Shraddha Institute of Pharmacy, Washim, Maharashtra, India.
This study explores the prevalence, clinical characteristics, and management approaches of thyroid disorders, with a primary focus on hypothyroidism and hyperthyroidism, across diverse patient populations. By analyzing patient data—including demographics, symptom profiles, and comorbid conditions—the research underscores both the widespread nature and the intricate presentation of thyroid dysfunction. Key risk factors such as iodine deficiency, autoimmune diseases, certain medications, and lifestyle influences are also examined. The study emphasizes the critical importance of early detection, patient awareness, and appropriate therapeutic interventions to minimize long-term complications and enhance clinical outcomes.
Thyroid disorders are among the most common endocrine conditions worldwide, affecting individuals across all age groups and health backgrounds. The thyroid gland plays a pivotal role in regulating metabolism, growth, and development through the secretion of essential hormones. Dysfunction in this gland manifesting as hypothyroidism, hyperthyroidism, or autoimmune thyroid disease can result in significant physiological and metabolic disruptions. Vulnerable populations such as children, pregnant women, and the elderly are especially at risk. In these groups, thyroid imbalances may lead to developmental delays, pregnancy complications, or metabolic instability. Furthermore, thyroid disorders often coexist with other chronic conditions including diabetes mellitus, hypertension, and obesity, which can obscure diagnosis and complicate treatment strategies. This study investigates the distribution and clinical profile of thyroid disorders among varied patient groups, ranging from pediatric to geriatric populations and including individuals with comorbid conditions. By examining the symptomatology, diagnostic methodologies (such as biochemical assays and imaging), and therapeutic responses, this research aims to enhance understanding of thyroid pathology. Improved insight into these aspects is essential for timely diagnosis and effective management, ultimately contributing to better patient outcomes. Despite growing awareness and advancements in diagnostic techniques, cases of undiagnosed or mismanaged thyroid disease continue to surface, often with severe health consequences. Given that thyroid hormones impact nearly every nucleated cell in the body, precise diagnosis and management are imperative to avoid long-term systemic effects and ensure optimal health outcomes.
Thyroid Gland
The thyroid gland is an essential endocrine gland in the human body that plays a significant role in metabolism, growth, and overall body function.
Location of the Thyroid gland
The thyroid gland is a butterfly-shaped organ located in the front of the neck, just below the Adam’s apple (larynx) and along the trachea (windpipe). It consists of two lobes (right and left) connected by a thin strip of tissue called the isthmus. The gland wraps around the trachea and is highly vascularized, meaning it has a rich blood supply.(19)
Function of The Thyroid Gland
The thyroid is responsible for producing and regulating hormones that control various body functions including Metabolism How the body converts food into energy.
The thyroid gland is regulated by the hypothalamus and pituitary gland, which control hormone release through a feedback mechanism. (20)
Hormones Produced by the Thyroid Gland
The thyroid gland produces three main hormones
Regulation
