1 MET’s Institute of Pharmacy, MET Bhujbal Knowledge City, Nashik, Maharashtra, India
2 K.V.N.N.S.P.S's Institute of Pharmaceutical Education and Research, Nashik
Transdermal drug delivery systems (TDDS) have emerged as a promising alternative to conventional dosage forms due to their ability to deliver drugs directly into systemic circulation while bypassing hepatic first-pass metabolism. Conventional transdermal patches, although widely used, often face limitations such as poor skin permeability, restricted drug load, and local irritation. Recent advancements have focused on novel carriers, nanotechnology-based systems, microneedles, iontophoresis, and other enhancement techniques to overcome these barriers. This review highlights the evolution of transdermal systems beyond conventional patches, discussing their principles, types, applications, drug selection criteria, excipients, manufacturing methods, evaluation techniques, marketed formulations, and recent advances. Emphasis is given to how modern technologies expand the therapeutic scope of TDDS by improving drug absorption, patient compliance, and clinical outcomes.
Drug delivery is the process of administering an active pharmaceutical ingredient (API) in a way that ensures its therapeutic action at the desired site of effect. Conventional routes such as oral and parenteral administration often face challenges like poor bioavailability, enzymatic degradation, and hepatic first-pass metabolism [1]. To address these issues, advanced drug delivery systems, including transdermal routes, have been developed [2].
The use of skin for medicinal application dates back to ancient civilizations that relied on ointments, plasters, and herbal extracts [3]. The modern era of transdermal therapy began in 1979 with the U.S. FDA approval of the first scopolamine patch for motion sickness [4]. Later, transdermal patches for nitroglycerin, nicotine, and fentanyl demonstrated their value in chronic therapy [5].
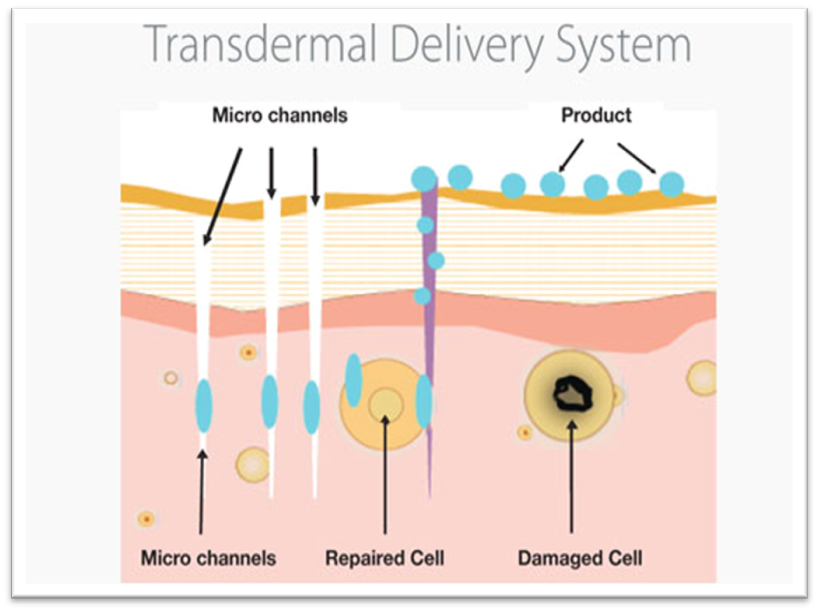
Fig 1. Transdermal Delivery System
1.3 Principle of Transdermal Drug Delivery
The stratum corneum acts as the main barrier to drug penetration. Drug permeation occurs via three pathways: transcellular, intercellular, and trans appendageal routes [6]. Only drugs with molecular weight less than 500 Da, adequate lipophilicity, and balanced partition coefficient can easily cross the skin barrier [7]. To enhance absorption, chemical enhancers, physical methods, and nanotechnology-based systems have been introduced [8].
1.5 Limitations of Conventional Patches
Despite advantages, conventional patches have limitations:
1.6 Rationale for Advanced Transdermal Systems
Modern therapeutics increasingly involve biologics, peptides, and vaccines, which cannot be effectively delivered by conventional patches. Advanced methods like microneedles, iontophoresis, sonophoresis, nano-vesicular carriers, and hydrogels are being explored to enhance penetration and broaden the scope of TDDS [18,19].
