1,2Dr. Vedprakash Patil Pharmacy College, Gevrai Tanda, Paithan Rd, Aurangabad, Maharashtra (INDIA)- 431 002
Dr. Babasaheb Ambedkar Technological University Lonere, Raigad-402 103
This research is focuses on the formulation and evaluation of mucoadhesive buccal patches containing Deflazacort, a synthetic glucocorticoid with potent anti-inflammatory and immunosuppressive properties. Deflazacort is used in the treatment of various inflammatory and autoimmune conditions, including rheumatoid arthritis, asthma, and inflammatory bowel disease. However, its clinical efficacy is limited by the necessity for frequent dosing, systemic side effects, and poor patient compliance. The Buccal patches of Deflazacort was formulated by solvent casting method using mucoadhesive polymer Hydroxy Propyl Methylcellulose and Ethyl cellulose. Total nine batches with different concentrations of HPMC and EC was formulated. The formulated batches were evaluated for its thickness, weight variation, drug content uniformity, and surface morphology etc. In vitro studies are conducted to investigate the mucoadhesive strength, swelling behaviour, and drug release profile of the patches using simulated saliva as the dissolution medium. The percent release of buccal patches was found in the range of 83.74± 0.2% to 97.67± 0.2%. Batch 2 was found to be most suitable due to the maximum drug release. Furthermore, in vitro permeation of Deflazacort of B2 were studied % Cumulative Deflazacort permeated in 24 hrs was up to 62.47± 0.2%. Stability study of Mucoadhesive buccal patches also carried out which states that, the buccal patches were found to be stable for the period of 3 months. This research holds promise for the development of alternative dosage forms for Deflazacort therapy, catering to the needs of patients with inflammatory conditions requiring targeted drug delivery via the buccal route.
In recent years, mucoadhesive drug delivery systems have garnered significant attention in pharmaceutical research due to their potential to enhance drug bioavailability and therapeutic outcomes. These systems, designed to adhere to the mucosal surfaces of the body, offer a localized and targeted approach to drug administration. Among the various forms of mucoadhesive drug delivery, buccal patches have emerged as a particularly promising strategy. Buccal patches deliver drugs directly through the mucosal membrane of the oral cavity, bypassing the gastrointestinal tract and hepatic first-pass metabolism. This not only enhances the bioavailability of the drug but also allows for controlled and sustained drug release, which can lead to prolonged therapeutic effects. Furthermore, buccal patches are non-invasive and user-friendly, offering a convenient and comfortable option for patients, which in turn promotes better adherence to treatment regimens. Deflazacort, a potent glucocorticoid known for its anti-inflammatory and immunosuppressive properties, is frequently prescribed in the treatment of a variety of chronic inflammatory diseases such as rheumatoid arthritis, Duchenne muscular dystrophy, and asthma. Despite its clinical efficacy, deflazacort’s conventional oral administration is often hindered by significant drawbacks, including low and variable bioavailability due to extensive first-pass metabolism in the liver. Additionally, long-term systemic exposure to glucocorticoids like deflazacort can lead to adverse side effects, such as bone density loss, glucose intolerance, and increased susceptibility to infections. As a result, there is a critical need to explore alternative drug delivery systems that can enhance deflazacort’s therapeutic effectiveness while minimizing its systemic side effects.1
This research focuses on the formulation and evaluation of mucoadhesive buccal patches as a novel drug delivery system for deflazacort. The central goal of this study is to develop a buccal patch capable of adhering to the mucosal surface of the mouth, providing sustained and controlled release of deflazacort over a prolonged period. This localized delivery system is expected to reduce systemic exposure, mitigate side effects, and improve patient outcomes. Various formulation parameters, including polymer selection, drug loading capacity, and mucoadhesive properties, will be optimized to enhance both the therapeutic efficacy and patient comfort of the buccal patches.
The evaluation process will encompass in-vitro studies to comprehensively assess the performance of the formulated patches. Key evaluation metrics will include drug release profiles, the strength and duration of mucoadhesion, patch stability, and pharmacokinetic behaviour. These assessments will provide valuable insights into the potential of mucoadhesive buccal patches as a viable and efficient alternative for the delivery of deflazacort.2 By exploring this innovative approach to drug delivery, this research aims to contribute to the development of safer and more effective therapeutic strategies for patients requiring long-term deflazacort treatment. The successful formulation of mucoadhesive buccal patches could not only improve the bioavailability of deflazacort but also represent a significant advancement in the field of non-invasive drug delivery systems.