The pituitary gland releases thyroid-stimulating hormone (TSH), which signals the thyroid to produce T3 and T4. The hypothalamus releases thyrotropin-releasing hormone (TRH), which stimulates the pituitary gland. (20) Small, bilobed structures located in the neck are called thyroid gland (20-25 g) secrets minor (7%) triiodothyronine and major (93%) thyroxin (T4) hormones from its follicles. It is clear from Guyton and Hall that the biological activity of T3 is 3-5 folds higher than T4. (24) Both of these are much similar to each other in holding two tyrosine amino acids. (22) The difference between these two is holding three iodine atoms in T3 and four iodine at-oms in T4 . The regulation of synthesis and secretion of T3 and T4 hormones is under the control of thyrotropin (also called thyroid stimulating hormone; TSH) released from the anterior pituitary, which is stimulated by tripped tide releasing hormone/thyrotrophic releasing hormone (TRH) from hypothalamus. Synthesis and regulation of triiodothyronine oxin from the thyroid gland (TG) Alamus AP Anterior Pituitary PP Posterior Pi-trophin Releasing Hormone TSH Thyroid Stimulating and denotes positive and negative regulation Distributed under creative commons license(23)
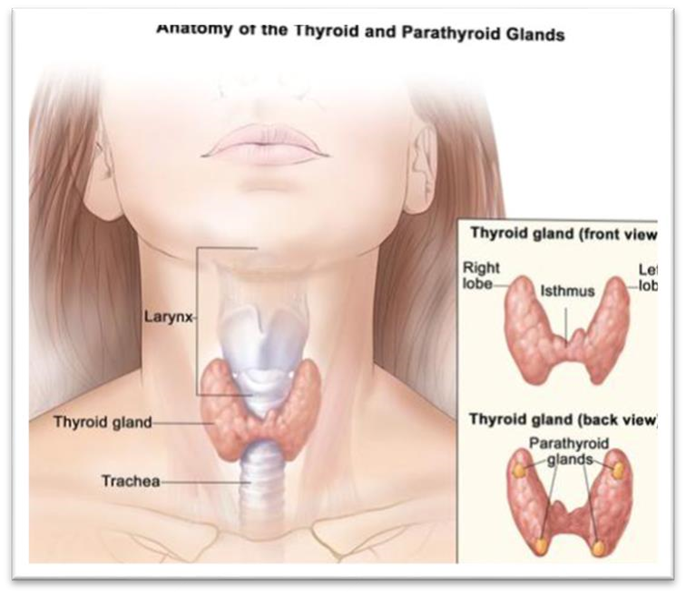
Fig No. 1 Thyroid Gland
Plan of Work
A literature review of thyroid studies in patients reveals a wide range of research focusing on various aspects of thyroid disorders. Association between Thyroid Disorders and Hyperprolactinemia Research has shown that thyroid disease, particularly hypothyroidism, is a significant cause of hyperprolactinemia. A systematic review of 47 articles found that 804 patients with this clinical association had distinct clinical characteristics, management, and outcomes.
Choose a study type (e.g., observational cohort study, cross-sectional study, or randomized controlled trial).Identify the study population (e.g.hyperthyrodisum and hypothyroidisms patients, age group, and ethnicity). Define inclusion and exclusion criteria (e.g., age range, co-morbidities, medication history). Select a sample size based on statistical power calculations. Develop ethical considerations (informed consent, patient privacy, ethical approval). (11)
Recruit participants Collaborate with hospitals, clinics, or diabetes care centers to recruit participants. Obtain patient consent Ensure ethical protocols are followed for obtaining informed consent from all participants Gather clinical data Collect baseline data on demographics (age, gender, ethnicity), medical history, lifestyle factors (diet, exercise), and current treatments. Measure thyroid levels Obtain thyroid levels at the start of the study (and at specified intervals if longitudinal).
Statistical tools Use statistical software (e.g. excel) for data analysis. Descriptive analysis: Calculate means, medians, and standard deviations of thyroid levels across different groups. Correlation analysis Perform correlation tests (e.g., Pearson’s or Spearman’s) to assess the relationship between thyroid and complications. Regression analysis: Use multiple regression analysis to identify significant predictors of thyroid levels (e.g., treatment type, demographic factors, lifestyle).Compare treatment groups: Analyze the impact of different treatment regimens (oral drugs, thyroid, lifestyle) on thyroid levels.
Contextualize finding Compare your findings with previous studies, particularly regarding the role of thyroid in complications and treatment outcomes. Discuss limitations Identify potential limitations of your study (e.g., sample size, biases, and measurement errors).Implications for clinical practice Discuss how the results can influence diabetes management, treatment strategies, and thyroid monitoring. (13)
Research assistants, statisticians, healthcare professionals (for recruitment and data collection).Facilities Hospitals or clinics for participant recruitment and testing. Funding Budget for research expenses, including participant compensation, lab tests, data analysis software, and publication fees. Equipment thyroid testing kits data analysis software and access to healthcare databases.
