Department of Pharmaceutics, The Oxford College of Pharmacy, 1st Cross, Hongasandra, Bengaluru, Karnataka 560068.
This paper reviews the advantages, disadvantages, methodologies, evaluation, advancements and applications of transdermal drug delivery system (TDDS). which includes the concept of controlled release, permeation enhancers, Approaches for development of TDDS.
Transdermal medication delivery refers to self-contained, distinct dosage forms that, when utilized for undamaged skin, allow the drug to enter the systemic circulation at a regulated pace. One crucial element of innovative drug delivery systems is the transdermal drug delivery system (TDDS)1
II. Advantages of Transdermal Drug Delivery:
III. Disadvantages of Transdermal Drug Delivery System:4
IV. Skin Is a Site for Drug Infusion:
A third or so of the blood that circulates travels via the skin throughout the body, which has a surface area of two square meters on average for an adult. The epidermis is a complex organ with numerous histological layers. The epidermis, dermis, and hypodermis are the three main tissue layers that are frequently used to characterize it. Under a microscope, The skin's outermost layer is further separated into five anatomical layers, with the corneum stratum acting as the outermost layer that is exposed to the outside world.5

Fig.1 Structure of Human Skin Showing Epidermis, Dermis and Hypodermis.
According to estimates, every square centimeter of human skin has between 40 and There are 200 hair follicles and 70 to 250 sweat ducts. However, in reality these parts of the skin make up a pitiful 0.1% of the whole surface of the human skin.6 This trans-appendage At steady state, the percutaneous absorption route contributes very little to the overall kinetic profile of Permeation via the skin despite the fact that the foreign agents, especially the ones that dissolve in water, may be able to penetrate the skin via These parts of the skin at a pace that surpasses that of the whole region of the stratum corneum. Consequently, most of neutral chemicals transdermal Penetration may be viewed as a passive diffusion process via the interfollicular region's complete stratum corneum.7 Therefore, a basic multilayer model can be used to represent the different layers of skin tissue for the sake of the mechanistic investigation of transdermal medication infusion. When systemically active medications are administered topically, the substance will be absorbed, first going into the bloodstream and subsequently reaching the intended tissues.8
V. Physicochemical Properties for A Drug Candidate for Transdermal Delivery9
Table I
Desirable physicochemical properties for a drug candidate for transdermal delivery
|
Physicochemical Properties |
Desirable Characteristic |
|
Molecular weight (MW) |
Low MW, typically<500 Daltons. |
|
Daily Dose |
A low dose, ideally<20mg/day (most marketed products are for low-dose drugs). |
|
Lipophilicity (Log P) |
Optimal log P (octanol-water partition coefficient) in the range of 1-3 |
|
Solubility |
Must be adequately soluble in both water and oil to navigate the lipophilic stratum corneum and the underlying aqueous layers. |
|
Melting point |
Low melting point, typically <200?, which favours solubility in the skin’s stratum corneum. |
|
Ionization |
Preferably non-ionic, as only the unionized form of the drug can permeate the lipid barrier in significant amounts. |
VI. Basic Components Of TDDS:10
The foundation of TDDS is composed of polymers, which regulate the drug's release from the apparatus. Drugs can be dispersed either as a liquid or solid synthetic polymer bases to create polymer matrices. The polymers in TDDS ought to be chemically and biocompatible with the medication and other system elements including PSAs and penetration enhancers. They ought to be safe and distribute a drug consistently and effectively for the duration of the product's stated shelf life.11 A small number of selective polymeric systems are the focus of distribution through the skin companies. For instance, Searle Pharmacia focuses on silicon rubber, while Alza Corporation mostly works with microporous polypropylene or ethylene vinyl acetate (EVA) copolymers. Similarly, Sigma employs ethyl cellulose for isosorbide dinitrate matrix while Colorcon, HPMC is used in the UK for matrix preparation for transdermal distribution of propranolol. The In TDDS, polymers are utilized fall into the following categories:12
As matrix formers for TDDS, polymers such as hydroxypropylmethylcellulose, ethyl cellulose, polyvinylpyrrolidone, eudragits, and cross-linked polyethylene glycol are employed. As rate-controlling membranes, other polymers such as silicon rubber, polyurethane, and EVA are employed.