MATERIAL AND METHOD
MATERIALS
Deflazacort (DFC), the active pharmaceutical ingredient, was obtained as a gift sample from Anuh Pharma Ltd., Mumbai. Hydroxypropyl methyl cellulose (HPMC), utilized as a sustained release polymer, and ethyl cellulose, employed as a mucoadhesive polymer, were sourced from Dipa Chemical Industries. Glycerol, also supplied by Dipa Chemical Industries, served as the plasticizer in the formulation. Methanol and chloroform, which functioned as solvents during the preparation process, were also procured from Dipa Chemical Industries.
METHODS:
Characterization of Drug
Melting behaviour
Melting point of Deflazacort (DFC) was determined using automated melting point apparatus OptiMelt (SRS).3
UV spectroscopy
A UV spectrum of Deflazacort was recorded in Methanol using ‘Spectrum Measurement’ function of UV-Visible Spectrophotometer (Lasany)4
Vibrational spectroscopic study
After starting the instrument, ‘Background Measurement’ was performed without placing the drug on panel. For ‘Sample Measurement’, pure Deflazacort was placed on cleaned panel of FT-IR Spectrometer (Bruker). The placed Deflazacort was sandwiched between panel and upper arm. This sample was scanned over a wave number range of 4000 to 400 cm-1.5
Construction of calibration curve for Deflazacort
Preparation of Stock Solution
Standard solution was prepared by accurately weighed 100 mg of Deflazacort working standard into a 100 ml volumetric flask, added 40 ml of MeOH, shake and sonicated to dissolve the content, made up the volume with MeOH. and filtered through 0.45-micron membrane filter. The solution was further diluted with water to obtain the required concentration of standard solution (20-100 µg/ml).6
Determination of Analytical Wavelength (?max)
The standard solution of Deflazacort was scanned in the wavelength range of 200-400 nm on a UV-Visible Spectrophotometer from this, wavelength corresponding to maximum absorbance (? max) was found to be 244 nm.7
Preparation of Standard curve
A six point standard curve of Deflazacort was prepared using different concentrations. The concentration range selected was from 20 µg/mL to 100 µg/mL. Concentrations of 20 µg/mL, 40 µg/mL, 60 µg/mL, 80 µg/mL and 100 µg/mL, were prepared by appropriate dilutions of Stock-1.8
Preparation of Preliminary Batches of Buccal Patches
The preliminary batches of Buccal Patches were tried on the basis of previous reports. These batches were prepared and evaluated for optimizing the formulation components like amount and ratio of polymers and concentration of plasticizer.9
Method of preparation of Mucoadhesive Buccal patches Deflazacort:
The mucoadhesive buccal patches of deflazacort were prepared using the solvent casting method. The formulation involved varying ratios of hydroxypropyl methylcellulose (HPMC), ethyl cellulose (EC), and glycerol as the plasticizer. Glass rings with an inner diameter of 5.3 cm were placed on a glass slab to shape the patches, while a mixture of chloroform (CHL) and methanol (MeOH) served as solvents.
The process began with the accurate weighing of the drug and polymers using an analytical balance. Next, the solvent mixture was prepared by measuring and mixing the CHL and MeOH in specific ratios. This solvent mixture was then used to dissolve both the drug and the polymers. In separate beakers, the accurately weighed polymers (a total of 1000 mg) were dissolved in the solvent mixture, with HPMC being added slowly and stirred continuously to prevent lumps. Since the ethyl cellulose solution was less viscous than that of HPMC, it was gradually combined with the HPMC solution under continuous stirring until a homogeneous mass was achieved.
The deflazacort was dissolved in a small volume of methanol, and this drug solution was added to the polymeric mixture, with continuous stirring to ensure even distribution of the drug within the viscous polymer solution. The plasticizer, glycerol, was then weighed and added to the mixture along with the remaining solvent, further stirred to form a homogeneous, clear, and viscous mass.10-12 This mixture was carefully poured into the glass rings on the glass slab to maintain uniform thickness. The patches were allowed to dry at room temperature for 24 hours. To ensure controlled evaporation, an inverted funnel was placed over the rings. Once the solvent had fully evaporated, the patches were carefully removed and cut into uniform squares. The dried patches were stored in self-sealing polythene bags with butter paper between each patch to prevent sticking, and the bags were placed in a desiccator until further use.13
Formulation development of Buccal Patches Deflazacort:
Formulation of Mucoadhesive Buccal patches of Deflazacort were developed by using change in the critical formulation parameters.

