher’s in the field of oral drug delivery. Various GRDDS approaches can be utilized to retain the dosage forms in the stomach and to releases the drug slowly for an extended period of time. GRDDS can be used to prolong the residence time of delivery system in the stomach. This results in targeting of drug release at a specific site for the systemic or local effects. GRDDS can be used to overcome challenges associated with conventional oral dosage forms and to release the drug at a specific absorption site to improve bio availability of particular drug substance. The challenges include fast gastric emptying of the dosage form which results in the poor bio availability of the drug . Prolongation of the retention of drugs in stomach those having low solubility at high intestinal PH improves solubility of drugs. GRDDS has proved to be effective in systemic actions as well as in local actions to treat gastric or duodenal ulcers. Local activity in the upper part of the small intestine can be obtained by improving the residence time of delivery system in the stomach. The system is useful for drugs which are unstable in the intestine or having a low solubility/ permeability in the small intestine. Various GRDDS approaches include high density [sinking] systems, low-density [floating systems], Mucoadhesive, expandable, unfold able, super porous hydrogel systems, and magnetic systems.
Oral route is the most appropriate and preferred route for systemic or local delivery of any drug. Oral controlled release delivery systems are gaining researcher's interest to obtain improved therapeutic merits, such as simple dosing, patient compliance, and dose safety. Drugs that are absorbed easily through GI tract having short half lives are rapidly eliminated from systemic circulation.
Thus, to achieve therapeutic activity, frequent administration of those drugs is becoming essential. The fast gastric emptying of other simple oral dosage forms results in bio availability problems of many drug molecules. To overcome this drawback, the preparation of oral sustained/ controlled release formulations is done, which helps to enable an effective concentration of the drugs in the systemic circulation by slowly releasing the drug into the gastrointestinal tract [GIT] for extended period of time. When given through the oral route, this drug delivery can be maintained in the stomach and release drug in a controlled/sustained manner. Thus, the drug is supplied without interruption to the specific site of absorption in the GIT.
STOMACH PHYSIOLOGY:
Knowing the stomach physiology and associated gastric emptying process plays the major role in the success of GRDDS. The stomach is present in the upper left part of abdominal cavity immediately after diaphragm12 The human stomach consists of three anatomical parts which are fundus, body, and antrum or pylorus15, remaining volume of the stomach is only 25-30ml after food has been process in the stomach, while the undigested material is stored at the region formed by fundus and the body. Antrum is the bottom most part of the stomach which acts as a gastric emptying pump by ejecting the stomach contents16, The stomach and duodenum are separated by the pylorus, which has an important role in residence time of the ingested substances in the stomach. The fasting or fed state influences the motility pattern of individual17,18, the gastric motility pattern has different cycles of activity. Each cycle is continue for four phases and the time span of each cycle is 90-120
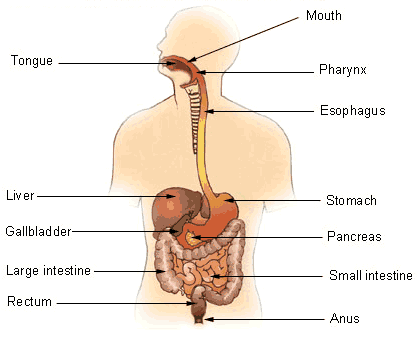
Fig:01- Stomach Physiology
Prolongation of the retention of drugs in stomach those having low solubility at high intestinal pH and improves the solubility of drugs1. Various drugs such as captopril, metronidazole. and ranitidine HCL are liable to degradation in colonic area2, Gastro retentive drug delivery system (GRDDS) has proven to be effective in systemic actions as well as in local actions to treat gastric or duodenal ulcer3,5.
GRDDS have two main problems which are the short gastric retention time (GRT) of GRDDS in the stomach and unpredictable short gastric emptying time of the delivery system (gastric emptying time [GET]), which may lead to insufficient drug release from the dosage form in the absorption area which results in low efficacy of administered drug. To develop a site-specific oral controlled release drug delivery system, it is beneficial to improve a GRT of drug formulation. Prolonged gastric retention improves bio availability, increases the duration of drug release, and increases the solubility of drugs those having a little solubility at high pH environment of the intestine or degrade in alkaline PH6,7.