1.7 Ideal Characteristics of TDDS
An ideal transdermal system should [20]:
The design of transdermal drug delivery systems (TDDS) has evolved significantly over the last three decades. Based on structural design and mechanism of drug release, TDDS can be broadly classified into conventional patches and advanced systems beyond patches [21].
|
Type |
Description |
Examples |
|
Reservoir system |
Drug stored in a liquid/gel reservoir; release controlled by a rate-controlling membrane |
Transderm-Nitro (Nitroglycerin) [22] |
|
Matrix system |
Drug dispersed in a polymeric matrix; drug release occurs by diffusion |
Nitro-Dur, Nicoderm CQ [23] |
|
Drug-in-adhesive system |
Drug incorporated directly in the adhesive layer; no separate reservoir or matrix |
Clonidine patch (Catapres-TTS) [24] |
|
Micro-reservoir system |
Combination of reservoir and matrix systems; drug is present in micro-dispersed reservoirs |
Estraderm (Estradiol) [25] |
|
Microneedle systems |
Arrays of micron-sized needles pierce the stratum corneum to enhance drug permeation |
Insulin delivery, vaccine patches [26] |
|
Iontophoretic systems |
Low-intensity electrical current drives charged drug molecules through the skin |
Iontophoresis of lidocaine [27] |
|
Sonophoretic systems |
Ultrasound waves disrupt lipid bilayers of the stratum corneum, enhancing drug penetration |
Delivery of macromolecules [28] |
|
Vesicular systems |
Nanocarriers like liposomes, niosomes, ethosomes enhance drug penetration |
Diclofenac liposomal gel [29] |
|
Nanoparticle-based patches |
Solid lipid nanoparticles (SLN) or nanostructured lipid carriers (NLC) provide controlled drug delivery |
Tacrolimus-loaded NLC patches [30] |
|
Hydrogel-based patches |
Hydrophilic polymer matrices swell and control drug release |
Lidocaine hydrogel patch [31] |
2.2 Conventional Systems
Conventional transdermal systems include reservoir, matrix, drug-in-adhesive, and micro-reservoir systems. These patches provide controlled release and have been widely commercialized for drugs such as nitroglycerin, nicotine, and estradiol [22,23]. However, they are limited to small, lipophilic, and low-dose drugs [24].
2.3 Advanced Systems Beyond Conventional Patches
Advanced TDDS are designed to overcome the skin barrier and deliver challenging molecules such as peptides, proteins, and vaccines. These include microneedle arrays, iontophoresis, sonophoresis, vesicular carriers, nanoparticle systems, and hydrogels [26–31]. Such technologies allow for higher drug loading, improved bioavailability, and broader therapeutic applications.
Transdermal drug delivery systems (TDDS) have demonstrated broad therapeutic applications in the management of chronic, acute, and preventive therapies. By bypassing the gastrointestinal tract and hepatic first-pass metabolism, TDDS improve drug bioavailability and patient compliance [32].
3.1 Cardiovascular Disorders
3.1.1 Antianginal Therapy
Nitroglycerin patches provide sustained vasodilation, reducing myocardial oxygen demand and preventing angina attacks [33].
3.1.2 Hypertension Management
Clonidine transdermal patches (Catapres-TTS) are widely used for long-term blood pressure control, minimizing fluctuations in plasma levels [34].
3.2.1 Parkinson’s Disease
Rotigotine transdermal systems offer continuous dopaminergic stimulation, reducing motor fluctuations compared to oral therapy [35].
3.2.2 Alzheimer’s Disease
Rivastigmine patches enhance cholinesterase inhibition with lower gastrointestinal side effects than oral dosage forms [36].
3.3 Pain Management
3.3.1 Chronic Pain
Fentanyl patches are gold-standard for cancer-related and postoperative chronic pain, providing long-term analgesia [37].