Table 1: Batch size for DFZ Mucoadhesive Buccal patches
Evaluation of Mucoadhesive buccal Patches of Deflazacort:
The evaluation of mucoadhesive buccal patches of deflazacort is crucial to ensure their clinical efficacy and patient compliance, as these patches deliver a controlled, smaller dose of the drug at a predetermined rate. Evaluation studies help predict the performance and consistency of the patches under specific environmental conditions. These evaluations are typically classified into two categories:14-16
Physicochemical evaluation:17-20
Physical Appearance
The appearance of the preparaed Mucoadhesive buccal patch of Deflazacort was observed physically.
Thickness
The thickness of mucoadhesive buccal patch was determined using screw gauge. The thickness of patch was measured at five different points of patch (4 at corners and 1at centre). The average of these five readings was calculated and reported as thickness ± SD in millimetres.
Uniformity of weight
The prepared patches were studied for weight variation by individually weighing 10 randomly selected patches and calculating the average weight. The individual weight should not deviate significantly from the average weight. Lesser the deviation more is the uniformity.
Drug content determination
A 50 mg portion of patch was weighed accurately and dissolved in 3mL of MeOH in a 10 mL beaker. It was shaken slowly to ensure complete immersion of patch portion into the solvent. This was sonicated for 2 minutes. After sonication, an accurate volume of resultant solution (1mL) was taken out by micropipette and transferred to 5mL volumetric flask. The volume was made up to 5mL using MeOH. The amount of drug was then estimated by UV spectrophotometer method at 244 nm and % drug content was reported.
Tensile strength determination
In this test, the prepared patch was cut in the shape of rectangle. The two ends of it were tied separately to corked linear iron plates. One end of this was kept fixed by tying it the firm base, and other end was connected to a freely movable thread over a pulley. The weights were added to pan in gradually increasing manner. This pan was attached with the hanging end of the thread over that pulley. A pointer on the thread was observed to measure and note the elongation of the film. The weight just sufficient to break the patch was noted. The tensile strength can be calculated using the following equation:
Tensile strength = Fa×b × (1+Ll)
Where F = force required to break the patch (N/cm2)
a = width of patch used (cm)
b = thickness of patch used (cm)
L = length of patch used (cm)
l = elongation of patch at break point (cm)
Folding endurance
The folding endurance of the patch is the number of times that patch could be folded at the same place without breaking it. Folding capacity of the patch was determined in this test. In this test, the selected portion of patch was folded repeatedly at the same place until it breaks. The number of folds required to break the patch, was reported as its folding endurance.
Flatness
To determine the flatness of a patch, a strip was cut from the centre and two from each side of patch. The length of each strip was measured and variation in length was noted. This data was used to determine percent constriction and results were shown in the form of % flatness. 0 % constriction indicates 100 % flatness.
It is calculated from following formula:
% constriction = L1- L2L1 × 100
Where L1= Initial length of strip (cm)
L2= Final length of strip (cm)
Muco-adhesive strength of patch
The mucoadhesive strength of the patch was measured using goat buccal mucosa, obtained from a local slaughterhouse and used within 2 hours. The mucosa was cut into a 3 cm piece, washed with phosphate buffer (pH 6.8), and attached to an inverted 50 ml container placed in the center of a 250 ml beaker containing the same buffer. The patch was affixed to the underside of a glass vial using cyanoacrylate glue. The setup was balanced with a 5 g weight, which was then removed to bring the patch into contact with the mucosa for a 5-minute contact time. Water was gradually added at a rate of 100 drops per minute until the patch detached from the mucosal surface. The weight in grams required to separate the patch indicated the mucoadhesive strength.
Percentage of moisture content
For this test, one patch from each batch was selected and weighed accurately (W1 mg). These weighed patches were kept in a desiccator containing Calcium chloride at room temperature for 24 hours. After the specified interval, patches were weighed again until a constant weight was obtained (W2 mg). The percent moisture content was calculated using following formula:
% Moisture content = W1- W2W1 × 100
Percentage of moisture uptake
Patches were selected from each batch and weighed accurately (W1 mg). These patches were kept in dessicator at room temperature for 24 hours. Then patches were taken out and exposed to 84% relative humidity using a saturate solution of Potassium chloride in another dessicator. Exposure was continued until a constant weight (W2 mg) was obtained. The percent moisture uptake was calculated using following formula:
% Moisture uptake=W2- W1W2 × 100
Differential Scanning Colorimetry (DSC)
Thermal behaviour of the deflazacort was studied using differential scanning calorimeter. The small quantity of sample was crimped between the aluminium pans using hydraulic press. The pans were heated at the rate of 5°C/min from 0 to 300 °C in the presence of nitrogen gas.
In vitro evaluation
In vitro dissolution studies
The in vitro drug discharge investigation of Delazacort buccal patch through the cellophone membrane was performed utilizing a Franz diffusion cell at 37.0±0.5°C. the cellophone layer was mounted between the contributor and receptor compartments. The patch was put on the cellophone membrane, and the compartments were braced together. The benefactor compartment was loaded up with 1 ml of phosphate buffer (pH 6.8). The receptor compartment was loaded up with 200 ml phosphate cradle (pH 6.8), and the hydrodynamics in the receptor compartment were kept up with by blending with an attractive beed at 50 rpm. At foreordained time stretches, 1 ml test was removed with timepoint of 0.25, 0.5, 1, 2, 4, 6, 8 hrs. and supplanted with new medium and absorbance of the examples were estimated at 244 nm, and the total dissolution release was determined. The examinations were performed for each formed clump.21-22
In-vitro skin permeation studies
In-vitro skin permeation studies across chicken skin were conducted using a Franz diffusion cell with a 10 mL receiver compartment. The diffusion cells were mounted on a magnetic stirrer, and the chicken skin was pre-equilibrated with phosphate buffer (0.01M, pH 7.4) for 2 hours. The full-thickness skin was placed in the cell with the stratum corneum facing the donor compartment. The receptor medium was stirred continuously at 37°C to maintain constant conditions. A blank sample was taken to ensure no residual absorbance at 244 nm. The patch was then adhered to the skin, and 1 mL samples were collected at intervals of 1, 2, 4, 6, 8, 10, 12, and 24 hours. Fresh buffer replaced the withdrawn volume each time. The samples were analyzed using UV spectrophotometry at 244 nm to calculate the amount of drug permeated per square centimetre at each time point.23-24
Stability study of Mucoadhesive buccal patch of Deflazacort
The Stability study of mucoadhesive buccal patch were stored in amber coloured glass bottles at 3 different temperatures 4 oC, Room temperature and 40±0.5 oC for a period of 3 months. The samples were withdrawn after 30, 60 and 90 days and analyzed for physical appearance, drug content, folding endurance.25-26
RESULTS AND DISCUSSION:
Characterization of Drug:
Melting behaviour
The melting range of Deflazacort was found to be 252°-258°C by OptiMelt.
Vibrational spectroscopic study
The spectrum of Deflazacort was recorded Structural assignments for the characteristics absorption bands in the spectrum are listed in Table 2.