Local activity in the upper part of small the intestine can be obtained by improving the residence time of delivery system in the stomach. GRDDS can be utilized to prolong the residence time of delivery system in the stomach. This results in targeting of drug release at a specific site for the systemic or local effects. Since the last few decades, different types of GRDDS approaches have been designed and developed. These approaches include: High density or sinking systems which can be retained in the basal part of the stomach8 low density or floating systems that continue to float on gastric fluid 9,10, mucoadhesive system causes adhesion to the mucous of the stomach11, unfold able, extendible, or swellable systems that restrict the emptying of delivery system out from the pyloric sphincter of the stomach 12 super porous hydrogel13 systems magnetic systems 14 etc.
*Conventional oral delivery is widely used in the pharmaceutical field to treat diseases. However or at intestine. It is obtained by retaining dosage form into stomach and drug is being released at controlled manner to specific site either in stomach, duodenum and intestine.
FORMULATIONS OF GRDDS:
PROPRANALOL HYDROCHLORIDE:
Dissolution of all the formulations was carried out. It was observed that drug release is controlled by the polymer type and its concentration. Many of the polymers used were found to be unsuitable for formulating floating tablets because of their lack of abilities to form matrix and control the release of drug or poor buoyancy shown by the formulations containing those particular polymers. So, it was decided to use HPMC K4 M and HPC to formulate floating drug delivery system of propranolol hydrochloride. Tablets were directly compressed with oval flat faced die.
EVALUATION FOR GRDDS:
The powder blend was evaluated for flow properties different tests that were carried out are angles of repose, loose bulk density, tapped bulk density and compressibility index, and Hausner ratio was calculated.
Tablets were subjected to various tests like hardness, friability, uniformity of drug content, and uniformity of mass of single dose preparation as per united state pharmacopoeia [USP].
After achieving lag time, the time taken for a tablet to remain float on the surface of the dissolution medium is called floating time.
: 37 ± 0.5 C
Various Factors Affecting Gastric Residence
Period of Delivery Systems:
The stomach anatomy and physiology parameters should be size of particles must be within the range of 1-2mm to pass through the pyloric sphincter into the small intestine22. The important factors that affect the residence time of the delivery systems in the stomach are food intake and its nature, frequency of intake density23,25, size and shape of dosage forms25,26 patient gender, age, sex, body mass index, and disease status of the individual person (i.e., Diabetes and Crohn’s disease)15,27,28 and drugs that have effects on gastrointestinal transit time such as anticholinergic drugs such as atropine or pro-kinetic agents such as metoclopramide and cisapride29.
DENSITY OF DOSAGE FORMS:
Density of dosage form also influence the gastric emptying rate of the dosage form. Density also plays a key role in determining the location of the delivery system in the stomach. Dosage forms with low density than gastric contents can float on the surface, whereas high-density systems go down to the bottom of the stomach. Low-density system or floating systems should maintain bulk density less than 1 g/cm, so as to remain buoyant on the gastric contents15.
SHAPE AND SIZE OF THE DOSAGE FORMS:
Shape and size of the dosage forms are the important factors in designing indigestible single unit dosage forms. The mean GRT of a non-floating dosage form is varying according to their size. In most cases, bigger the dosage form the better will be the gastric residence period. The larger size dosage form cannot be passed rapidly through the pyloric sphincter into the intestine. Dosage forms which having the diameter greater than 7.5mm shows better GRT as compared to that of9.9mm30. Likewise, as compared to other shapes, ring shaped, and tetrahedron shaped devices show better GRT6.