Ethical considerations are fundamental in ensuring that the rights, dignity, and welfare of individuals are respected in research, healthcare, and other professional practices. These considerations are guided by core principles such as respect for autonomy, beneficence, , justice, confidentiality, and integrity. Informed consent is a key ethical requirement that ensures individuals voluntarily agree to . The individual must fully comprehend this information, be competent to make the decision, and give consent without any form of pressure or coercion.(14)
Thyroid Study In Patients
|
Sr. No |
Age |
Gender |
Group |
Thyroid Type |
Conditions |
TSH ml(U/L) |
|
P001 |
37 |
F |
Adult |
Hyperthyroidism |
Hypertension |
2.26 |
|
P002 |
70 |
F |
Elderly |
Hypothyroidism |
None |
1.5 |
|
P003 |
40 |
F |
Adult |
Hyperthyroidism |
Type 2 Diabetes |
1.10 |
|
P004 |
71 |
F |
Elderly |
Hyperthyroidism |
Chronic kidney Disease |
7.62 |
|
P005 |
54 |
M |
Elderly |
Hypothyroidism |
None |
0.37 |
|
P006 |
17 |
M |
Adult |
Congenital Thyroid |
None |
1.28 |
|
P007 |
46 |
F |
Adult |
Hypothyroidism |
Asthma |
1.07 |
|
P008 |
44 |
F |
Adult |
Hypothyroidism |
Anemia |
6.78 |
|
P008 |
33 |
M |
Adult |
Hyperthyroidism |
Gastational Diabetes |
1.30 |
|
P009 |
55 |
F |
Elderly |
Hashimotos Disease |
None |
9.85 |
|
P010 |
50 |
F |
Elderly |
Hashimotos Disease |
None |
1.76 |
|
P011 |
37 |
F |
Adult |
Hyperthyroidism |
None |
4.56 |
|
P012 |
42 |
F |
Elderly |
Hyperthyroidism |
Hypertension |
16.55 |
|
P013 |
22 |
F |
Adult |
Hypothyroidism |
Types 2 Diabetes |
1.56 |
|
P014 |
60 |
M |
Elderly |
Hyperthyroidism |
PCOS |
2.53 |
|
P015 |
32 |
F |
Adult |
Hyperthyroidism |
Preclamp |
1.15 |
|
P016 |
61 |
F |
Elderly |
Hypothyroidism |
Coronary Artery Disease |
0.05 |
|
P017 |
50 |
F |
Elderly |
Hyperthyroidism |
Chronic kidney Disease |
2.26 |
|
P018 |
70 |
F |
Elderly |
Hypothyroidism |
Depression |
0.05 |
|
P019 |
61 |
F |
Elderly |
Hypothyroidism |
None |
11.81 |
|
P020 |
42 |
M |
Adult |
Hypothyroidism |
None |
18.71 |
|
P021 |
54 |
F |
Elderly |