Table 2: Assignments for the principle FT-IR absorbance bands of Deflazacort
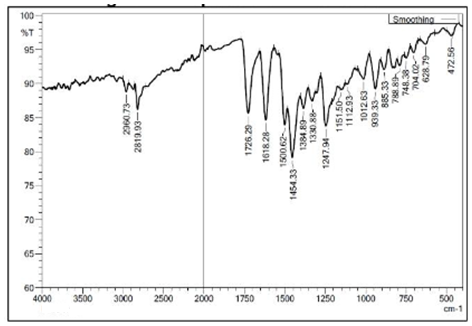
Figure 1: FTIR Spectrum of Deflazacort
Initially, the drug was characterized by its melting behavior and FT-IR spectroscopic studies. The melting range of Deflazacort matched with that of standard range, indicating the drug was in its pure form and was not degraded. FT-IR spectrum of Deflazacort showed the prominent peaks at the wavelengths (cm-1) 1726.29, 2960.73, 1618.28, 1112.93. These peaks appeared for the C=O (Ketone); C-H (Alkane); C=C (Conjugated System); C-O (Ether) respectively. These functional groups matched with the groups in the structure of Deflazacort, hence confirming the functional groups in the structure.
Drug –Excipients Compatibility study
Deflazacort and HPMC

Table 3: Assignments for the principle FT-IR absorbance bands of Deflazacort with HPMC