FOOD INTAKE AND ITS NATURE:
Factors such as food intake, viscosity and amount of food, caloric value, and recurrence of feeding have an intense effect on gastric retention of dosage forms. The existence and non-existence of food in the GI tract also influence the gastric retention of dosage forms. In general, the existence of food material in the GI tract increases the GRT of the dosage form and therefore drug absorption improved by allowing its residence at the specific absorption site for the longer period of time. The increase in stomach acid and caloric value slows the GET15, which can increase the gastric retention of delivery system24.
EFFECT OF SEXUAL CATEGORY, POSITION AND AGE:
Normally, females show a slower rate of gastric emptying as compared to males3, The effect of position does not have any notable difference in the mean GRT for individuals in standing, ambulatory or lying position. In case of aging peoples, gastric emptying is slowed down.
Possible drug candidates for GRDDS31,46
1. Drugs those have local activity in the stomach (e.g., ranitidine, amoxicillin, levofloxacin and metronidazole)
2. Drugs with narrow GI absorption window (e.g., riboflavin, pregabalin, and metformin)
3. Drugs that are unstable or degrade in intestinal or colonic environment (e.g., verapamil and captopril)
4. Drugs those have little solubility at high pH of the intestine (e.g., ofloxacin and cinnarizine).
Drugs those are Unsuitable for GRDDS [21]
1. Drugs with low acidic solubility (e.g., phenytoin)
2. Drugs those are unstable or degrade in the acidic environment of the stomach (e.g., erythromycin)
3. Drugs those are used for targeted release in the colon(e.g., corticosteroids).
Various Approaches to accomplish Gastro retention of dosage forms:
High density or sinking systems or non-floating systems. In this approach, the density of formulation must be superior to the density of normal gastric content (1.004g)47. These formulations are developed by coating drug on a heavy Core or mixed with inert substances such as iron powder, barium sulfate, zinc oxide, and titanium oxide48 Materials increase density up to 1.5-2.4 g/cm3. A density of almost 2.5glcm found to be necessary for significant prolongation of GRT49. This system has its disadvantage that the size of form is increased to achieve the high density.
Low density systems or floating systems:
The FDDS is an important dosage form which helps in obtaining sufficient bio availability by prolongation of GRT50 . The floating system was first introduced by Davis in 1968 depicted the Concept of the floating. This delivery system is suitable for drugs with system an absorption window in the stomach or upper small intestine51,42.It is also helpful for the drugs that have action locally in the proximal portion of GIT such as antibiotics used for eradication of Helicobacter pylori in the treatment of peptic ulcer33. These have a bulk density less than gastric fluids and therefore remain afloat on the stomach contents without influencing the gastric emptying rate for an extended period of time and the drug is released slowly at a desired rate from the system. After the release of active drug, the delivery system is emptied. from the stomach24. The key necessities for floating drug delivery systems are:
The low density is obtained from the entrapment of air(e.g., hollow chamber]5 or due to merging low-density materials50 (fatty materials oils5 or foam powder]8,9. Recently, a single unit floating system was formulated by utilizing polypropylene foam powder, matrix forming polymers, drugs, and filters5 Single unit dosage forms may cause problems such as sticking together or being blocked in the GIT which may Cause GI irritation. Multiple unit floating systems may be an attractive alternative as they lower the chances of dose dumping6. Many multiple unit floating systems such as air compartment multiple unit system 61 hallow-micro spheres (micro balloons) formulated using the emulsion solvent diffusion method6 micro particles based on low-density foam powders50,6 beads prepared by emulsion, gelatin method51,6 can be distributed widely throughout the GIT, providing the opportunity of obtaining a long lasting, and more reliable release of active medicament. Depends on the mechanism buoyancy, two clearly different techniques which are effervescent and non-effervescent drug delivery systems have been used in the formulation of FDDS.