Hypothyroidism |
Hypertension |
15.05 |
|
P022 |
49 |
M |
Elderly |
Hypothyroidism |
Chronic kidney Disease |
0.3 |
|
P023 |
59 |
F |
Elderly |
Hypothyroidism |
Type 2 Diabetes |
11.99 |
|
P024 |
62 |
M |
Elderly |
Goiter |
Asthma |
6.97 |
|
P025 |
47 |
F |
Adult |
Papillary thyroid |
Anemia |
1.51 |
|
P026 |
28 |
M |
Adult |
Hypothyroidism |
Hypertension |
0.2 |
|
P027 |
50 |
F |
Elder |
Hypothyroidism |
PCOS |
1.26 |
|
P028 |
55 |
F |
Elderly |
Hyperthyroidism |
Heart Failure |
9.85 |
|
P029 |
33 |
M |
Adult |
Goiter |
Heart Failure |
1.30 |
|
P030 |
44 |
F |
Adult |
Hashimotos Disease |
Asthma |
6.78 |
|
P031 |
46 |
F |
Adult |
Hyperthyroidism |
Types 2 Diabetes |
1.07 |
|
P032 |
17 |
M |
Adult |
Goiter |
Hypertension |
1.28 |
|
P033 |
5 |
F |
Children |
Hypothyroidism |
Types 2 Diabetes |
11.48 |
|
P034 |
11 |
M |
Children |
Graves Disease |
Chronic kidney Disease |
0.04 |
|
P035 |
54 |
M |
Elderly |
Hashimotos |
Hypertension |
0.37 |
|
P036 |
38 |
M |
Adult |
Hypothyroidism |
PCOS |
156 |
|
P037 |
50 |
F |
Elderly |
Goiter |
Types 2 Diabetes |
0.3 |
|
P038 |
71 |
F |
Elderly |
Hypothyroidism |
Heart Failure |
7.62 |
|
P039 |
53 |
M |
Adult |
Hypothyroidism |
Asthma |
0.08 |
|
P040 |
40 |
F |
Adult |
Hypothyroidism |
None |
1.10 |
Graphs
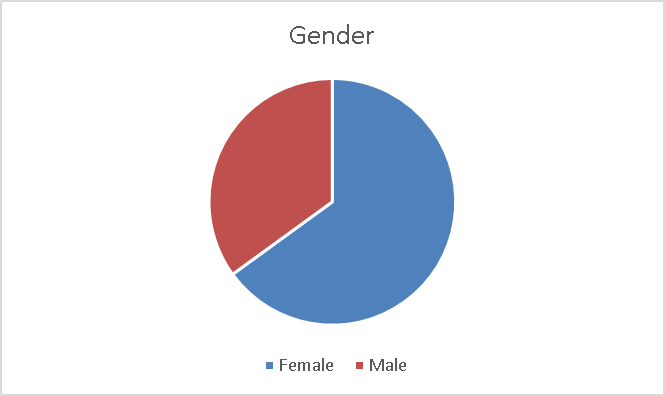
Graph No. 1 Graphical Representations of thyroid on the basis of Gender
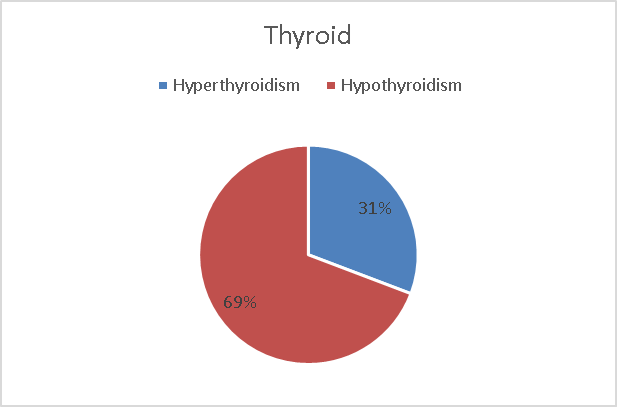
Graph No.2 Graphical Representations of thyroid on the basis of thyroid Level
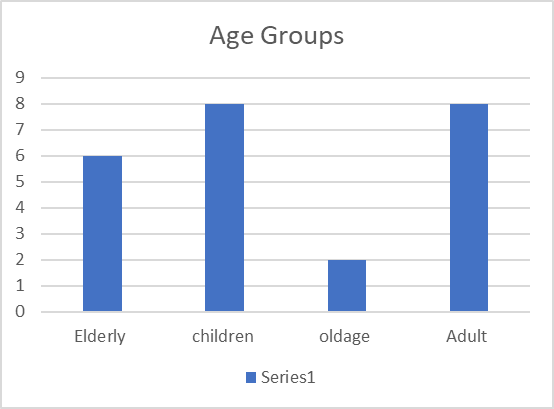
Graph No.3 Graphical Representations of thyroid on the basis of Age Groups
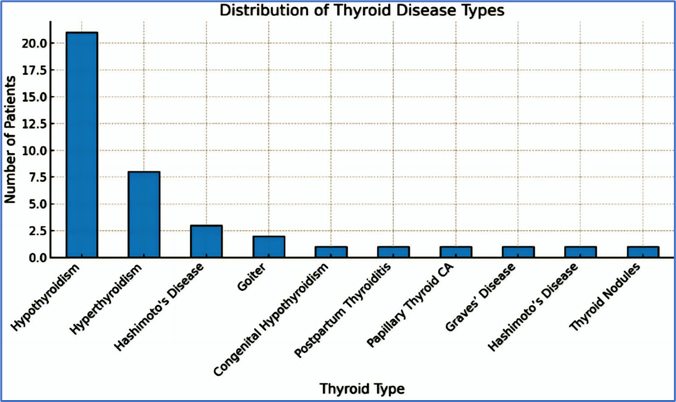
Graph No .4 Graphical Representations of thyroid on the basis of Different Thyroid Disorder
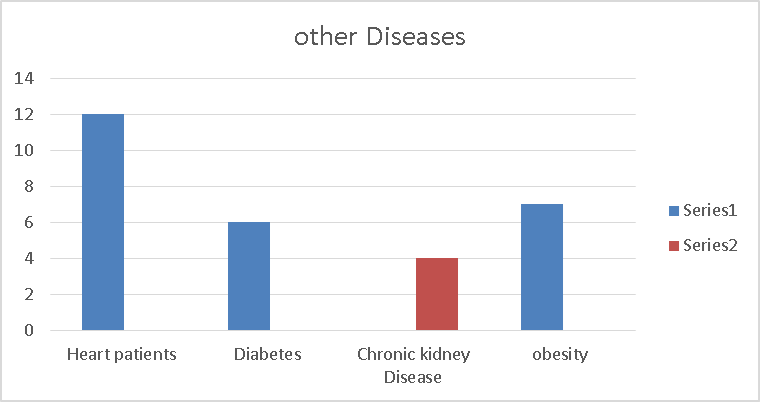
Graph No .5 Graphical Representations of thyroid on the basis on Other Diseases
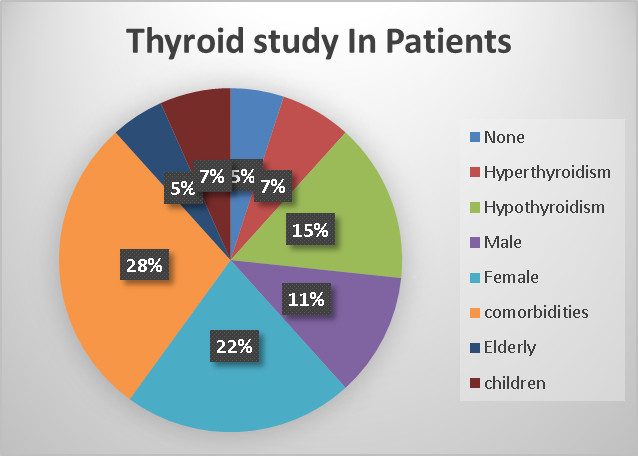
Graph No.6 Graphical Representations of thyroid
Factors Affecting Thyroid Levels