3.3.2 Local Pain Relief
Lidocaine patches are effective in neuropathic pain and post-herpetic neuralgia, offering site-specific therapy [38].
Estradiol patches are used in menopausal women to reduce vasomotor symptoms, osteoporosis risk, and urogenital atrophy [39]. Combined estrogen-progestin systems help balance hormone therapy safely [40].
3.5 Smoking Cessation
Nicotine patches deliver controlled nicotine levels, reducing withdrawal symptoms and aiding smoking cessation programs [41].
Insulin delivery via microneedle patches represents a promising approach for diabetes management, improving patient compliance over injections [42].
3.7 Vaccination and Immunization
Microneedle patches are being investigated for vaccine delivery against influenza, hepatitis B, and COVID-19, offering advantages such as pain-free administration and reduced need for cold-chain storage [43].
Transdermal patches for antiemetic therapy (e.g., granisetron) reduce chemotherapy-induced nausea and vomiting [44]. Novel systems for hormone therapy in breast and prostate cancer are also under investigation [45].
3.9 Miscellaneous Applications
4. DRUG SELECTION CRITERIA
The success of a Transdermal Drug Delivery System (TDDS) largely relies on the careful selection of a suitable drug candidate, as not all drugs can effectively penetrate the skin barrier to produce the desired therapeutic effect. The skin, particularly the stratum corneum, acts as a strong protective barrier, allowing only molecules with certain physicochemical and pharmacokinetic characteristics to pass through efficiently. For optimal transdermal delivery, the drug should ideally possess a low molecular weight, generally less than 500 Daltons, as larger molecules have difficulty diffusing through the tightly packed lipid layers of the skin. Additionally, the drug must have moderate lipophilicity, allowing it to partition into both the lipid-rich stratum corneum and the aqueous viable epidermis and dermis beneath it. The octanol-water partition coefficient (log P) is a crucial parameter, with an ideal range of 1 to 3, ensuring balanced solubility in both lipids and water for effective permeation. Furthermore, the drug should have a potent pharmacological action, requiring only a small dose (typically less than 10 mg/day), since the amount of drug that can be delivered transdermally is limited by the surface area of the patch and the rate of skin penetration. From a pharmacokinetic perspective, the drug should exhibit short plasma half-life and first-pass metabolism, making transdermal delivery advantageous by providing sustained release and bypassing hepatic metabolism. It should also have a steady and predictable absorption profile to maintain constant plasma drug concentrations, thereby minimizing peak-trough fluctuations often seen with oral or injectable routes. Additionally, the drug must be non-irritating and non-sensitizing to the skin to avoid allergic reactions or local irritation, ensuring patient compliance with long-term use. Drugs such as nitroglycerin, clonidine, estradiol, nicotine, and fentanyl are successful examples that meet these criteria and are widely available in marketed transdermal systems. Therefore, thorough evaluation of drug properties during the formulation design phase is critical, as selecting an inappropriate drug candidate can lead to poor skin permeation, sub-therapeutic drug levels, and ultimately, failure of the transdermal system [49].
4.1.1 Molecular Weight
Drugs intended for TDDS should ideally have a molecular weight less than 500 Daltons to cross the stratum corneum effectively [50].
4.1.2 Lipophilicity
Moderately lipophilic drugs (log P between 1–3) are suitable, as they must partition into both the stratum corneum and aqueous layers of the epidermis [51].
4.1.3 Solubility
A balance of aqueous and lipid solubility is required to ensure drug transport through the lipid-rich skin layers and into systemic circulation [52].
4.1.4 Potency
Since TDDS can deliver only limited drug quantities per unit area, the selected drug should be potent at low doses (≤10 mg/day) [53].
4.2.1 Half-life
Drugs with short biological half-lives are preferred for TDDS to maintain steady plasma concentrations over prolonged periods [54].
4.2.2 Oral Bioavailability
Drugs undergoing extensive first-pass metabolism (e.g., nitroglycerin, estradiol) are ideal candidates, as TDDS bypasses hepatic metabolism [55].
4.2.3 Therapeutic Index
Drugs with a narrow therapeutic index may be unsuitable due to variations in skin permeability, which could lead to dose fluctuations [56].