Effervescent or gas generating systems:
In this system, buoyancy can be resulted from generation of gas bubbles. These floating systems use the matrices developed using swellable polymers such as poly saccharides (e.g., chitosan), effervescent agents such as sodium bicarbonate16, sodium citrate, or tartaric acid. In these systems, the dosage form floats on the gastric fluid in stomach due to liberation of CO2. Other approaches and materials are a mixture of sodium alginate and sodium bicarbonates, multiple unit floating dosage forms that produce carbon dioxide gas in the stomach after ingestion, floating mini capsule having a core of sodium bicarbonate, lactose, and polyvinyl pyrrolidone coated with hydroxy-propyl methyl cellulose (HPMC), and floating system based on ion exchange resin technology6 etc. Bi layer or multi layer system has been designed6. Gas generating agents are incorporated in any of these layers after the drug and excipients are formulated independently.
Non effervescent systems:
These floating systems are generally prepared by gel forming or swellable cellulose type hydro-colloids, poly-saccharides, or matrix forming polymers such as polyacrylate, polycarbonate, polystyrene, polymethacrylate15,6. In one approach, mixing of medicament with a gel forming hydrocolloid which in Contact with gastric fluid after oral administration maintain a relative integrity of shape and a bulk density lower than that of gastric content. The air trapped by the swollen polymer grant float-ability to these dosage forms6. The excipients .utilized very commonly are HPMC, polyacrylate, polyvinyl acetate, Carbopol, agar, sodium alginate, calcium chloride, polyethylene oxide, and polycarbonates6. This system can be again classified into following sub types:
Hydro dynamically balanced systems (HBS):
These systems were first designed by Sheath and Tossounian in 1984. HBS are consisting of drug with gel forming hydrocolloids that remain buoyant on the gastric content. One or additional gel forming polymers are used to prepare these single unit dosage forms. In general, used excipients are HPMC, hydroxy propyl cellulose, polycarbophil, sodium carboxymethyl, alginic polyacrylate, polystyrene acid. The polymer mixed with drug and generally is given in HBS capsule. The capsule shell breakdown in contact with water and swells which lead to the formation of gelatinous barrier, which gives float-ability in dosage form in gastric content for a longer period of time. The erosion of the exterior layer permits penetration of water into the internal layers maintaining the surface hydration and float-ability to the drug delivery system. Various approaches have been tried and examined to improve efficiencies of the floating HBS68
Micro balloons/ hollow micro spheres:
Micro balloons/ hollow micro spheres are loaded with APIS in their outer polymer shelf were formulated using simple solvent evaporation or solvent diffusion/evaporation methods42, to improve the residence time of the delivery system in the stomach. Some common polymers used to prepare these systems are cellulose acetate, polycarbonate, calcium alginate, low methoxylated pectin, agar, etc. The quality of polymers, the plasticizer polymer proportion, and solvent used for preparation have a significant effect on the floating and drug release from the delivery system. The micro balloon remains buoyant without interruption on the surface of an acidic dissolution medium more than 12hrs . Hollow micro spheres are ranked among the most promising floating system because they have combined the advantages of a multiple unit system and good buoyancy.
Alginate beads:
Recently, multiple unit floating systems were prepared that is based on cross linked beads, The system was prepared using calcium ion and low methoxylated pectin calcium ions + low methoxylated pectin and sodium alginate. Sodium alginate solution is dropped into an aqueous solution of CaCl2, which leads to the precipitation of calcium alginate. These beads are then separated and desiccated using air convection and freeze drying, results in the formulation of porous system which can remain floating for more than 12hrs. These beads increase the GRT more than 5.5hrs. Recently, floating alginate beads prepared using a gas generating agent such as calcium sodium bicarbonate and carbonate (CaCO3) (NaHCo3)51.
Bio adhesive or mucoadhesive drug delivery system:
These systems were first introduced by Park and Robinson in 1984 Mucoadhesive DDS are utilized as delivery devices within humans to increase drug absorption at a specific site. In this approach, mucoadhesive polymers are used49,50 which hold on to the epithelial surface in the stomach. Therefore, they can prolong the gastric retention. The delivery system can hold onto the mucosal surface by various mechanisms. These mechanisms include48,41.
1) The wetting theory- is based on the ability of mucoadhesive polymers to spread and form contact with the mucous layers.
2) The diffusion theory is based on interpenetration of mucin strands into the porous configuration of the polymer substrate.