For medications with the right pharmacology and physical chemistry, the transdermal route is a very alluring choice. Drugs with a limited therapeutic window, high first pass metabolism, or short half lives that result in noncompliance from frequent doses can benefit greatly from transdermal patches. The primary prerequisite for transdermal drug delivery (TDDS) is that the medicine has the necessary combination of biological and physicochemical characteristics.13 The best Potential medications for transdermal patches with passive adhesive are typically believed to require non-ionic properties, a low molecular weight (less than 500 Daltons), be potent (dose in mg per day), have a low melting point (less than 200°C), be adequately soluble in water and oil (log P in the range of 1-3), and be non-ionic. The drugs that are already available for transdermal administration. Furthermore, medications such as selegiline for depression, methylphenidate for hyperactivity and attention deficit disorder, rotigotine for Parkinson's disease, and rivastigmine for Alzheimer's and Parkinson's dementia have recently been licensed as TDDS.14
Three routes- polar, non-polar, and polar/nonpolar- are proposed for drug penetration via the skin. One of these routes is changed by the enhancers. The key to changing the polar route is to induce solvent swelling or a change in protein structure. Modifying the lipid structure's stiffness and fluidizing the crystalline channel- which significantly boosts diffusion—are the keys to changing the nonpolar pathway. The fatty acid enhancers make the lipid layer of the stratum corneum more fluid. Certain enhancers (binary vehicles) change the multilaminate pathway for penetrants, which affects both polar and nonpolar pathways. Enhancers can dissolve skin lipids or denaturize skin proteins to improve medication diffusivity in the stratum corneum (SC). The design and development of the product are significantly impacted by the sort of enhancer used. The ability of the medicine to permeate the skin in enough amounts to have the intended therapeutic effect is necessary to the effectiveness of dermatological drug treatments designed for the administration of drugs systemically, such as transdermal. The techniques used to alter the SC's barrier qualities in order to improve drug penetration (and absorption) via the skin fall into two categories:
A PSA is a material that aids in preserving close contact between the skin's surface and the transdermal system. It should be aggressively and persistently tachy, exert a strong holding force, and adhere with little more pressure than is applied with the fingers. It should also be able to be removed without causing any residue from the smooth surface. In TDDSs, silicon-based adhesives, polyacrylates, and polyisobutylene are frequently utilized. The medicine composition and patch design are two of the many considerations that go into choosing an adhesive. An unintentional interaction between the glue and the drug and penetration enhancer in matrix systems with a Adhesive peripheral shouldn't result in instability for either of them. The diffusing medicine must not interfere with the face adhesive in reservoir systems that have one. The selection process for drug-in-adhesive matrix systems will be determined by how quickly the drug and penetration enhancer diffuse through the adhesive. PSA should ideally not change drug release and be compatible with physic-chemical and biological processes.
The most crucial factor to consider When making a backing layer, the substance's chemical resistance. Compatibility of the excipients should also be taken into account because extended interaction between the excipients and the layer of backing may result in the spread of excipients , drugs, or penetration enhancers through the stratum or the additives leaking away from the support layer. Over emphasizing chemical resistance, however, can result in stiffness and excessive occlusiveness to air and moisture vapour, which can cause patches to remove and potentially irritate the skin over time. The backing with the lowest modulus or high flexibility, healthy oxygen transfer, and A high rate of transfer of moisture vapour will be the most comfortable. Vinyl, polyester films, and polyethylene are a few examples of backing materials.
The protective lining that covers The patch while being stored is taken off and discarded right before the patch is utilized in the skin. Consequently, it is considered to be One element of the main packing material rather than the drug delivery dosage form. The liner must, however, meet certain standards for chemical inertness and permeability to the drug, penetration enhancer, and water because it comes into intimate contact with the delivery system. A release liner usually consists of a silicon or teflon release coating layer and a base layer that can be either occlusive (like paper fabric) or nonocclusive (like polyethylene or polyvinyl chloride). Metallized laminates and polyester foil are other materials utilized for the TDDS release liner.