4.3 Clinical Suitability
5. COMPOSITION / EXCIPIENT

Fig 2. Transdermal drug delivery systems (TDDS) beyond conventional Patches
A transdermal drug delivery system (TDDS) is a complex, multi-layered structure composed of several components that work synergistically to ensure drug stability, skin permeation, and therapeutic efficacy [61]. Each excipient has a unique role in determining drug release kinetics, adhesion, patient compliance, and product stability.
Polymers form the backbone of most transdermal systems, controlling drug release rate and providing mechanical strength.
Examples: Ethyl cellulose, Eudragit, Hydroxypropyl methylcellulose (HPMC), Polyvinylpyrrolidone (PVP), Polyisobutylene [62].
Function: Control release kinetics, provide flexibility, prevent drug crystallization.
The active pharmaceutical ingredient (API) is incorporated into the system depending on solubility, potency, and compatibility with excipients.
Examples: Nitroglycerin, Fentanyl, Estradiol, Nicotine [63].
Adhesives are critical for ensuring intimate contact of the patch with the skin throughout the application period.
Examples: Polyacrylates, Silicone-based adhesives, Polyisobutylene [64].
Function: Secure adhesion, allow drug release, minimize skin irritation.
Enhancers temporarily modify the skin barrier to improve drug permeability.
Examples: Oleic acid, Propylene glycol, Dimethyl sulfoxide (DMSO), Terpenes [65].
Function: Disrupt stratum corneum lipids, increase diffusion coefficient, enhance drug flux.
Plasticizers improve flexibility, reduce brittleness of polymer films, and enhance patient comfort.
Examples: Dibutyl phthalate, Triethyl citrate, Glycerol [66].
The impermeable backing membrane protects the drug reservoir from environmental exposure (moisture, oxygen) and prevents drug loss.
Examples: Polyethylene terephthalate (PET), Aluminum foil laminate, Polyvinyl chloride (PVC) [67].
A release liner is a temporary protective cover that prevents drug loss during storage and is removed before application.
Examples: Polyester films, Siliconized paper [68].
In reservoir-type patches, a membrane regulates drug release at a predetermined rate.
Examples: Ethylene-vinyl acetate copolymer (EVA), Cellulose acetate [69].
These prevent drug degradation caused by light, heat, or oxidation.
Examples: Butylated hydroxytoluene (BHT), Butylated hydroxyanisole (BHA), Tocopherol [70].
Solvents aid in solubilizing drugs and polymers, while co-solvents improve penetration.
Examples: Ethanol, Isopropanol, PEG 400 [71].
|
Component |
Examples |
Function |
|
Polymer matrix |
HPMC, PVP, Eudragit |
Provides structural integrity and controls drug release |
|
Adhesive |
Silicone, Polyisobutylene, Polyacrylate |
Ensures proper skin adhesion |
|
Penetration enhancer |
Oleic acid, DMSO, Propylene glycol |
Enhances drug permeation through the skin |
|
Plasticizer |
Triethyl citrate, Glycerol |
Improves flexibility and mechanical strength |
|
Backing layer |
PET film, Aluminum foil laminate |
Protects the patch from environmental factors |
|
Release liner |
Siliconized polyester film |
Protects the patch during storage before use |
|
Antioxidants |
BHT, Tocopherol |
Prevents oxidation and improves stability |
Manufacturing of transdermal drug delivery systems (TDDS) requires careful selection of polymers, adhesives, and penetration enhancers, followed by controlled processing techniques to ensure reproducibility, drug stability, and consistent release profiles [72]. The choice of manufacturing method depends on the type of patch (matrix, reservoir, drug-in-adhesive, or micro-reservoir) and the physicochemical properties of the drug.
6.1 Methods for Matrix-Type Systems
6.1.1 Solvent Evaporation Method
Drug and polymer are dissolved in a volatile solvent (e.g., chloroform, ethanol).
The solution is cast onto a backing membrane and dried under controlled conditions.
Solvent evaporation leaves behind a thin drug-loaded polymeric film [73].
Advantage: Simple and suitable for heat-sensitive drugs.