3) The absorption theory - states that the bio adhesion is the result of VanderWalls forces and hydrogen bonding.
4) The electronic theory - is based on attractive electrostatic forces between the glycoprotein mucin network and the bio adhesive materials.
Materials that exhibit bio adhesive property are chitosan, HPMC, acrylic acid, cholestyramine, sodium alginate, sucralfate, dextrin, tragacanth, polyethylene glycol, polylactic acid, etc. Despite some of these polymers are effectively produce bio adhesion, it is hard to maintain this bio adhesion due to rapid turnover of mucus in the GIT30.
Expandable, Unfold able and swellable systems:
An expandable system can achieve a longer GRT by increasing its shape or volume. These systems were first designed for veterinary use and then explore for the human use6 . A dosage form can be retained in the stomach still after gastric transit when it is larger in size than the diameter of the pyloric sphincter. In general, these systems composed of hydrophilic polymers, when polymer comes in contact with gastric fluid it absorbs water and becomes swollen12. The swelling and drug release is occur due to the process of diffusion. However, care should be taken that the dosage form must be small enough to swallow and should not cause gastric blockage alone or by accumulation. Thus, their configurations should be considered while developing expandable systems to prolong GRT.
1. A small design for oral use
2. An expanded gastro retentive form
3. A small form that allows clearance subsequent to drug release from the device.
Unfold able systems are prepared from biodegradable polymers which are folded and encapsulated inside a carrier which degrade in the stomach12 Unfold able systems are available in the different geometric forms Such as a tetrahedron, ring, or planner membrane (4-limbed cross or 4-label disc form) of biodegradable polymer compressed within a capsule which extends in the stomach. Swellable systems are also retained in the stomach because of their mechanical properties. The Swelling is generally caused due to osmotic absorption of water. The expandable systems have some dis-benefits such as the storage of easily hydrolysable polymers is problematic26. biodegradable polymers are most difficult to industrialize and not cost effective. Permanent retention of rigid, large single-unit expandable drug delivery dosage forms may cause brief obstacle, intestinal sticking, and gastric diseases12.
Super porous hydrogel system:
In this approach, the GRT is improved by super porous average pore size greater than 100um. They swell to an equilibrium size from minute due to water uptake by capillary wetting through numerous interconnected open pores16. They swell to large size up to 100 or more45. These systems utilize the highly swellable polymers such as croscarmellose sodium and sodium alginate43. These formulations have high mechanical strength and elastic properties.
Raft forming systems:
These systems are developed using gel forming polymers and effervescent excipients so as to obtain sustained drug delivery. These systems are effective in achieving localized effect as they form a blockade between esophagus and stomach. Therefore, System can be utilized for the treatment of peptic ulcer and GASTRO esophageal REFLUX disease. After contact with stomach fluid these systems become Swelled and forms a viscous cohesive gel which results in the formation of a continuous layer called as raft 14. The antacid raft forming system is also developed recently in which sodium alginate is used as gel forming polymer, sodium bicarbonate, and acid neutralizer as gas generating agents. The raft floats on the gastric fluid due to generation of CO2 that reduce the bulk density of the system.
The raft can remain floating on the gastric fluid for a few hours and release the drug in a sustained manner. Such rafts are especially useful for the delivery of antacid drugs. These systems can be disrupted by MMC as they have weak mechanical strength. The mechanism includes the formation of viscous cohesive gel in contact with gastric fluids, where in each portion of the liquid swells forming a continuous layer called a RAFT. This raft floats on gastric fluids because of low bulk density created by the formation of CO2.
Magnetic system:
In this approach, external magnet is used to improve GRT of the dosage form which consists of a small internal magnet along with the excipients and API, the external magnet is placed on the abdomen over the position of the stomach that controls the position of internal dosage form or improves the GRT of dosage form14, The external magnet must be placed with a degree of accuracy that may reduce patient compliance51,Some often used drugs in the development of GRDDS and some gastro retentive products available in the market. Although magnetic system seems to work, the external magnet should be positioned with a degree of precision that might compromise patient compliance. The technological approach in rabbits with bio adhesive granules containing ultra-fine ferrite. They guided them to esophagus with an external magnet for the initial 2 minutes and almost all the granules were retained in the regions after 2 hrs.