Drug reservoirs are prepared using a variety of solvents, including Methanol, acetone, dichloromethane, isopropanol, and chloroform. To provide the transdermal patch flexibility, plasticizers such dibutylpthalate, triethylcitrate, polyethylene glycol, and propylene glycol are also included.
VII. Approaches to Development Transdermal Therapeutic Systems:20
To enable rate control over medication release and transdermal penetration, a Many technologies have been created using success. These technologies fall under the following four categories:
A shallow compartment made of a drug-impermeable metallic plastic laminate and a rate-controlling polymeric membrane—which may be microporous or non-porous—encloses the drug reservoir in this kind of device. Only through the rate-controlling polymeric membrane are the medication molecules allowed to release. The drug Particles are either evenly spaced or in a solid polymer matrix (like polyisobutylene adhesive) or suspended in a viscous, unbleachable liquid medium (like silicon fluids) to create a paste-like suspension in the drug reservoir compartment.21

Fig.2 Membrane -Moderated Transdermal Drug Delivery Systems.
By altering the polymer composition, permeability coefficient, and the thickness of the adhesive and rate-limiting membrane. The rate at which medications are discharged from this kind of system can be customized. The main benefit of a membrane permeation regulated system is the drug's steady release rate. However, there is also a rare chance that dose dumping or the quick release of the full drug content could occur from an unintentional rupture of the rate-controlling membrane. Instances of this system include:
A Transdermal device that releases Nitro-glycerine is used to treat angina pectoris once day.
Scopolamine – transdermal system release for seventy-two hours. preventing motion sickness.
Transdermal clonidine-releasing device for seven-day hypertension treatment.
A transdermal system that releases estradiol to treat menopausal symptoms for three to four days. Controlled absorption through the skin of prostaglandins derivatives has also been completed using the membrane permeation-controlled method.
A streamlined version of the membrane permeation-controlled system is this one. In order to establish a thin layer of drug reservoir, the drug is first dispersed in an adhesive polymer, such as poly (isobutylene) or poly (acrylate) adhesive, and then the medicated adhesive is applied, either by solvent casting or hot melt, to a flat sheet of drug-impermeable metallic plastic backing. To create an adhesive diffusion-controlled delivery system, thin coatings of a rate-regulating, non-medicated sticky polymer with a certain permeability and consistent thickness are put above the medication reservoir layer.
Makes isosorbide dinitrate available for use as a once-daily angina pectoris treatment.
Helps treat angina pectoris by delivering nitro- glycerine.

Fig.3 Adhesive Diffusion- Controlled Transdermal Drug Delivery Systems.
By uniformly spreading the hydrophilic or hydrophilic medication particles lipophillic polymer matrix, this method creates the drug reservoir. A disc with medication and a specified surface area and regulated thickness is then formed from the resulting medicated polymer. Drug particles can be dispersed in the polymer matrix by either mixing a rubbery polymer with medication solids uniformly at a high temperature or by combining a liquid polymer with the finely ground drug particles or a highly viscous base polymer and then cross-linking the polymer chains. Another method for creating the drug reservoir is to dissolve the drug and the polymer in a common solvent, then let the solvent evaporate in a Mold at a high temperature or under a vacuum. Then, in a compartment made of a drug-impermeable plastic backing membrane, this drug reservoir with polymer disc is adhered to an occlusive base plate. As was previously mentioned in the first two types of transdermal delivery methods, the sticky polymer is applied around the patch to create an adhesive ring around the medicated disc rather than directly on the disc's surface. For instance. Nitro-Dur: Treats angina pectoris by delivering nitro-glycerine.