The function of the thyroid is influenced by a range of internal and external elements. These factors can impact the synthesis, release, transport, and metabolism of thyroid hormones, primarily thyroxine (T4), triiodothyronine (T3), and the regulatory hormone thyroid-stimulating hormone (TSH).
A deficiency in essential nutrients can lead to hypothyroidism and goiter, while an excess may result in autoimmune thyroiditis or hyperthyroidism. Selenium is crucial for the enzyme that converts T4 into the active form T3, and its deficiency can hinder thyroid function. Iron is necessary for the thyroid peroxidase enzyme; thus, iron deficiency (anemia) may diminish T3/T4 synthesis. Zinc and Vitamin D are important for regulating TSH and supporting immune function, with deficiencies linked to thyroid problems.
Hashimoto’s Thyroiditis leads to hypothyroidism due to the autoimmune destruction of the thyroid gland. Conversely, Graves’ Disease is an autoimmune disorder that causes hyperthyroidism through stimulation of the TSH receptor. The presence of thyroid antibodies (TPOAb, TgAb, TRAb) can affect hormone levels and the progression of the disease.(15)
Amiodarone, with its high iodine content, can induce hypo- or hyperthyroidism. Lithium can interfere with the release of hormones from the thyroid. Glucocorticoids, dopamine, and certain chemotherapy agents can suppress TSH secretion. Antithyroid medications, such as methimazole, are used to intentionally lower hormone levels in patients with hyperthyroidism.
During pregnancy, HCG can mimic TSH and stimulate the thyroid, often resulting in lower TSH levels in the first trimester. The increased demand for thyroid hormones during pregnancy can reveal underlying disorders. Hormonal changes during puberty and menopause also affect thyroid regulation. Additionally, TSH levels tend to rise with age, even in the absence of clinical thyroid disease.(16)
Both acute and chronic stress can alter the hypothalamic-pituitary-thyroid (HPT) axis, potentially leading to reduced T3 levels. Non-thyroidal illness syndrome (Euthyroid Sick Syndrome) can also impact thyroid function.