Figure 2: FTIR Spectrum of Deflazacort with HPMC
Deflazacort and Ethyl Cellulose

Table 4: Assignments for the principle FT-IR absorbance bands of Deflazacort with Ethyl Cellulose

Figure 3: FT-IR Spectrum of Deflazacort with Ethyl Cellulose
Construction of calibration curve for Deflazacort
Maximum Wavelength for Deflazacort was found to be 244 nm. The standard calibration curve of Deflazacort was obtained by plotting the absorbance of the standard solution against its concentration at 244 nm. The standard solution of Deflazacort showed the linear curve with correlation coefficient of 0.9991. Their equations of lines were y = 0.0099x – 0.0317 at selected ?max. Following table 5 shows absorbance of respective standard solution. The standard curve for Deflazacort at 244 nm.

Table 5: Calibration range for Deflazacort

Figure 4: Standard curve for Deflazacort
Although a pre-validated UV method was used for the analysis, ?max for Deflazacort was confirmed by scanning standard solution of Deflazacort. ?max was found to be 244 nm. The calibration curve was developed in the concentration range of 20-100 µg/mL. The solvent used for the calibration curve development was MeOH. The method was found to be linear (R2 =0.9991). R2 near 1 gave the confidence that standard solutions of Deflazacort follow the Beer-Lambert Law.
Evaluation of Mucoadhesive buccal patch for Deflazacort
Physicochemical evaluation
Physical appearance
All prepared Mucoadhesive buccal patch have good appearance with smooth surface. Films prepared were semi-transparent. Surface texture was smooth and uniform.

Figure 5: Mucoadhesive Buccal Patches of Deflazacort
Thickness evaluation of Mucoadhesive buccal patch
The average thickness of transdermal patches is shown in following table 6.

Table 6: Average thickness of Mucoadhesive buccal patch
* All values are mean±SD (n=3)
Uniformity of weight
A good weight uniformity of all formulation indicates an even distribution of drug and the polymers in the patch prepared by solvent evaporation technique. It was also accounted that weight and thickness of patch were increasing with increasing polymer concentration. The average weight of prepared Mucoadhesive buccal patch is shown in following table 7.