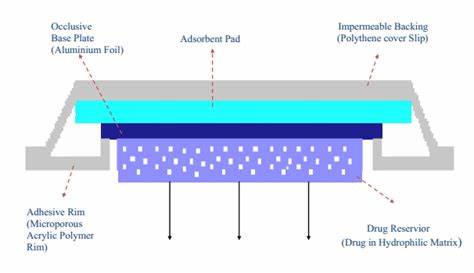
Fig.4 Matrix diffusion controlled Transdermal drug delivery system
The medication delivery system in the form of a micro reservoir can be considered as a hybrid of the matrix diffusion and reservoir types. This method involves first suspending the drug solids in an aqueous solution of a water-soluble liquid polymer (like polyethylene glycol), and then using a high energy dispersion technique to disperse the medication equally suspension in lipophillic polymers, such as silicone elastomers, to create a number of distinct, impermeable microspheres of drug reservoirs. Cross-linking the polymer chains in-situ instantly stabilizes This unstable thermodynamic dispersion, resulting in a polymer disc with medication a fixed thickness and constant surface area.The medicated disc is then positioned in the center and encircled by a ring that is sticky to provide a transdermal treatment system Nitro-glycerine, for instance: launching a transdermal therapy device to treat angina pectoris once daily.
VIII. Evaluation of Transdermal Films:23
In vitro studies play a major role in the design and creation of transdermal medication delivery systems. Prior to developing a transdermal treatment system, in vitro research can aid in examining the drug's mechanism skin penetration. The in vitro study's technique is comparatively simple to follow and typically gives the researcher more control over the experimental circumstances than in vivo. When choosing an in vitro system, the following elements need to be taken into account
Here, membrane hydration and the presence of penetration enhancers might be crucial. Examining the time course for the drug's penetration through a newly removed skin placed on a diffusion cell, like the Franz diffusion cell, allows for a more accurate analysis of the kinetics of skin penetration. Certain flaws in the Franz cell have been identified by Keshary and Chien, who have made modifications to bring the model closer to in vivo circumstances. Some diffusion cells are designed to hold the skin at a vertical position between donor and receptor chambers. The valia, Chien cell is a more contemporary example. It is better than similar older models because it prevents solvent loss from either phase and does not expose the donor and receptor phases to the same temperature. Additionally, the design gets around another drawback of the Franz cell, which is that its donor phase is sensitive to variations in the surrounding temperature. Lastly, it is possible to agitate the contents of the donor compartment, which qualifies the cell for transdermal medication delivery from suspensions and solutions. The literature has documented a variety of in vitro devices for assessing drug penetration characteristics through the skin. As seen below, they can be roughly divided into two groups.24
Diffusion cell physical design:
Method of Sampling and Measurement:
1. Membrane:25
2.Donor Compartment:25
3.Receptor Fluid:
Animal skins, such as hairless mice, guineas, rabbits, etc., are used in the majority of in vitro research. Despite these similarities, there is yet no animal skin that perfectly replicates the penetrating characteristics of human skin.
It is possible to perform an in-vivo evaluation of TDDS employing
In vivo animal there has been a preference for models and Resources are needed in order to carry out studies in humans. Some of the animals that have been used for in vivo testing are, rabbit, guinea pig, rat, mouse, hairless mouse, hairless rat, hair less dog, cat, dog, miniature pig, monkey, chimpanzee, rhesus monkey, horse, goat, squirrel, etc. To find out which animal models best anticipate how the technology under test will behave in people, a number of trials have been conducted.
After the transdermal device is applied to human volunteers, pharmacokinetic and pharmacodynamic data must be gathered as the last step in the development process. In a fair amount of time, an in vivo evaluation involving human subjects should provide relevant information with the least amount of risk to the subjects. Percutaneous absorption is measured indirectly by measuring radioactivity in excreta after topical administration of the labeled medication in human models for in vivo study. Typically, radio-labelling uses 14C. The amount of radioactivity that is retained in the body or expelled through unmonitored channels must be understood by the investigator in order to determine absorption after topical delivery. This calls for the dose absorbed to be measured. However, this strategy has a number of drawbacks. Several There have been attempts to address these issues. Below is a description of these,
Using this technique, the skin is exposed to the (radio-labeled) compound under investigation for a brief period of time. After that, tape stripping is used to remove the stratum corneum and the compound's content in the stratum corneum is analyzed. The amount of medicine that will permeate over an extended length of time can be predicted using this analysis.