Disadvantage: Possible residual solvent toxicity.
6.1.2 Melt Extrusion Method
Drug and polymer are mixed and melted at controlled temperature.
The molten mixture is extruded into thin films.
No solvents are used [74].
Advantage: Solvent-free, continuous process.
Disadvantage: Not suitable for thermolabile drugs.
6.2 Methods for Reservoir-Type Systems
6.2.1 Membrane-Laminated System
Drug reservoir is prepared as a liquid/gel.
Reservoir is enclosed between a backing layer and a rate-controlling membrane.
Adhesive layer is applied to the external surface [75].
Advantage: Provides zero-order drug release.
Disadvantage: Complex and costly.
6.3.1 Direct Incorporation Method
Drug is directly dispersed or dissolved in the adhesive polymer.
The mixture is coated uniformly on a release liner and dried.
Backing layer is then laminated [76].
Advantage: Thin and elegant patches.
Disadvantage: Limited drug loading.
Drug is suspended in an aqueous solution, then dispersed in a lipophilic polymer.
Mechanical dispersion forms micro-sized reservoirs.
Film is cast and laminated with a backing layer [77].
Advantage: Combines properties of reservoir and matrix systems.
Disadvantage: Technically complex.
6.5 Novel Manufacturing Approaches
6.5.1 Microneedle Fabrication
Made using lithography, laser cutting, or 3D printing.
Arrays are coated or filled with drug formulations [78].
6.5.2 Nanocarrier-Loaded Patches
Nanoparticles, liposomes, or ethosomes are embedded into polymer matrices.
Provide sustained and enhanced drug penetration [79].
6.5.3 Pressure-Sensitive Adhesive Coating
Modern roll-to-roll coating techniques are used for large-scale adhesive patch manufacturing.
Ensures uniform thickness and reproducibility [80].
Drug–polymer compatibility (avoiding crystallization).
Moisture and temperature control during drying and lamination.
Uniform thickness of films for dose accuracy.
Scalability and reproducibility of process for commercial production [81].
7. EVALUATION OF TRANSDERMAL DRUG DELIVERY SYSTEMS
Evaluation of transdermal drug delivery systems (TDDS) is essential to ensure safety, efficacy, uniformity, and patient acceptability. Both in vitro and in vivo tests are performed to characterize the mechanical, physicochemical, and pharmacokinetic properties of patches [82].
7.1 Physicochemical Evaluation
7.1.1 Thickness and Weight Variation
7.1.2 Drug Content Uniformity
7.1.3 Moisture Content and Uptake
7.1.4 Folding Endurance
7.2 Mechanical and Adhesion Properties
7.2.1 Tensile Strength
7.2.2 Peel Adhesion Test
7.2.3 Tack Test
7.3 In Vitro Drug Release Studies
7.4 Ex Vivo Permeation Studies
7.5 In Vivo Evaluation
7.5.1 Pharmacokinetic Studies
7.5.2 Pharmacodynamic Studies
7.5.3 Skin Irritation and Sensitization Tests
7.6 Stability Studies
7.7 Advanced Evaluation Techniques
8. RESULT & DISCUSSION
The evaluation of transdermal drug delivery systems (TDDS) has been extensively reported in the literature, and numerous comparative studies demonstrate their advantages over conventional dosage forms. This section summarizes the key outcomes from previously published research, focusing on drug permeation, pharmacokinetics, patient compliance, and therapeutic success.
8.1 Drug Permeation and Skin Barrier Modulation
Several studies have confirmed that the stratum corneum remains the major barrier for drug penetration. Chemical enhancers such as oleic acid and propylene glycol increased drug flux significantly compared to placebo patches [99]. Furthermore, physical techniques such as iontophoresis and microneedles were shown to enhance delivery of peptides, insulin, and vaccines, which are otherwise unsuitable for passive diffusion [100].
8.2 Pharmacokinetic Profiles
Conventional oral dosage forms often result in fluctuating plasma levels, leading to peaks and troughs. In contrast, TDDS provide steady plasma concentrations. For instance, fentanyl patches maintained consistent analgesic levels for 72 hours, reducing breakthrough pain episodes compared to oral opioids [101]. Rivastigmine patches demonstrated lower gastrointestinal side effects and improved adherence compared to oral capsules [102].