Merits of GRDDS:
*The bio availability and therapeutic effects can be improved for those drugs which get metabolized in the alkaline environment of the intestine.
*Lessen the frequency of dosing and thus improves patient compliance
*They have a benefit over their conventional system as they can use to overcome gastric emptying time (GET). These systems are likely to remain floating on the gastric fluid without influencing the intrinsic rate of emptying as their bulk density is lower than that of the gastric fluids *GRDDS can prolong and sustain the drug release Iron the dosage form which facilitates local delivery In the stomach and small intestine. Thus, these Systems are useful to treat diseases related to the stomach or small intestine.
* The controlled, slow delivery of the active drug from the gastro retentive delivery systems provides adequate local action at the diseased site thus minimizes or eliminates the systemic disclosure of drugs. This site specific drug delivery minimizes undesirable effects of drugs
* GRDDS can reduce the fluctuations of drug concentrations and effects. This helps to avoid concentration dependent adverse effects that are associated with peak concentrations. This aspect is of a special importance for drugs with a narrow therapeutic index.
*GRDDS can diminish the counter activity of the body, leading to higher drug effect.
*Reduction in fluctuation in drug concentration ensures increased selectivity in receptor activation.
*The continuous release of drug for an extended period from the GRDDS allows extension of the time Over the critical concentration and hence intensifies the pharmacological effects and improves chemical outcomes.
Challenges involved in GRDDS:
The GRDDS are stomach specific and required to retain in the stomach only. Therefore, the retention of the dosage form in the stomach or in the upper part of the small intestine for a long period of time until all drug from the system is released at predetermined rate is the biggest challenge in formulating GRDDS. The gastric emptying process is highly variable and depends on various factors. However, the main factor is dosage form and fasted or fed state of the stomach. The gastric emptying time is also influenced by the factors such as food, caloric content, gender, and age. The process of gastric emptying is also prolonged by high fat and high calories containing food. The GRT is varying and related to the patients age, gender, size and shape of dosage forms, individuals disease state, and body mass index. The GRT is also affected by the pylorus. Another fact is the animals (dog or rabbit) that have different size of the pylorus and its peristaltic movement than that of human beings. Indigestible polymers and fatty acid salts also alter the motility pattern of the stomach under fed 3 conditions and assist in decreasing gastric emptying rate. Therefore, it is necessary to conclude the results a carefully.
ADVANTAGES OF GRDDS:
Enhanced bio availability,
DISADVANTAGES OF GRDDS:
Limitations of GRDDS:
CONCLUSION
Based on the literature reviewed, it may be concluded that GRDDS can provide numerous advantages for drugs with low bio availability as these delivery systems restrict the absorption of the drug in the upper GIT and they can be delivered efficiently thereby improving their absorption and intensifying absolute bio availability. The in vivo studies are important to create the optional dosage form for a specific drug because of complexity of pharmacokinetics and pharmacodynamics parameters. Gastro retentive drug delivery has great significance to increase the therapeutic efficacy of drugs those having a narrow absorption window, high solubility at acidic pH (in Stomach), and low solubility or instability at alkaline pH (intestine). But understanding the anatomy and physiology of the stomach, the effect of formulation and process variables on the quality of dosage form is necessary for successful GRDDS design. Even though numerous GRDDS have been reported in the literature such as low or high density, bio or mucoadhesive, and magnetic systems, but their effectiveness or clinical significance should be necessary to studied. To understand the influence of formulations and process variables of the dosage forms performance QBD approach can be used.
REFERENCES

Dr. C. S. Parameswari*, Gastroretentive Drug Delivery System, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 647-658. https://doi.org/10.5281/zenodo.14293650
 10.5281/zenodo.14293650
10.5281/zenodo.14293650