This technique entails covering the application site with an occlusive chamber and replacing it with a new one after a predetermined amount of time. During these periods, the site is also washed. In addition to using radio-labeling techniques, the patients' faces, urine, chambers, and washings are analyzed. Using surface wash measurements to anticipate percutaneous absorption and achieving mass balance between the administered dose and excretion levels are two advantages of this technique.
The literature has described models based on linear kinetics, the solution of Fick's second law of diffusion for the device, stratum corneum, and viable epidermis, as well as the steady-state mass balance equation. There is need for improvement despite the fact that numerous methods for evaluating transdermal systems in vivo have been proposed. The skin's barrier function as we age, skin metabolism, penetration enhancers' in-vivo operation, etc. are some of the unsolved problems.
IX. Applications of Transdermal Patches:28
The nicotine patch, which helps people quit smoking tobacco by releasing nicotine in controlled dosages, is the most popular transdermal patch in the US.
X. Transdermal Market Product:29
For the foreseeable future, the transdermal product industry is anticipated to maintain its notable increasing trend. Around the world, a growing quantity of TDD goods are still providing patients with genuine therapeutic benefits. Approximately 16 active Compounds are permitted for use in TDD products worldwide, and over 35 TDD products are now authorized for sale in the US.
Table II
Examples Of Currently Marketed Transdermal Patches
|
Drug Name |
Brand Name Examples |
|
Fentanyl |
Duragesic®, Fentanyl patch |
|
Nicotine |
Nicoderm CQ®, Habitrol |
|
Clonidine |
Catapres-TTS® |
|
Buprenorphine |
Butrans® |
|
Scopolamine |
Transderm-Scop® |
|
Nitroglycerin |
Minitran®, Nitro-Dur® |
|
Rivastigmine |
Exlen® |
|
Oxybutynin |
Oxytrol® |
|
Testosterone |
Androderm® |
XI. Advance Developments In TDDS:30
Adhesives and excipients are the subject of two formulation research topics. Drugs in adhesive technology have become the preferred approach for passive transdermal distribution. The primary objective of adhesive research is to tailor the adhesive to improve skin adhesion over time, improve drug stability and solubility, reduce lag time, and expedite delivery. Since there isn't a single adhesive that works for all medicine and formulation chemistries, the transdermal formulator can optimize the effectiveness of the transdermal patch by customizing the adhesive chemistry. Over the past ten to fifteen years, research has been successful in developing transdermal technologies that use mechanical energy to increase the drug flux over the skin by either altering the stratum corneum, the skin barrier, or increasing the energy of the drug molecules. Thermal energy, electroporation (which uses short high voltage electrical pulses to create temporary aqueous pores in the skin), sonophoresis (which uses low frequency ultrasonic energy to disrupt the stratum corneum), and iontophoresis (which uses low voltage electrical current to drive charged drugs through the skin) are some of these so-called "active" transdermal technologies. (which increases the energy of drug molecules and increases skin permeability by using heat). Magnetophoresis, or magnetic energy, has also been researched to enhance drug flux across the skin.
CONCLUSION:
For the research scientist working on TDDS, the TDDS review papers offer useful information about transdermal drug delivery systems and the specifics of its evaluation procedure. The a fore mentioned demonstrates the immense potential concerning TDDS, which might be used to create promising deliverable pharmaceuticals with both hydrophobic and hydrophilic active substances. More knowledge of the various biological interaction processes and polymers is needed to optimize this drug delivery technology. TDDS is a viable, real-world use case for the next drug delivery technology.
REFERENCES




Karthik M., Gururaj S. K. Kulkarni, Vikram Choudhary*, Dr. Anna Balaji, Transdermal Drug Delivery System: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2936-2950 https://doi.org/10.5281/zenodo.17461180
 10.5281/zenodo.17461180
10.5281/zenodo.17461180