8.3 Patient Compliance and Acceptance
Clinical trials suggest that patient preference for patches is higher due to painless, non-invasive administration and reduced dosing frequency [103]. In smoking cessation programs, nicotine patch users reported higher compliance compared to gum or lozenge users [104]. Similarly, Parkinson’s patients preferred rotigotine patches due to ease of application and 24-hour symptom control [105].
8.4 Comparative Effectiveness of Advanced Systems
Advanced systems have shown superiority over conventional patches:
8.5 Safety and Tolerability
Most patches were reported to be safe; however, mild erythema and skin irritation were occasionally observed, especially with chemical enhancers [109]. Novel hydrogel-based patches were found to minimize irritation by maintaining hydration at the site of application [110].
8.6 Discussion and Future Perspective
From the reviewed studies, it is evident that TDDS provide substantial advantages over conventional formulations in terms of controlled release, bioavailability, and patient compliance. While conventional patches are successful for small, lipophilic drugs, advanced technologies are expanding the scope to include biologics, macromolecules, and vaccines.
Future research should focus on:
9. MARKETED EXAMPLES
Several transdermal patches are available commercially, offering sustained and controlled drug delivery. These marketed formulations highlight the practical success of TDDS in diverse therapeutic areas [111].
9.1 Examples of Marketed Transdermal Patches
|
Brand |
Drug |
Use |
Strength |
Cost (USD) |
Ref |
|
Nitro-Dur |
Nitroglycerin |
Angina |
0.1 – 0.8 mg/hr |
20 – 40 |
[112] |
|
Catapres-TTS |
Clonidine |
Hypertension |
0.1 – 0.3 mg/day |
35 – 50 |
[113] |
|
Duragesic |
Fentanyl |
Chronic pain |
12 – 100 mcg/hr |
50 – 200 |
[114] |
|
Nicoderm CQ |
Nicotine |
Smoking cessation |
7 – 21 mg/24 hr |
40 – 60 |
[115] |
|
Exelon |
Rivastigmine |
Alzheimer’s |
4.6 – 9.5 mg/24 hr |
150 – 200 |
[116] |
|
Neupro |
Rotigotine |
Parkinson’s |
2 – 8 mg/24 hr |
180 – 250 |
[117] |
|
Climara |
Estradiol |
HRT (Hormone Replacement Therapy) |
0.025 – 0.1 mg/day |
80 – 120 |
[118] |
|
Ortho Evra |
Ethinylestradiol + Norelgestromin |
Contraception |
20 µg + 150 µg/24 hr |
70 – 100 |
[119] |
|
Transderm-Scop |
Scopolamine |
Motion sickness |
1.5 mg/72 hr |
25 – 40 |
[120] |
|
BuTrans |
Buprenorphine |
Pain, Opioid dep. |
5 – 20 mcg/hr |
100 – 150 |
[121] |
9.2 Key Observations
10. RECENT RESEARCH / ADVANCES
In recent years, there has been remarkable progress in the development of next-generation Transdermal Drug Delivery Systems (TDDS), driven by the need to overcome the inherent limitations of conventional patches and expand their application beyond small, lipophilic drug molecules. Traditional TDDS are often restricted by the skin’s barrier function, particularly the stratum corneum, which significantly limits the penetration of large and hydrophilic molecules. To address this challenge, modern research has focused on innovative technologies that facilitate the delivery of peptides, proteins, vaccines, nucleic acids, and other biologics, which were previously unsuitable for transdermal administration. These advancements integrate nanotechnology, physical enhancement methods, and smart materials to achieve precise, controlled, and patient-friendly drug delivery.