Thyroid Tests And Long Term Complications
Thyroid Tests
Thyroid function tests (TFTs) are essential for diagnosing, monitoring, and managing thyroid disorders. These tests evaluate the thyroid gland’s ability to produce hormones and assess the impact of thyroid conditions on the body. (17)
Primary screening test Produced by the pituitary gland stimulates the thyroid to produce T3 and T4 High TSH Suggests hypothyroidism (underactive thyroid) Low TSH Suggests hyperthyroidism (overactive thyroid) or pituitary dysfunction.
Measures unbound, biologically active T4 Low Free T4Hypothyroidism High Free T4
Hyperthyroidism
Active form of thyroid hormone. Especially helpful in diagnosing hyperthyroidism and T3 toxicosis. Useful alone in hypothyroidism evaluation (33)
Measures both bound and unbound hormone Affected by protein levels, so less accurate than free hormone levels.
Anti-TPO (Thyroid Peroxidase Antibodies) Common in Hashimoto’s thyroiditis Anti-Tg (Thyroglobulin Antibodies) May be present in autoimmune thyroid disease TRAb (TSH Receptor Antibodies)Seen in Graves’ disease
Assesses structure: nodules, goiter, cysts, inflammation. Helps guide fine needle aspiration (FNA) biopsy for suspicious nodules (34)
Measures iodine uptake by the thyroid Differentiates causes of hyperthyroidism (e.g., Graves’, toxic nodule)
Used to assess thyroid nodules for malignancy
Treatments And Therapies
Hypothyroidism Treatment
Hyperthyroidism Treatment
Thyroid Nodule and Cancer Treatment
Thyroid Hormone Replacement Therapy
Lifestyle Changes and Alternative Therapies
Thyroid Surgery
Radioactive Iodine (RAI) Therapy
Diagnostic Limitations
False Positives/Negatives in Lab Tests TSH Test Variability:
TSH levels can be affected by factors like age, pregnancy, medications (e.g., steroids, dopamine), or critical illness, leading to false positives or false negatives.
Subclinical hypothyroidism (elevated TSH with normal T4) may not necessarily progress to full hypothyroidism, complicating diagnosis.
Normal TSH with Symptoms
Euthyroid sick syndrome (low thyroid function in critically ill patients) can cause misleading results.
Thyroid antibodies: Even if present, they may not always correlate with disease severity (e.g., Hashimoto’s thyroiditis) and can be seen in healthy individuals. (25)
Thyroid Ultrasound
While useful for identifying nodules, it cannot definitively determine whether they are benign or malignant without biopsy.
Some benign nodules may still require monitoring for growth or functional changes.
RAI Uptake Scan
It may not be useful in certain populations (e.g., pregnancy, breastfeeding) or patients with iodine allergies.
Does not always provide clear answers in cases of thyroiditis or subacute thyroiditis.
Fine Needle Aspiration (FNA) Limitations
FNA is crucial for assessing thyroid nodules, but it is not always 100% accurate.
May yield indeterminate results that require further testing or repeat biopsy.
Risk of inadequate sample or sampling error. (28)
Hormone Replacement Therapy Challenges
Levothyroxine Therapy
Dosing The correct dose of levothyroxine may vary significantly across individuals, and adjustments are often required over time. It may take several months to find the optimal dose.
Drug Interactions Certain medications (e.g., calcium, iron supplements, proton pump inhibitors) can interfere with levothyroxine absorption.
Monitoring Regular blood tests (e.g., TSH levels) are required to adjust the dose, which can be burdensome for some patients.
Comorbidities Patients with cardiovascular disease or elderly patients may need lower starting doses to avoid strain on the heart. (33)
Antithyroid Drugs
Methimazole and propylthiouracil (PTU) can cause side effects, including rash, liver toxicity, and agranulocytosis (a serious condition involving a low white blood cell count).
These medications don’t offer a permanent cure and often require long-term use.
Radioactive Iodine Therapy
Post-treatment hypothyroidism is common, requiring lifelong levothyroxine replacement.
Pregnancy Not recommended during pregnancy or for a period after RAI treatment.
Risk of cancer: Rare, but there is a slight increased risk of developing other cancers following radiation therapy.