Table 7: Uniformity of weight of Mucoadhesive buccal patch
* All values are mean±SD (n=3)
Drug content determination
The prepared 9 batches were tested for their drug content. From results, it was found that the calculated drug loading obtained from the drug content test yielded a satisfactory result ranging from 86.32 ±0.5 % to 98.12 ±0.4 % of the theoretical drug distribution. The % drug content of prepared patches is shown in following table 8.
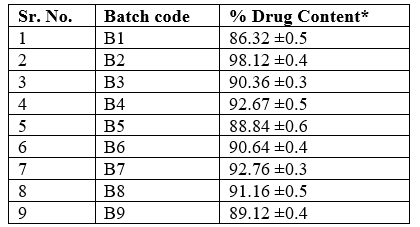
Table 8: Percent Drug content of Mucoadhesive buccal patch
* All values are mean±SD (n=3)
Tensile strength determination
Adequate tensile strength is essential for patches to maintain integrity under stretching conditions, with the amount of plasticizer playing a crucial role. The tensile strength of the transdermal patches ranged from 2.18 ± 0.4 to 4.63 ± 0.2 kg/cm?2;, with batch B2 exhibiting the highest tensile strength and batch B4 the lowest. An increase in plasticizer and HPMC content in the formulation correlated with increased tensile strength. The tensile strength data for the mucoadhesive buccal patches are presented in the table below.

Table 9: Tensile strength of Mucoadhesive buccal patch
* All values are mean±SD (n=3)
Folding endurance test for Mucoadhesive buccal patch
Folding endurance is parameter to measure the ability of transdermal patch to withstand the conditions of folding when it is applied to skin. If patch withstand these conditions and does not break, then burst release can be avoided. Folding endurance of transdermal patch was found to be increase with increasing concentration of plasticizer. The number of folds required to break the patch is shown in following table, with respective batches.

Table 10: Folding endurance of Mucoadhesive buccal patch
* All values are mean±SD (n=3)
Flatness of Mucoadhesive buccal patch
The prerequisite for Mucoadhesive buccal patch is that it should have smooth surface and it should not constrict with time. Flatness study shows whether the transdermal patch fulfils above expectations or not. The flatness study showed that all the formulations had the same strip length before and after their cuts, indicating 100% flatness. Percent constriction with respective % flatness of film is shown in table below.

Table 11: Flatness of Mucoadhesive buccal patch
Muco-adhesive strength of patch
The Muco-adhesive strength of Deflazacort Buccal patch for every batch were evaluated. The muco-adhesive strengths of all batches were found to be in the range of 4.23±0.31 gm to 7.86±0.76 gm respectively. As a result, shows that an increasing in muco-adhesive polymers concentration increases the viscosity of the buccal patches hence increases muco-adhesive strength of patches.

Table 12: Muco-adhesive strength of Deflazacort Buccal patch
Percentage of moisture content
Moisture content of Mucoadhesive buccal patch may affect the release of Deflazacort from it. Relatively “dry” patch may need more time to release the drug. Hence, these tests were performed to evaluate the ability of patch to lose and to gain the moisture. From results it was found that the moisture content and moisture uptake of Mucoadhesive buccal patch changes significantly with change in its HPMC (hydrophilic polymer) content. It was found that there is direct relation between moisture content of patch and its HPMC content. This is because HPMC already have high moisture content. Moisture content and moisture uptake studies indicated that the increase in the moisture uptake may be attributed to the hygroscopic nature of the polymer composite patch. The moisture content of the prepared formulations was low, which could help the formulations remain stable and reduce brittleness during long term storage. The moisture uptake of the formulations was also low, which could protect the formulations from microbial contamination and reduce bulkiness. The weight lost by patches due to loss of moisture is shown in following table 13.

Table 13: Moisture content of Mucoadhesive buccal patch
* All values are mean±SD (n=3)
Percentage of moisture uptake
The water uptake or absorption behaviour of the Mucoadhesive buccal patch plays an important role at the beginning stage of drug release from dosage form Thus, the patch with higher moisture uptake supposed to give higher drug release rate initially. The moisture uptake of the formulations was also low, which could protect the formulations from microbial contamination and reduce bulkiness. The weight gain of patch due to exposure to moisture is shown in following table 14.