Nanotechnology-based approaches have introduced nanocarriers such as liposomes, niosomes, transfersomes, ethosomes, solid lipid nanoparticles (SLNs), and nanostructured lipid carriers (NLCs) that can encapsulate large or sensitive molecules, protecting them from degradation while enhancing their permeation through the skin’s layers. These carriers not only improve drug stability but also allow sustained and targeted release, reducing dosing frequency and improving therapeutic outcomes. In parallel, physical enhancement techniques have been developed to actively disrupt the stratum corneum or create microchannels for drug entry. Among these, microneedle arrays have gained significant attention, as they painlessly pierce the outermost layer of the skin, enabling efficient and minimally invasive delivery of macromolecules like insulin, growth hormones, and vaccines. Other physical methods such as iontophoresis, which uses mild electrical currents to drive charged drug molecules, and sonophoresis, which applies ultrasound waves to temporarily disrupt lipid bilayers, have also shown promising results in enhancing transdermal transport.
Moreover, the introduction of smart materials has revolutionized TDDS by enabling responsive and controlled drug release. These materials are designed to react to external stimuli such as temperature, pH, light, or mechanical pressure, releasing the drug only when needed, thereby mimicking physiological conditions and improving therapeutic precision. For example, temperature-sensitive hydrogels can release insulin in response to elevated glucose levels, offering a novel approach to diabetes management. Similarly, pH-responsive patches are being explored for wound healing applications and targeted cancer therapy. The integration of wearable electronic sensors with TDDS has also opened the door for real-time monitoring and feedback, allowing personalized medicine and dosage adjustments based on patient-specific needs.
Collectively, these next-generation systems represent a significant leap forward in drug delivery science, providing solutions for challenges such as poor skin permeability, variable absorption rates, and patient non-compliance. By combining nanocarriers for drug protection and penetration, physical enhancers for barrier disruption, and smart materials for precision control, researchers are creating TDDS that are not only more efficient but also more versatile. These cutting-edge technologies hold immense potential for delivering complex biological drugs, enabling non-invasive, sustained, and targeted therapies for chronic diseases, cancer, and immunization programs. As a result, the future of TDDS lies in these multifunctional, intelligent systems, which are expected to transform how medications are administered, offering safer, more convenient, and highly effective alternatives to traditional oral and injectable routes [122].
10.1 Microneedle Technology
Microneedles (MNs) are arrays of micron-sized needles that painlessly create microchannels in the stratum corneum.
10.2 Iontophoresis and Electroporation
10.3 Sonophoresis and Ultrasound-Mediated Delivery
Ultrasound waves disrupt the lipid structure of the stratum corneum, enhancing penetration.
10.4 Vesicular and Nanocarrier Systems
10.5 Hydrogel and Smart Patches
Hydrogels provide controlled hydration, enhanced comfort, and sustained release.
10.6 Vaccine Delivery
Microneedle-based patches for COVID-19, influenza, and hepatitis B vaccines have shown promising immunogenicity with reduced need for cold-chain logistics [132].
10.7 Biodegradable and Eco-Friendly Systems
Research focuses on biodegradable polymers (e.g., chitosan, PLGA) to reduce environmental burden. These materials provide safe degradation and minimize patch disposal concerns [133].
10.8 Future Directions
CONCLUSION
Transdermal drug delivery systems represent a revolutionary advancement in pharmaceutical technology by offering controlled, non-invasive, and patient-friendly drug administration. Conventional patches have established their role in cardiovascular, pain, neurological, and hormonal therapies, while recent advances such as microneedles, nanocarriers, and smart patches are expanding applications to biologics, vaccines, and personalized medicine. Despite limitations like skin barrier resistance and local irritation, ongoing research continues to address these challenges with novel approaches such as iontophoresis, ultrasound-mediated delivery, and biodegradable materials. The future of TDDS lies in next-generation intelligent patches that can monitor physiological signals and release drugs accordingly, thereby achieving precision medicine.In conclusion, transdermal systems, particularly beyond conventional patches, have demonstrated immense potential to transform therapeutic outcomes, improve compliance, and broaden the scope of modern drug delivery.
REFERENCES


Shraddha Sanap, Pratik Bhabad, Transdermal Drug Delivery: Beyond Conventional Patches, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 4214-4234. https://doi.org/10.5281/zenodo.18108044
 10.5281/zenodo.18108044
10.5281/zenodo.18108044