Thyroid Surgery
Surgical risks include bleeding, infection, and damage to the recurrent laryngeal nerve (which controls the vocal cords) leading to hoarseness. (39)
Lifelong hormone therapy may be required after total thyroidectomy, and some patients may need regular follow-up for recurrence or metastasis in cases of cancer.
Pregnant Women
Uncontrolled thyroid disorders during pregnancy (especially hypothyroidism and hyperthyroidism) can lead to complications like miscarriage, preterm birth, and fetal development issues. Medication adjustments are often necessary, especially with levothyroxine (need for higher doses during pregnancy).
Thyroid dysfunction may be harder to detect due to the overlapping symptoms of pregnancy (fatigue, weight changes, mood swings).
Elderly Patients
Atypical Presentation: Symptoms of thyroid disorders may not present clearly in older adults, making diagnosis challenging.
Hypothyroidism may be mistaken for depression, dementia, or normal aging.
Hyperthyroidism can be confused with age-related conditions like atrial fibrillation, heart failure, or osteoporosis.
Co-morbidities: The presence of other medical conditions (e.g., heart disease, diabetes) can complicate the management of thyroid disorders. Dosing of thyroid medication may need to be adjusted carefully.
False-Negative FNA Results Even with FNA biopsy, there is a risk of false-negative results in thyroid cancer diagnosis, leading to a missed diagnosis.
Mental Health Both hypothyroidism and hyperthyroidism can affect mental health, leading to depression, anxiety, and cognitive dysfunction. (40)
Emerging Trends and Future Direction
The study of thyroid disorders across different types of patients has become highly specialized to account for variations based on age, gender, pregnancy status, comorbidities, and genetic background. In children, researchers are focusing on early detection and treatment of congenital hypothyroidism and autoimmune thyroiditis to prevent cognitive and growth impairments. In pregnant women, special attention is being given to subtle thyroid dysfunctions that could affect both maternal health and fetal development, leading to efforts to refine universal screening and treatment guidelines. In the elderly, thyroid diseases often present with nonspecific symptoms, and studies are examining whether to treat mild dysfunctions to avoid overtreatment risks like heart rhythm problems. Gender-specific research continues to show that women are more vulnerable to autoimmune thyroid diseases, encouraging further studies into hormonal and immune system interactions. In cancer patients, research is moving toward identifying molecular and genetic markers to detect thyroid malignancies earlier and guide personalized treatments. Moreover, the relationship between thyroid function and chronic illnesses like diabetes and heart disease is being intensively studied to better manage patients with multiple health issues. Ethnic, racial, and genetic studies are expanding, aiming to explain disparities in disease prevalence and outcomes among different populations.
Future directions
In thyroid research are highly promising and focused on precision medicine, with genetic profiling expected to become a routine part of diagnosis and management. There is a growing interest in developing non-invasive diagnostic methods, such as advanced imaging and liquid biopsies using blood-based biomarkers. Artificial intelligence (AI) and machine learning are being incorporated to predict disease progression and optimize individualized treatment plans. Immunotherapy, already a breakthrough in cancer treatment, is also being explored for thyroid cancers and autoimmune thyroid conditions. The role of the microbiome (gut-thyroid axis) is emerging as a new frontier, with future therapies potentially targeting gut health to manage thyroid dysfunction. Additionally, environmental research is expected to deepen, investigating how pollutants and endocrine disruptors contribute to rising rates of thyroid disease.
RESULT AND DISCUSSION
Analysis of Thyroid Patient Data
The provided data includes 40 patients with various thyroid conditions, including hyperthyroidism, hypothyroidism, Hashimoto’s disease, and goiter. The data also includes demographic information, such as age and sex, as well as comorbidities like hypertension, type 2 diabetes, and chronic kidney disease.
DISCUSSION
The data suggests that thyroid disorders are more prevalent in elderly females. Hypertension and type 2 diabetes are common comorbidities, which may be related to the thyroid condition or age. The data also highlights the importance of monitoring and managing thyroid disorders, particularly in elderly patients with comorbidities. Further analysis and research would be needed to draw more specific conclusions.
REFERENCES


Gayatri Apotikar*, Shubham Tikait, Swati Deshmukh, Thyroid Study in Patients, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 4028-4042. https://doi.org/10.5281/zenodo.15505489
 10.5281/zenodo.15505489
10.5281/zenodo.15505489