Table 14: Moisture uptake by Mucoadhesive buccal patch
* All values are mean±SD (n=3)
Differential scanning calorimetry (DSC)
The DSC curve of Deflazacort shows a single endothermic peak corresponding to the melting event of the substance in the range between 252 – 258°C. The DSC curve of Deflazacort was illustrated in Figure 6.

Figure 6: Differential Scanning Colorimetry (DSC) thermogram of Deflazacort
In- vitro dissolution studies
Table shows % drug release for all batches and Figure 12 show the release pattern for each batch.

Table 15: Percent Release of Deflazacort Mucoadhesive buccal patch
Table continue…

Figure 7 show the release pattern of Deflazacort from buccal patch in in vitro dissolution studies.

Figure 7: Percent Drug release for batches B1-B9
Drug release from polymer matrix and drug dissolution ensured sustained reproducibility of rate and duration of drug release. In vitro drug dissolution studies of the Mucoadhesive buccal patch were conducted using a Franz diffusion cell apparatus and phosphate buffer (pH7.4) as dissolution fluid. From results, it was found that that batch B2 showed highest drug release (97.67 ± 0.2%) and the lowest release was from batch B6 (83.74 ± 0.2%). The drug release was found to decrease with decrease in HPMC content up to some time period. The hydrophobic polymer EC retards the release of drug from matrix.
In vitro skin permeation studies
The in vitro permeation of Deflazacort of formulation B2 through chicken skin is shown in table 16 below. The flux and permeability coefficient are also shown.

Figure 8: in vitro permeation of Deflazacort through Franz diffusion cell

Table 16: Permeability parameters Deflazacort in Batch 2

Figure 9: In vitro permeation study of Mucoadhesive buccal patches of DFZ
Stability study of Mucoadhesive buccal patch
In view of the potential utility of B2 formulation for targeting of Deflazacort to skin, stability studies were carried out. After storage the formulation was subjected to evaluation of physical parameters, drug content studies.

Table 17: Stability data of Deflazacort Buccal Patches
CONCLUSION
Present study aimed to formulate and evaluate Mucoadhesive Buccal patch of Deflazacort (DFC). The Mucoadhesive Buccal patch of DFC was prepared successfully using solvent evaporation technique. The incorporation of HPMC and EC in the buccal patch formulation has demonstrated substantial improvements in mucoadhesive strength, allowing for prolonged residence time and intimate contact with the buccal mucosa. This enhanced adhesion facilitates sustained drug release and improved drug absorption, potentially leading to enhanced therapeutic efficacy. The inclusion of glycerol as a plasticizer has contributed to the flexibility and mechanical integrity of the buccal patch, ensuring ease of application and comfortable wearability for the patient. Additionally, glycerol aids in maintaining the hydration of the patch, promoting mucoadhesion and drug release at the site of application. All formulations showed satisfactory properties like thickness, weight, tensile strength, folding endurance, flatness, etc. Moisture content and moisture uptake varied with variation in HPMC & EC content. The in vitro dissolution study of patches showed release in the range 83.74± 0.2% - 97.67± 0.2%. Varying amount of HPMC and EC were found to be responsible for this variation in release. Permeation of DFC through chicken skin also changes with change in amounts of HPMC. The formulation batch 2 (B2) was studied for drug permeation in vitro skin permeation study. The permeation of DFC from chicken skin was found up to 62.47± 0.2%. Hence, it can be concluded that Mucoadhesive Buccal patch of Deflazacort with HPMC: EC polymeric system, Glycerol as plasticizer is an effective drug delivery system for buccal administration of DFC.
FUNDING
There was no external funding received for this research.
DECLARATION OF CONFLICT
The authors declare that there are no conflicts of interest related to this study.
AUTHOR CONTRIBUTION
All authors contributed equally to the research and the preparation of the manuscript.
REFERENCE


Pooja Dandge, Vinayak Mundhe, Formulation and Evaluation of Mucoadhesive Buccal Patches of Deflazacort, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 10, 550-565. https://doi.org/10.5281/zenodo.13919669
 10.5281/zenodo.13919669
10.5281/zenodo.13919669
